Download as docx, pdf, or txt
You might also like
- SoCal's UW Step 2 CK EOs (UTD 10 Nov)Document292 pagesSoCal's UW Step 2 CK EOs (UTD 10 Nov)JJ0% (1)
- Creating Vibrant EcosystemDocument7 pagesCreating Vibrant Ecosystem周一行No ratings yet
- Prognostic TestsDocument3 pagesPrognostic TestsHANS BENNo ratings yet
- Structured Reading of Articles (PICO)Document2 pagesStructured Reading of Articles (PICO)Cholis Nur AiniNo ratings yet
- Keller2002 PDFDocument10 pagesKeller2002 PDFFatymah Azzahra RirinNo ratings yet
- Ed Triage ReviewDocument13 pagesEd Triage ReviewTheala RadistaNo ratings yet
- Example Systermatic Review and Narrative SynthesisDocument11 pagesExample Systermatic Review and Narrative SynthesisTamsin Athalie NicholsonNo ratings yet
- 2 Art Ingles IJA-67-39Document9 pages2 Art Ingles IJA-67-39Vanesa Osco SilloNo ratings yet
- Clinical Decision Support System PDFDocument9 pagesClinical Decision Support System PDFJieshun WangNo ratings yet
- Trauma Scores: A Review of The Literature: ArticleDocument8 pagesTrauma Scores: A Review of The Literature: ArticleXenia PopovNo ratings yet
- Vgi FX CaderaDocument8 pagesVgi FX CaderaLuz Veronica Taipe MorveliNo ratings yet
- Early Warning ScoreDocument7 pagesEarly Warning ScoreDaniello RahanrNo ratings yet
- Measuring Explicit Prospective Payment: Quality SystemDocument5 pagesMeasuring Explicit Prospective Payment: Quality Systemsolxmar tmNo ratings yet
- Medi 99 E20541Document3 pagesMedi 99 E20541wlNo ratings yet
- 2nd - Neelam Dhingra - WHO Patient Safety Assessments WHO HQ Documents July 2018Document3 pages2nd - Neelam Dhingra - WHO Patient Safety Assessments WHO HQ Documents July 2018David Rafael Cañez MartinezNo ratings yet
- Diagnostic Accuracy Measures: Methodological NotesDocument6 pagesDiagnostic Accuracy Measures: Methodological NotesFrontiersNo ratings yet
- Prognosis Worksheet CitationDocument4 pagesPrognosis Worksheet Citationanon_65353286No ratings yet
- Li 2020Document13 pagesLi 2020Nurul AidaNo ratings yet
- Template Evidence Tables: 1.1. Evidence Table of Systematic ReviewsDocument10 pagesTemplate Evidence Tables: 1.1. Evidence Table of Systematic ReviewsthelordhaniNo ratings yet
- Endorsement NotesDocument8 pagesEndorsement NotesAngel Marie BarquezNo ratings yet
- Template-Data Extraction Form - Cochrane Review Group Review GroupDocument13 pagesTemplate-Data Extraction Form - Cochrane Review Group Review GroupDiana DidiNo ratings yet
- OhnsDocument7 pagesOhnsDaniel AbomaNo ratings yet
- Warko Karnadihardja, Reno Rudiman: (Critical Appraisal of The Topics)Document53 pagesWarko Karnadihardja, Reno Rudiman: (Critical Appraisal of The Topics)yuyu tuptupNo ratings yet
- Researcher 4Document14 pagesResearcher 4Marimiel PagulayanNo ratings yet
- Early Warning Scores and Their Application in The Inpatient Oncology SettingsDocument10 pagesEarly Warning Scores and Their Application in The Inpatient Oncology SettingsNajwacitraazzahraNo ratings yet
- Rad Rle Students Guide Written Requirements Sem.2Document5 pagesRad Rle Students Guide Written Requirements Sem.2bekbekk cabahugNo ratings yet
- 1 s2.0 S0002961017313697 MainDocument10 pages1 s2.0 S0002961017313697 MainWialda Dwi rodyahNo ratings yet
- Decarvalho2020 CX Pancreas PedsDocument5 pagesDecarvalho2020 CX Pancreas PedsnutricionhiemiNo ratings yet
- Critical Appraisal HarmDocument5 pagesCritical Appraisal HarmRois HasyimNo ratings yet
- The Effect of CaregiverFacilitated Pain Management Interventions in Hospitalized Patients On Patient Caregiver Provider and Health System Outcomes A Systematic ReviewDocument60 pagesThe Effect of CaregiverFacilitated Pain Management Interventions in Hospitalized Patients On Patient Caregiver Provider and Health System Outcomes A Systematic ReviewRavikiran SuryanarayanamurthyNo ratings yet
- Emulating Randomized Clinical Trials With Non-Randomized Real-World Evidence StudiesDocument26 pagesEmulating Randomized Clinical Trials With Non-Randomized Real-World Evidence StudiesNational Press FoundationNo ratings yet
- Healthcare Professionals' Perceptions and Confrontations at Patients' End-Of-Life in Emergency Departments A Systematic ReviewDocument4 pagesHealthcare Professionals' Perceptions and Confrontations at Patients' End-Of-Life in Emergency Departments A Systematic ReviewGabriella MulèNo ratings yet
- RAD RLE Guide - Written RequirementsDocument5 pagesRAD RLE Guide - Written RequirementsAngelo MadjosNo ratings yet
- Oral Anticoagulant and Antiplatelet in PADDocument7 pagesOral Anticoagulant and Antiplatelet in PADHninNo ratings yet
- Effect of CDSSDocument20 pagesEffect of CDSSMia Md. RaihanNo ratings yet
- Presición de EcografíaDocument3 pagesPresición de Ecografíasamuelfdiaz.0103No ratings yet
- Analgesic Efficacy of Preoperative Dexketoprofen TrometamolDocument11 pagesAnalgesic Efficacy of Preoperative Dexketoprofen TrometamolzhuangemrysNo ratings yet
- Halkiadakis - A Prospective Assessment of Resilience in Trauma Patients Using The Connor-Davidson Resilience ScaleDocument6 pagesHalkiadakis - A Prospective Assessment of Resilience in Trauma Patients Using The Connor-Davidson Resilience ScaleBrittany Caroline BlackNo ratings yet
- Patient Safety To Prevent Bad Ulcer1sDocument19 pagesPatient Safety To Prevent Bad Ulcer1sMo7med YasserNo ratings yet
- Predicting 30-DayMortality For PatientsWith AcuteHeart Failure in The EmergencyDepartmentDocument14 pagesPredicting 30-DayMortality For PatientsWith AcuteHeart Failure in The EmergencyDepartmentRoberto López MataNo ratings yet
- Features and Explainable Methods For Cytokines Analysis of Dry Eye Disease in HIV Infected PatientsDocument12 pagesFeatures and Explainable Methods For Cytokines Analysis of Dry Eye Disease in HIV Infected PatientsAgil PambudiNo ratings yet
- Role of WRD in Establishing Clinical Evidece in Context of Regulatory FrameworksDocument16 pagesRole of WRD in Establishing Clinical Evidece in Context of Regulatory FrameworksNaqibullahNo ratings yet
- Menilai Jurnal (CAT)Document53 pagesMenilai Jurnal (CAT)Risya TheupstarNo ratings yet
- The Preoperative Cost of Carpal Tunnel Syndrome: PurposeDocument11 pagesThe Preoperative Cost of Carpal Tunnel Syndrome: PurposeRonal Zumaeta PortocarreroNo ratings yet
- Evidence Based Mecidine (Ebm) : Laporan PraktikumDocument6 pagesEvidence Based Mecidine (Ebm) : Laporan Praktikumlailatut toriqohNo ratings yet
- The Value of Preoperative Exercise and Education For Patients Undergoing Total Hip and Knee ArthroplastyDocument15 pagesThe Value of Preoperative Exercise and Education For Patients Undergoing Total Hip and Knee ArthroplastyemilNo ratings yet
- 2018 - Holger J Schünemann - GRADEguidelines18HowROBINSIandothertoolstoa...Document10 pages2018 - Holger J Schünemann - GRADEguidelines18HowROBINSIandothertoolstoa...zenenNo ratings yet
- Critical Appraisal PrognoseDocument5 pagesCritical Appraisal PrognoseRois HasyimNo ratings yet
- Epidemiologi Klinik & Evidence Based Medicine: Profesor DR, DR R.M. Suryadi Tjekyan DTM&H, MPHDocument69 pagesEpidemiologi Klinik & Evidence Based Medicine: Profesor DR, DR R.M. Suryadi Tjekyan DTM&H, MPHDamal An NasherNo ratings yet
- 2020 Terri Glioma PRODocument7 pages2020 Terri Glioma PRORimpa Basu AchariNo ratings yet
- Critical Appraisal - Therapy - APTDocument36 pagesCritical Appraisal - Therapy - APTJason LiberiNo ratings yet
- 10 1001@jamanetworkopen 2018 7053Document14 pages10 1001@jamanetworkopen 2018 7053Eka BagaskaraNo ratings yet
- Rehabilitation: I (EadDocument9 pagesRehabilitation: I (EadalizzxNo ratings yet
- Virtual Reality Tour To Reduce Perioperative AnxietyDocument8 pagesVirtual Reality Tour To Reduce Perioperative AnxietyFiorel Loves EveryoneNo ratings yet
- Diagnostic Errors in TelehealthDocument8 pagesDiagnostic Errors in TelehealthKarina AuliaNo ratings yet
- Cart Cardiac Arrest Risk TriageDocument8 pagesCart Cardiac Arrest Risk TriageAlexeiLópezCarbonellNo ratings yet
- Art 1Document7 pagesArt 1Hajji AhmedNo ratings yet
- Statisticial MedicineDocument16 pagesStatisticial MedicineAbhaya IndrayanNo ratings yet
- Critical Appraisal of The TopicsDocument13 pagesCritical Appraisal of The TopicsIntan Eklesiana NapitupuluNo ratings yet
- Long Night Shifts Among Health Workers and Physical and Mental Health: The Influence of On-Shift Nap and Domestic WorkDocument1 pageLong Night Shifts Among Health Workers and Physical and Mental Health: The Influence of On-Shift Nap and Domestic WorksicodaNo ratings yet
- RCS - Surgical LeadershipDocument12 pagesRCS - Surgical Leadershipyesakula30No ratings yet
- Marino Video StudyDocument3 pagesMarino Video Studyyesakula30No ratings yet
- Marino Case Matched StudyDocument13 pagesMarino Case Matched Studyyesakula30No ratings yet
- 7pmtank KNTTDocument8 pages7pmtank KNTTyesakula30No ratings yet
- Productflyer - 978 3 319 18841 6Document1 pageProductflyer - 978 3 319 18841 6Jesse BurrisNo ratings yet
- AE 106 Module 10 Decision TheoryDocument21 pagesAE 106 Module 10 Decision TheoryJohn Michael CabasaNo ratings yet
- Tutorial Week 11 - Correlation and RegressionDocument8 pagesTutorial Week 11 - Correlation and RegressionDemo PutraNo ratings yet
- HB 092012 SubmittedDocument26 pagesHB 092012 SubmittedBindyan KarenuNo ratings yet
- Chapter 8 Solution To Example Exercises PDFDocument3 pagesChapter 8 Solution To Example Exercises PDFShiela RengelNo ratings yet
- SAMPLING Lectures - 3Document11 pagesSAMPLING Lectures - 3Robert ManeaNo ratings yet
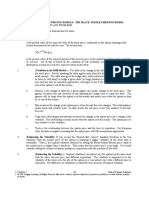
- ) N (D Xe: Chapter 5: Option Pricing Models: The Black-Scholes-Merton ModelDocument9 pages) N (D Xe: Chapter 5: Option Pricing Models: The Black-Scholes-Merton ModelTami DoanNo ratings yet
- Chapter 3Document15 pagesChapter 3Joseph KandalaftNo ratings yet
- QMT425 - Assignment 1Document5 pagesQMT425 - Assignment 1Azwan AyopNo ratings yet
- Tugas ENMS 4Document58 pagesTugas ENMS 4yuri67No ratings yet
- Game Theory - Wikipedia, The Free Encyclopedia PDFDocument25 pagesGame Theory - Wikipedia, The Free Encyclopedia PDFHenryNo ratings yet
- Kontribusi Pembelajaran Di Perguruan Tinggi Dan Literasi Keuangan Terhadap Perilaku Keuangan MahasiswaDocument11 pagesKontribusi Pembelajaran Di Perguruan Tinggi Dan Literasi Keuangan Terhadap Perilaku Keuangan MahasiswareinandaNo ratings yet
- MCQs On Correlation and Regression Analysis 1 PDFDocument3 pagesMCQs On Correlation and Regression Analysis 1 PDFnarayanasmrithiNo ratings yet
- Behavioral Econ Cheat SheetDocument3 pagesBehavioral Econ Cheat SheetM SharkNo ratings yet
- Game Theory (18Cs7F2) 7 Semester, CSE Department Faculty: Anitha Sandeep UNIT-4Document63 pagesGame Theory (18Cs7F2) 7 Semester, CSE Department Faculty: Anitha Sandeep UNIT-4Rishab RajNo ratings yet
- Chapter 2 - Quantitative AnalysisDocument244 pagesChapter 2 - Quantitative AnalysisCHAN StephenieNo ratings yet
- Course Content Lecture Plan VFDocument4 pagesCourse Content Lecture Plan VFSabbir Hasan MonirNo ratings yet
- The "Greeks": Courtesy of John Hull RotmanDocument14 pagesThe "Greeks": Courtesy of John Hull RotmansanchiNo ratings yet
- R Code For Logistic RegressionDocument3 pagesR Code For Logistic RegressionSanjay NavghareNo ratings yet
- SPSS-RAK FaktorialDocument61 pagesSPSS-RAK FaktorialMulyadi WitjaksonoNo ratings yet
- Session 11 HandoutsDocument37 pagesSession 11 HandoutsFUDANI MANISHANo ratings yet
- Basic Biostatistics Syllabus MPH 2022-2024Document5 pagesBasic Biostatistics Syllabus MPH 2022-2024Dr. Arya AgarwalNo ratings yet
- Technical Sheet: Uncertainty of Test ResultDocument6 pagesTechnical Sheet: Uncertainty of Test ResultDatHoNo ratings yet
- Econometrics Unit 2Document21 pagesEconometrics Unit 2Minh HoàngNo ratings yet
- Present Value Annuity Tables: What Is An Annuity Table?Document8 pagesPresent Value Annuity Tables: What Is An Annuity Table?Sharmin ReulaNo ratings yet
- WeightDocument5 pagesWeightijaz afzalNo ratings yet
- 1 205Document205 pages1 205bicameloNo ratings yet
- Randomized Block DesignDocument15 pagesRandomized Block Designamitpatwari100% (1)
- SST 412 Design and Analysis of ExperimentsDocument2 pagesSST 412 Design and Analysis of ExperimentsEsekon Geoffrey LokolNo ratings yet