Download as pdf or txt
You might also like
- BWS - The Smartest Back Workout For A Thicker, Wider Back PDFDocument19 pagesBWS - The Smartest Back Workout For A Thicker, Wider Back PDFSanjo SunnyNo ratings yet
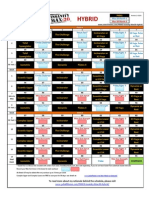
- P90X3 Max30 Hybrid Rev1Document1 pageP90X3 Max30 Hybrid Rev1Felipe Andres Soto ZavalaNo ratings yet
- HomeHero Ebook 2020Document31 pagesHomeHero Ebook 2020Valentín DamsNo ratings yet
- Ef73152bedf3ae PDFDocument2 pagesEf73152bedf3ae PDFMouloud ZéMaNo ratings yet
- Shoulder Secial Tests Final FrontierDocument6 pagesShoulder Secial Tests Final Frontierdina sharafNo ratings yet
- Orthopedic Shoulder ExaminationDocument4 pagesOrthopedic Shoulder Examinationapi-281340024No ratings yet
- Shoulder TestsDocument39 pagesShoulder TestsranafayyazsahilNo ratings yet
- Special Tests UeDocument7 pagesSpecial Tests UeRiaz KhanNo ratings yet
- Tendon TestsDocument8 pagesTendon TestsASM MutahirNo ratings yet
- Special Test:: Sensitivity: The Ability of A Test To Correctly Identify Patients With ADocument32 pagesSpecial Test:: Sensitivity: The Ability of A Test To Correctly Identify Patients With AnatkwqNo ratings yet
- 9 Hip & Lumber DDDocument29 pages9 Hip & Lumber DDHeba Abo bakrNo ratings yet
- Shoulder Exam ChecklistDocument2 pagesShoulder Exam ChecklistJaymin BhattNo ratings yet
- Shoulder Exam - Shoulder & Elbow - OrthobulletsDocument8 pagesShoulder Exam - Shoulder & Elbow - Orthobulletsbrokenlimit5No ratings yet
- Special Test For Shoulder:-For ImpingementDocument5 pagesSpecial Test For Shoulder:-For ImpingementYusrah SaniNo ratings yet
- C5 Elbow Flexors - Biceps Brachii, BrachialisDocument17 pagesC5 Elbow Flexors - Biceps Brachii, BrachialismayraNo ratings yet
- Motor Exam GuideDocument16 pagesMotor Exam GuideNohemí Gómez ANo ratings yet
- Kinesiologi Siku-Pf UnaDocument59 pagesKinesiologi Siku-Pf Unasingle_ladyNo ratings yet
- Assignment 5Document3 pagesAssignment 5Madesh YadavNo ratings yet
- TM Shoulder Exam-1Document36 pagesTM Shoulder Exam-1ratkhiaberNo ratings yet
- Shoulder AssessmentDocument9 pagesShoulder AssessmentsarahemulvennaNo ratings yet
- Unhappy Triad of O'DonahueDocument14 pagesUnhappy Triad of O'DonahueGuadalupe GuzmánNo ratings yet
- Anterior DeltoidDocument2 pagesAnterior DeltoidneuropandianNo ratings yet
- Shoulder InstabilityDocument57 pagesShoulder Instabilityashithoshn06No ratings yet
- MMT Volume 2 Lower Extremity and Spine SampleDocument6 pagesMMT Volume 2 Lower Extremity and Spine SampleYong Kyu KimNo ratings yet
- 5-Shoulder FlexionDocument16 pages5-Shoulder FlexionDaniJaralNo ratings yet
- Clinical Tests in Shoulder Examination - How To Perform ThemDocument7 pagesClinical Tests in Shoulder Examination - How To Perform Themprofpt98No ratings yet
- Functional Tests For The TrunkDocument13 pagesFunctional Tests For The TrunkLisa SmithNo ratings yet
- Hip Joint ExaminationDocument53 pagesHip Joint ExaminationmybabyistaeNo ratings yet
- Ortho VertDocument4 pagesOrtho VertfelixhartantoNo ratings yet
- Sahana MSDocument19 pagesSahana MSSahana ChowdhuryNo ratings yet
- Reading Knee - RamaDocument33 pagesReading Knee - RamavjhvghcghcghghNo ratings yet
- Umar ExamDocument11 pagesUmar ExamDan IonescuNo ratings yet
- Manual Muscle TestingDocument19 pagesManual Muscle TestingJoanna EdenNo ratings yet
- Special Tests of The KneeDocument21 pagesSpecial Tests of The KneeZephyrin Izukw100% (1)
- Specialtest Knee 140720123835 Phpapp01 PDFDocument146 pagesSpecialtest Knee 140720123835 Phpapp01 PDFlaszlo-368875100% (1)
- 09 Cervical Spine 2Document12 pages09 Cervical Spine 2楊畯凱No ratings yet
- MMT8 Testing ProceduresDocument17 pagesMMT8 Testing ProceduresTafzz SailoNo ratings yet
- Exam ShoulderDocument27 pagesExam ShouldersingwongcsNo ratings yet
- Cross Test of The Arm Abductor Muscle & Wrist Extensor Muscles Without RotationDocument2 pagesCross Test of The Arm Abductor Muscle & Wrist Extensor Muscles Without Rotationonix2000No ratings yet
- Special Test LEDocument45 pagesSpecial Test LEStudy PhillyNo ratings yet
- Physioterapy SalveDocument45 pagesPhysioterapy SalveIkhar KeliobasNo ratings yet
- Shoulder TestDocument2 pagesShoulder TestEdwinNo ratings yet
- Physical Exam Shoulder EditDocument28 pagesPhysical Exam Shoulder EditNur Syamsiah MNo ratings yet
- Hawkins-Kennedy Test: Humerus LigamentDocument7 pagesHawkins-Kennedy Test: Humerus LigamentlewienNo ratings yet
- MSK 3Document6 pagesMSK 3saharnawaz791No ratings yet
- Examination of The ShoulderDocument33 pagesExamination of The ShoulderAnonymous 9QxPDpNo ratings yet
- Muscle Testing: Knee Flexion + ExtensionDocument38 pagesMuscle Testing: Knee Flexion + ExtensionHaruka HaganeNo ratings yet
- MSK Special Test ChartDocument6 pagesMSK Special Test ChartevahealthfirstNo ratings yet
- Manual Muscle Testing: Shoulde R AbductionDocument14 pagesManual Muscle Testing: Shoulde R AbductionDaniJaralNo ratings yet
- Physical Examination of The Shoulder FinalDocument28 pagesPhysical Examination of The Shoulder FinalAndinNo ratings yet
- Different Special Tests For Different JointsDocument4 pagesDifferent Special Tests For Different JointsAbbas AliNo ratings yet
- Special Test KneeDocument7 pagesSpecial Test KneeraniNo ratings yet
- Pemeriksaan Fisik BahuDocument35 pagesPemeriksaan Fisik BahuShone NamNo ratings yet
- Workshop PPT (Final) Knee JointDocument127 pagesWorkshop PPT (Final) Knee Jointpasha100% (2)
- Position of PatientDocument47 pagesPosition of PatientMuhammad Al-azzizNo ratings yet
- Mulligan Therapy: What Is It and How Does It WorkDocument33 pagesMulligan Therapy: What Is It and How Does It WorkAgus SantosoNo ratings yet
- Joint Exam Special Test ReviewDocument4 pagesJoint Exam Special Test ReviewNish ShahNo ratings yet
- Position S: Pratiksha RaiDocument49 pagesPosition S: Pratiksha RaiJoanne Cristie TolopiaNo ratings yet
- Shoulder ExaminationDocument10 pagesShoulder ExaminationcmonmanNo ratings yet
- Ortopedic TestsDocument4 pagesOrtopedic TestsdocfinNo ratings yet
- Scorpio Training: Kettlebell Exercises: The Way of the ScorpioFrom EverandScorpio Training: Kettlebell Exercises: The Way of the ScorpioNo ratings yet
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Outcome Measures PCE Final FrontierDocument14 pagesOutcome Measures PCE Final FrontierMaitryChhedaNo ratings yet
- Open Chain Vs Closed ChainDocument7 pagesOpen Chain Vs Closed ChainMaitryChhedaNo ratings yet
- Shoulder Joint PCEFFDocument38 pagesShoulder Joint PCEFFMaitryChhedaNo ratings yet
- Wrist and Hand PCEFFDocument17 pagesWrist and Hand PCEFFMaitryChhedaNo ratings yet
- Types Fo Fractures Dutton 3rd 44-45Document2 pagesTypes Fo Fractures Dutton 3rd 44-45MaitryChhedaNo ratings yet
- Tens & Ems Pce FFDocument5 pagesTens & Ems Pce FFMaitryChhedaNo ratings yet
- Therapy Ed 2018 304-308Document5 pagesTherapy Ed 2018 304-308MaitryChhedaNo ratings yet
- PneumoniaDocument3 pagesPneumoniaMaitryChhedaNo ratings yet
- Pleural Effusion-DESKTOP-3C8QD8MDocument3 pagesPleural Effusion-DESKTOP-3C8QD8MMaitryChhedaNo ratings yet
- Pulmonary TBDocument2 pagesPulmonary TBMaitryChhedaNo ratings yet
- Henna Designs PDFDocument10 pagesHenna Designs PDFMaitryChhedaNo ratings yet
- Maitry Chheda: Ug 2020 - PresentDocument2 pagesMaitry Chheda: Ug 2020 - PresentMaitryChhedaNo ratings yet
- Log Sheet 2Document1 pageLog Sheet 2MaitryChhedaNo ratings yet
- The New 5x5: How To Make 5x5 Training Even BetterDocument5 pagesThe New 5x5: How To Make 5x5 Training Even BetterÒó ReverseNo ratings yet
- ModalsDocument4 pagesModalsMuhammet ÜNLÜNo ratings yet
- REVISIONDocument2 pagesREVISIONThủy TiênNo ratings yet
- Research Study 4Document1 pageResearch Study 4api-259085702No ratings yet
- Lesson1 Subject Orientation The Concept of Physical EducationDocument5 pagesLesson1 Subject Orientation The Concept of Physical EducationsoftjjungkookNo ratings yet
- Laselle Manual ENG PreviewDocument12 pagesLaselle Manual ENG PreviewSilvia IriarteNo ratings yet
- Cardio Fitness ProjectDocument1 pageCardio Fitness ProjectVijay ChikkiNo ratings yet
- Write Your Answer in Red (Escriba Su Respuesta Con Rojo)Document3 pagesWrite Your Answer in Red (Escriba Su Respuesta Con Rojo)Veronika FlorianNo ratings yet
- VHSL Recommended Phase 3 Guidelines For Reopening High School Sports/activitiesDocument9 pagesVHSL Recommended Phase 3 Guidelines For Reopening High School Sports/activitiesJeff WilliamsonNo ratings yet
- The Power of Stretching v5Document12 pagesThe Power of Stretching v5Maria TelloNo ratings yet
- NCP 2Document2 pagesNCP 2Aneeza Musa IndananNo ratings yet
- Activity 1 Matching Type, Collage, Physical Fitness TestDocument5 pagesActivity 1 Matching Type, Collage, Physical Fitness TestMiles ObedenciaNo ratings yet
- The 8 Benefits of Exercising: 1. Beter Mood ControlDocument2 pagesThe 8 Benefits of Exercising: 1. Beter Mood ControlBaha YazıcılarNo ratings yet
- Zumba (Final Demo)Document10 pagesZumba (Final Demo)Hyzel Faith ParanNo ratings yet
- Presentation 1Document91 pagesPresentation 1Alemar AcotNo ratings yet
- Basic Powerlifting RoutineDocument20 pagesBasic Powerlifting RoutineRoberto Trotta100% (2)
- Power Breathing Breathe Your Way To Inner Power (2008)Document264 pagesPower Breathing Breathe Your Way To Inner Power (2008)Pk100% (2)
- Dorian Yates 1987-1992 Workout Routine SpreadsheetDocument13 pagesDorian Yates 1987-1992 Workout Routine SpreadsheetRicardo RibeiroNo ratings yet
- BROCHURE - Empress PDFDocument24 pagesBROCHURE - Empress PDFDave LooNo ratings yet
- Physical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersDocument6 pagesPhysical Rehabilitation 2.2 Rehabilitation of Lower Limb Musculoskeletal DisordersJAIRISH YZABELLE SALVADORNo ratings yet
- KIZEN 3 Day Maximum Strength (Boris Sheiko) - Cycle 2Document61 pagesKIZEN 3 Day Maximum Strength (Boris Sheiko) - Cycle 2Dornilda Jovino De Almeida Aimbaré De Tucunduvá0% (2)
- Case Summary France v. Turkey, (1927) PCIJ Ser. A, No. 10, 4Document5 pagesCase Summary France v. Turkey, (1927) PCIJ Ser. A, No. 10, 4Priyal GuptaNo ratings yet
- Stress Management in Young AdultsDocument12 pagesStress Management in Young AdultsamoeboidNo ratings yet
- Physical Education and Health 3: Module ForDocument5 pagesPhysical Education and Health 3: Module Forsay francoNo ratings yet
- Yoga MapehDocument2 pagesYoga MapehEilinre OlinNo ratings yet
- Sheiko Base TemplatesDocument108 pagesSheiko Base TemplatesSami KukkonenNo ratings yet