Download as pdf or txt
You might also like
- HDFC Ergo Policy Renewal 2023 SelfDocument5 pagesHDFC Ergo Policy Renewal 2023 SelfGopivishnu KanchiNo ratings yet
- Masturbation Free EbookDocument5 pagesMasturbation Free EbookVishal Pandey75% (4)
- BS 4254Document19 pagesBS 4254gugaruban100% (4)
- Lumber Case ModelDocument6 pagesLumber Case ModeltheonlypaulNo ratings yet
- Introduction To Orthopaedic OncologyDocument22 pagesIntroduction To Orthopaedic OncologyKikiMaria100% (1)
- Primary Chest Wall TumorsDocument13 pagesPrimary Chest Wall Tumorsmhany12345No ratings yet
- Bone Tumors: Benign Tumor Malignant TumorDocument5 pagesBone Tumors: Benign Tumor Malignant TumorManish ShresthaNo ratings yet
- 6.musculoskeletal TumorsDocument110 pages6.musculoskeletal Tumorslina jamalNo ratings yet
- Bone and Joint Neoplasm or TumorDocument49 pagesBone and Joint Neoplasm or Tumorendah rahmadaniNo ratings yet
- Musculoskeletal TumorDocument89 pagesMusculoskeletal TumorHayaNo ratings yet
- Bone Tumors FinalDocument80 pagesBone Tumors FinalPATHMAPRIYA GANESANNo ratings yet
- Benign Bone TumoursDocument106 pagesBenign Bone TumoursBharath NarasimhaNo ratings yet
- Bone Tumors: - Most Common:: 5-Minute Orthopaedic Consult, 2nd EditionDocument20 pagesBone Tumors: - Most Common:: 5-Minute Orthopaedic Consult, 2nd EditionNiqavie IndonesiaNo ratings yet
- Basic MST OS GCT - QMDocument192 pagesBasic MST OS GCT - QMvicky174No ratings yet
- General Principles of Bone TumorsDocument6 pagesGeneral Principles of Bone TumorsRonald TejoprayitnoNo ratings yet
- Bone and Joint TumoursDocument49 pagesBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- BONE TUMOURS (Benign)Document42 pagesBONE TUMOURS (Benign)Ayush ChaliseNo ratings yet
- Septic ArthritisDocument94 pagesSeptic ArthritisCut Riska NovizaNo ratings yet
- Cellular Growth and AberrationsDocument20 pagesCellular Growth and Aberrationspyongjong100% (1)
- debalabreast Cancer topicDocument16 pagesdebalabreast Cancer topicbandyNo ratings yet
- Bone Tumours Evaluation Laboratory Investigations: BiopsyDocument2 pagesBone Tumours Evaluation Laboratory Investigations: BiopsyMalueth AnguiNo ratings yet
- Bone Tumor GopalDocument53 pagesBone Tumor GopalJennifer DixonNo ratings yet
- Bone Tumor: Daniel A. (Orthopedic Surgeon)Document225 pagesBone Tumor: Daniel A. (Orthopedic Surgeon)mebrieNo ratings yet
- Bone Tumor GDocument29 pagesBone Tumor Ggeleta.dima2013No ratings yet
- Non-Odontogenic Tumors of Epithelial Tissue Origin: Guided By-Presented byDocument93 pagesNon-Odontogenic Tumors of Epithelial Tissue Origin: Guided By-Presented byrajaniNo ratings yet
- LP Soft Tissue Carsinoma 1-1Document21 pagesLP Soft Tissue Carsinoma 1-1eva nandyaNo ratings yet
- GCT SeminarDocument49 pagesGCT SeminarGils ThampiNo ratings yet
- Basic Concepts of Cancer: Mohamad Bayu SahadewaDocument34 pagesBasic Concepts of Cancer: Mohamad Bayu SahadewaHendra EfendiNo ratings yet
- Session 9 MalignanciesDocument92 pagesSession 9 MalignanciesZNo ratings yet
- 9.2 - Soft Tissue TumorsDocument13 pages9.2 - Soft Tissue Tumorsmoges beletachawNo ratings yet
- Soft Tissue Sarcomas ofDocument35 pagesSoft Tissue Sarcomas ofmogesie1995No ratings yet
- Cellular AberrationDocument83 pagesCellular AberrationA. Lizette PabloNo ratings yet
- Retroperitoneal SarcomaDocument88 pagesRetroperitoneal SarcomaJeff LuwangNo ratings yet
- Tumors Around Knee in PediatricsDocument25 pagesTumors Around Knee in PediatricsMike RossNo ratings yet
- Spinal Tumor: Zelin Sun MD, PH.DDocument28 pagesSpinal Tumor: Zelin Sun MD, PH.DMargaret ThatcherNo ratings yet
- Oncology NursingDocument6 pagesOncology NursingreooooNo ratings yet
- Bone TumorsDocument29 pagesBone TumorsmatameaNo ratings yet
- Bone Tumor DefinitionDocument2 pagesBone Tumor DefinitionJinsen Paul MartinNo ratings yet
- Book Reading BiopsyDocument9 pagesBook Reading BiopsyAidil NurshalNo ratings yet
- 02.22.1 Neoplasia I Final PDFDocument79 pages02.22.1 Neoplasia I Final PDFSameeha AbbasNo ratings yet
- Dr. Alban-ODP 2016 SarcomaDocument37 pagesDr. Alban-ODP 2016 SarcomaAfraDewitaNo ratings yet
- Tumours: Apley 9th Ed p.187-223Document66 pagesTumours: Apley 9th Ed p.187-223Helmi IsmunandarNo ratings yet
- Bone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaDocument85 pagesBone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaWan Nur AdilahNo ratings yet
- Approach To Bone Tumor DiagnosisDocument25 pagesApproach To Bone Tumor DiagnosisFatini ChokNo ratings yet
- Neoplastic DisordersDocument36 pagesNeoplastic DisordersJSeasharkNo ratings yet
- Xraydxbonetumor Jenkinson1927Document10 pagesXraydxbonetumor Jenkinson1927pantukan doctorsNo ratings yet
- Oral Neoplasma III SoundDocument53 pagesOral Neoplasma III SoundJi ChuNo ratings yet
- Clinical Oncology - Teaching Clinic - Overture To Cancer CareDocument13 pagesClinical Oncology - Teaching Clinic - Overture To Cancer CarehalesipsumNo ratings yet
- Neoplasia 2Document38 pagesNeoplasia 2yusramoe14No ratings yet
- Management of Soft Tissue SarcomaDocument86 pagesManagement of Soft Tissue SarcomaSACHIN SNo ratings yet
- Cancer Bio Lecture 3Document26 pagesCancer Bio Lecture 3snoori2307No ratings yet
- MS TumorsDocument16 pagesMS TumorsASM MutahirNo ratings yet
- Cancer NotesDocument6 pagesCancer NotesRocco WalksNo ratings yet
- 3 - Fudamentals of Neoplasm 2022Document32 pages3 - Fudamentals of Neoplasm 2022noreentamer20No ratings yet
- NeoplasiaDocument31 pagesNeoplasiaAnin PrakashNo ratings yet
- LP Soft Tisue SarcomaDocument10 pagesLP Soft Tisue Sarcomaarsala ashariNo ratings yet
- 2014 Musculoskeletal Tumors and DiseasesDocument102 pages2014 Musculoskeletal Tumors and DiseasesNanda GemaNo ratings yet
- Chest Wall and Chest Wall Neoplasms: Dr. Alfredo M. IgamaDocument11 pagesChest Wall and Chest Wall Neoplasms: Dr. Alfredo M. Igamaredz_ekg619No ratings yet
- Tumor MusculoskeletalDocument41 pagesTumor Musculoskeletalrisky setyanNo ratings yet
- Oncology: Farrahiyah IsmailDocument33 pagesOncology: Farrahiyah IsmailaisyahambaliNo ratings yet
- Imaging Evaluation of Malignant Chest Wall NeoplasmsDocument51 pagesImaging Evaluation of Malignant Chest Wall NeoplasmsRicky SeptafiantyNo ratings yet
- Nursing Oncology NotesDocument58 pagesNursing Oncology Notesrachel lorenNo ratings yet
- Bone tm3Document57 pagesBone tm3ZakiyahulfahdwNo ratings yet
- Case Study On A Highway Project: Environmental Impact AssesmentDocument10 pagesCase Study On A Highway Project: Environmental Impact AssesmentSRUTHI FRANCIS M.Tech Environmental Engineering 2020-2022No ratings yet
- Materials Chemistry A: Journal ofDocument7 pagesMaterials Chemistry A: Journal ofFamiloni LayoNo ratings yet
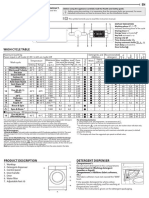
- Whirlpool BIWDWG861484uk enDocument4 pagesWhirlpool BIWDWG861484uk ennadaljoachim77No ratings yet
- Phason FHC1D User ManualDocument16 pagesPhason FHC1D User Manuale-ComfortUSANo ratings yet
- Codes Standards RegulationsDocument11 pagesCodes Standards RegulationsEslNo ratings yet
- Parent Medical CoverageDocument9 pagesParent Medical CoveragecampeonNo ratings yet
- GRES Integrated Energy Storage SystemDocument33 pagesGRES Integrated Energy Storage SystemVadim PopovichNo ratings yet
- Ebook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFDocument67 pagesEbook Chemistry For Today General Organic and Biochemistry PDF Full Chapter PDFrobert.davidson233100% (31)
- Dan Sof TG 0122Document30 pagesDan Sof TG 0122Erick Trujillo100% (1)
- Fiberdyne G.652.D Single Mode Fiber SpecificationsDocument1 pageFiberdyne G.652.D Single Mode Fiber SpecificationsjunedNo ratings yet
- Hospital Management System: Dept. of CSE, GECRDocument30 pagesHospital Management System: Dept. of CSE, GECRYounus KhanNo ratings yet
- Reading ResponseDocument3 pagesReading ResponseJack SikoliaNo ratings yet
- VBIED Attack July 31, 2007Document1 pageVBIED Attack July 31, 2007Rhonda NoldeNo ratings yet
- PLKS321 Unit 8.9 PMDocument56 pagesPLKS321 Unit 8.9 PMmonagomolemo9No ratings yet
- Chemistry Project 2021-2022Document19 pagesChemistry Project 2021-2022Rudra SathwaraNo ratings yet
- Feasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentDocument9 pagesFeasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentAhmed RamzyNo ratings yet
- Building An Effective Safety Management System For Airlines: James J.H. Liou, Leon Yen, Gwo-Hshiung TzengDocument7 pagesBuilding An Effective Safety Management System For Airlines: James J.H. Liou, Leon Yen, Gwo-Hshiung Tzengzatul hasniNo ratings yet
- Problem Sets For Solutions AnalysisDocument2 pagesProblem Sets For Solutions AnalysisKamil Guillergan100% (1)
- Test Bank For The Practice of Statistics in The Life Sciences 4th Edition Brigitte BaldiDocument23 pagesTest Bank For The Practice of Statistics in The Life Sciences 4th Edition Brigitte BaldiDebra Franken100% (31)
- Conference Meeting ScriptDocument2 pagesConference Meeting ScriptAndrei PrinsesaNo ratings yet
- PHAS0027 RevisionDocument21 pagesPHAS0027 Revisionunknown.unknown9901No ratings yet
- Iec Inverse Protection CurvesDocument1 pageIec Inverse Protection CurvesEng-Ahmad Abo-AledousNo ratings yet
- Bio OhDocument3 pagesBio OhEmmaNo ratings yet
- Re 51400Document14 pagesRe 51400Jamin Smtpng0% (1)
- VegDocument130 pagesVegAnanda PreethiNo ratings yet