
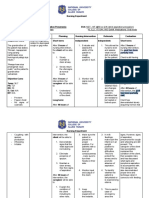
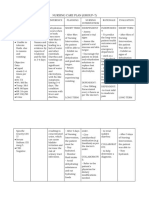
Case Mapping NCP
Case Mapping NCP
You might also like
- NCP 3rd YearDocument6 pagesNCP 3rd YearTotoro AblogNo ratings yet
- NCP (Appendicitis)Document3 pagesNCP (Appendicitis)Jenny Ajoc100% (1)
- NCP LeptospirosisDocument2 pagesNCP LeptospirosisLouise Anne Asuncion OclimaNo ratings yet
- Reports No Pain During Urination. There Will Be No Tension in Bladder The Patient Will Appear CalmDocument4 pagesReports No Pain During Urination. There Will Be No Tension in Bladder The Patient Will Appear CalmDenise Louise PoNo ratings yet
- Toward A Theory of DeceptionDocument37 pagesToward A Theory of DeceptionThe Angry ManNo ratings yet
- Green GDP 2Document51 pagesGreen GDP 2Vikas GuptaNo ratings yet
- NCP UTI (Artillo)Document3 pagesNCP UTI (Artillo)Al TheóNo ratings yet
- Beronio, Gracel Caye M. CMC Module 6 GI Pedia (Nursing Care Plans)Document5 pagesBeronio, Gracel Caye M. CMC Module 6 GI Pedia (Nursing Care Plans)Gracel Caye Maon BeronioNo ratings yet
- Uti - NCPDocument3 pagesUti - NCPRap De la Cruz100% (1)
- NCP Ruq PainDocument3 pagesNCP Ruq PainKristine YoungNo ratings yet
- NCP Requirements RleDocument7 pagesNCP Requirements RleZymer Lee AbasoloNo ratings yet
- 3.1 Assessment: A. Gender: Male Age: 40 Years Old B. Main ComplaintsDocument5 pages3.1 Assessment: A. Gender: Male Age: 40 Years Old B. Main Complaintsvictor zhefaNo ratings yet
- Appendix B Nursing Care Plan Clinical Portait Assessment: Received PatientDocument14 pagesAppendix B Nursing Care Plan Clinical Portait Assessment: Received Patientjopearl18No ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Related Learning Experience Fundamentals in Nursing 4 RotationDocument3 pagesRelated Learning Experience Fundamentals in Nursing 4 RotationMark Eliezer CulasingNo ratings yet
- Fernandez 1b NCPDocument7 pagesFernandez 1b NCPToni Marie FernandezNo ratings yet
- 1st DayDocument2 pages1st DayLyrechel de GuzmanNo ratings yet
- NCPDocument2 pagesNCPKhatlen BagaresNo ratings yet
- Bert Mao Nani Final Promise HahahaahDocument10 pagesBert Mao Nani Final Promise HahahaahHerbert EstremosNo ratings yet
- NCP Conception ActivityDocument3 pagesNCP Conception ActivityMarl TanNo ratings yet
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- Nursing Care Plan of A Patient With Ebola Virus DiseaseDocument3 pagesNursing Care Plan of A Patient With Ebola Virus DiseaseJam100% (1)
- 1st DayDocument3 pages1st DayLyrechel de GuzmanNo ratings yet
- NCMB 316 Assignment NCP Part 2Document3 pagesNCMB 316 Assignment NCP Part 2I'm a PepegaNo ratings yet
- Assessment Diagnosis Scientific Background Planning Implementation Rationale EvaluationDocument2 pagesAssessment Diagnosis Scientific Background Planning Implementation Rationale EvaluationREOLALAS, Mariane JoyNo ratings yet
- Case Study Group C MCN Rle Level IIDocument14 pagesCase Study Group C MCN Rle Level IIRea Jane Astrologo PastorNo ratings yet
- Assessment Planning Intervention Evaluation: Subjective Short Term Goal: Independent Short Term GoalDocument2 pagesAssessment Planning Intervention Evaluation: Subjective Short Term Goal: Independent Short Term GoalGlaiza FabiaNo ratings yet
- Cough NCPDocument2 pagesCough NCPMYLENE GRACE ELARCOSANo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- Nursing Care Plan - ProdigalidadDocument5 pagesNursing Care Plan - ProdigalidadZxiayieee JeonNo ratings yet
- Nurses Notes Date Focus Data Action Response: SubjectiveDocument2 pagesNurses Notes Date Focus Data Action Response: SubjectiveGILIANNE MARIE JIMENEANo ratings yet
- Funda Sample ScenarioDocument2 pagesFunda Sample ScenarioGadez JeanpelNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationMykel FloresNo ratings yet
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- ASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoDocument1 pageASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoCherie MayNo ratings yet
- NCP - PneumoniaDocument3 pagesNCP - PneumoniaNikiNo ratings yet
- Saransamun Jonaisah M. NCPDocument2 pagesSaransamun Jonaisah M. NCPJames Conrad SalengaNo ratings yet
- NCP (Acute Pain)Document2 pagesNCP (Acute Pain)jennilois100% (1)
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- 2 NCP Formulated From Case Study LUCI DONNA MAE V.Document8 pages2 NCP Formulated From Case Study LUCI DONNA MAE V.Harlene Joyce ReyNo ratings yet
- MONIS, Clemcy Pearl A. (NCP 103)Document5 pagesMONIS, Clemcy Pearl A. (NCP 103)Clemcy Pearl MonisNo ratings yet
- NCP - BSN12F - Pumbaya (Module 4)Document3 pagesNCP - BSN12F - Pumbaya (Module 4)Ellah PumbayaNo ratings yet
- 1BSN3 GRP 2 Worksheet 3Document5 pages1BSN3 GRP 2 Worksheet 3ysa.antonio12No ratings yet
- Forro Intestinal ObstructionDocument3 pagesForro Intestinal ObstructionShiehan Mae ForroNo ratings yet
- Mirana BSN2-7 NCPDocument3 pagesMirana BSN2-7 NCPCrystal MiranaNo ratings yet
- NCP ADocument2 pagesNCP AMarithe Joi Abarico AberosNo ratings yet
- Group-5 NCM-107 NCPDocument4 pagesGroup-5 NCM-107 NCPbulok netflakes100% (1)
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- Concept Map Good ExampleDocument1 pageConcept Map Good Examplekellymk2584No ratings yet
- Uti Nursing Care Plan FinalDocument18 pagesUti Nursing Care Plan FinalAmit RanjanNo ratings yet
- Ehr PDFDocument31 pagesEhr PDFNicolai MabituinNo ratings yet
- NCP & DSDocument4 pagesNCP & DSKyla Marie TejadaNo ratings yet
- NCP With Eval Dewara BSN3FDocument2 pagesNCP With Eval Dewara BSN3FPrincess Faniega SugatonNo ratings yet
- Patient Name: Lorna Dimagiba Age: 84 Years Old Gender: Female C.S: Widow BED#: #1Document3 pagesPatient Name: Lorna Dimagiba Age: 84 Years Old Gender: Female C.S: Widow BED#: #1Girlie MebañaNo ratings yet
- SKYLA FIESTA NCP (Acute Pancreatitis)Document4 pagesSKYLA FIESTA NCP (Acute Pancreatitis)Skyla FiestaNo ratings yet
- NCP Kenezo, Female 17Document2 pagesNCP Kenezo, Female 17labanesstephanyNo ratings yet
- NCP Ectopic-Pregnancy1Document9 pagesNCP Ectopic-Pregnancy1Jullian PloyaNo ratings yet
- ASSESSMENT SummerDocument1 pageASSESSMENT SummerThoyotsukha Faeldan123No ratings yet
- NCP G7Document2 pagesNCP G7katt.edlessNo ratings yet
- Appendix D Nursing Care PlanDocument8 pagesAppendix D Nursing Care PlanVinz OñoNo ratings yet
- Postpartum SimulationDocument2 pagesPostpartum SimulationEarly SaribaNo ratings yet
- Soak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyFrom EverandSoak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyNo ratings yet
- 14-54 8m-Inetermediate-3Document10 pages14-54 8m-Inetermediate-3epdsan3dNo ratings yet
- 18CS731Document438 pages18CS731Sangeetha NNo ratings yet
- Online Marketing EssentialsDocument508 pagesOnline Marketing EssentialsElena BotezatuNo ratings yet
- Science Internet ResourcesDocument4 pagesScience Internet ResourcesGabriela D CostescuNo ratings yet
- Course Curriculum of PGP Renewable EnergyDocument6 pagesCourse Curriculum of PGP Renewable EnergyRonanki RaviNo ratings yet
- Finding and Correcting Mistakes Exercise 1. The Boss From HellDocument6 pagesFinding and Correcting Mistakes Exercise 1. The Boss From HellKhiêm Trần ThịNo ratings yet
- MDR11 InstructionsDocument4 pagesMDR11 Instructionsjuan tellezNo ratings yet
- Total Marks: 25 Duration: One Hour: Xii-Msths Case Study Questions - Test Term-IDocument8 pagesTotal Marks: 25 Duration: One Hour: Xii-Msths Case Study Questions - Test Term-ISABARI SRINIVAS ANo ratings yet
- Tilt TableDocument2 pagesTilt TablenikhilNo ratings yet
- Evangelism 1Document4 pagesEvangelism 1Horace Owiti O.No ratings yet
- Safety Instrumented Systems: GlobalDocument410 pagesSafety Instrumented Systems: Globalmohammed el erianNo ratings yet
- Smoke DetectorDocument1 pageSmoke DetectorTarikNo ratings yet
- A289A289M-97 (2013) Standard Specification For Alloy Steel Forgings For Nonmagnetic Retaining Rings For GeneratorsDocument3 pagesA289A289M-97 (2013) Standard Specification For Alloy Steel Forgings For Nonmagnetic Retaining Rings For GeneratorsShico1983No ratings yet
- Unit 7-Chemical Reactions NotesDocument55 pagesUnit 7-Chemical Reactions Notesapi-182809945No ratings yet
- 216B2, 226B2, 232B2, 236B2, 242B2, Electrical System 247B2 and 257B2 Multi-Terrain Loader and 252B2 Skid Steer LoaderDocument4 pages216B2, 226B2, 232B2, 236B2, 242B2, Electrical System 247B2 and 257B2 Multi-Terrain Loader and 252B2 Skid Steer LoaderAirton SenaNo ratings yet
- PC/SC Partial Documentation of The API: PMDZ061-AE 24/09/2009Document32 pagesPC/SC Partial Documentation of The API: PMDZ061-AE 24/09/2009manskebe6121No ratings yet
- Surface Preparation Standards JotunDocument2 pagesSurface Preparation Standards JotunbacabacabacaNo ratings yet
- What Is Big DataDocument2 pagesWhat Is Big DatasanjnaNo ratings yet
- IT 16 - Neurogenic Bladder - SMDocument31 pagesIT 16 - Neurogenic Bladder - SMRurie Awalia SuhardiNo ratings yet
- 2023 - ECON422 - TURKISH ECONOMY - HOMEWORK - Final VersionDocument3 pages2023 - ECON422 - TURKISH ECONOMY - HOMEWORK - Final VersionsenaNo ratings yet
- Internet Banking (E-Banking)Document16 pagesInternet Banking (E-Banking)Saurabh G0% (2)
- Filtration Solution To Problems - Pdf-Midterm-Exam-AnswerDocument7 pagesFiltration Solution To Problems - Pdf-Midterm-Exam-AnswerDubu Kim100% (1)
- 61cm InfoDocument4 pages61cm InfoHow to do anything By HimanshuNo ratings yet
- PHD Syllabus AMUDocument2 pagesPHD Syllabus AMUMohd ShahidNo ratings yet
- Volume 7 No 8 2018Document142 pagesVolume 7 No 8 2018Salhi AmaraNo ratings yet
- System Path VariablesDocument5 pagesSystem Path VariablesUnessNo ratings yet
- Gravimetric Determination of Barium SulfateDocument3 pagesGravimetric Determination of Barium SulfateArmiee InfiniteNo ratings yet
- DB Nutrition GuideDocument59 pagesDB Nutrition GuideBárbara Leite100% (2)
























































































Download as docx, pdf, or txt
You might also like
- NCP 3rd YearDocument6 pagesNCP 3rd YearTotoro AblogNo ratings yet
- NCP (Appendicitis)Document3 pagesNCP (Appendicitis)Jenny Ajoc100% (1)
- NCP LeptospirosisDocument2 pagesNCP LeptospirosisLouise Anne Asuncion OclimaNo ratings yet
- Reports No Pain During Urination. There Will Be No Tension in Bladder The Patient Will Appear CalmDocument4 pagesReports No Pain During Urination. There Will Be No Tension in Bladder The Patient Will Appear CalmDenise Louise PoNo ratings yet
- Toward A Theory of DeceptionDocument37 pagesToward A Theory of DeceptionThe Angry ManNo ratings yet
- Green GDP 2Document51 pagesGreen GDP 2Vikas GuptaNo ratings yet
- NCP UTI (Artillo)Document3 pagesNCP UTI (Artillo)Al TheóNo ratings yet
- Beronio, Gracel Caye M. CMC Module 6 GI Pedia (Nursing Care Plans)Document5 pagesBeronio, Gracel Caye M. CMC Module 6 GI Pedia (Nursing Care Plans)Gracel Caye Maon BeronioNo ratings yet
- Uti - NCPDocument3 pagesUti - NCPRap De la Cruz100% (1)
- NCP Ruq PainDocument3 pagesNCP Ruq PainKristine YoungNo ratings yet
- NCP Requirements RleDocument7 pagesNCP Requirements RleZymer Lee AbasoloNo ratings yet
- 3.1 Assessment: A. Gender: Male Age: 40 Years Old B. Main ComplaintsDocument5 pages3.1 Assessment: A. Gender: Male Age: 40 Years Old B. Main Complaintsvictor zhefaNo ratings yet
- Appendix B Nursing Care Plan Clinical Portait Assessment: Received PatientDocument14 pagesAppendix B Nursing Care Plan Clinical Portait Assessment: Received Patientjopearl18No ratings yet
- Final Nursing Care PlanDocument7 pagesFinal Nursing Care PlanKatherine BellezaNo ratings yet
- Related Learning Experience Fundamentals in Nursing 4 RotationDocument3 pagesRelated Learning Experience Fundamentals in Nursing 4 RotationMark Eliezer CulasingNo ratings yet
- Fernandez 1b NCPDocument7 pagesFernandez 1b NCPToni Marie FernandezNo ratings yet
- 1st DayDocument2 pages1st DayLyrechel de GuzmanNo ratings yet
- NCPDocument2 pagesNCPKhatlen BagaresNo ratings yet
- Bert Mao Nani Final Promise HahahaahDocument10 pagesBert Mao Nani Final Promise HahahaahHerbert EstremosNo ratings yet
- NCP Conception ActivityDocument3 pagesNCP Conception ActivityMarl TanNo ratings yet
- NCP Case Analysis GastritisDocument7 pagesNCP Case Analysis GastritisSteffi GolezNo ratings yet
- Nursing Care Plan of A Patient With Ebola Virus DiseaseDocument3 pagesNursing Care Plan of A Patient With Ebola Virus DiseaseJam100% (1)
- 1st DayDocument3 pages1st DayLyrechel de GuzmanNo ratings yet
- NCMB 316 Assignment NCP Part 2Document3 pagesNCMB 316 Assignment NCP Part 2I'm a PepegaNo ratings yet
- Assessment Diagnosis Scientific Background Planning Implementation Rationale EvaluationDocument2 pagesAssessment Diagnosis Scientific Background Planning Implementation Rationale EvaluationREOLALAS, Mariane JoyNo ratings yet
- Case Study Group C MCN Rle Level IIDocument14 pagesCase Study Group C MCN Rle Level IIRea Jane Astrologo PastorNo ratings yet
- Assessment Planning Intervention Evaluation: Subjective Short Term Goal: Independent Short Term GoalDocument2 pagesAssessment Planning Intervention Evaluation: Subjective Short Term Goal: Independent Short Term GoalGlaiza FabiaNo ratings yet
- Cough NCPDocument2 pagesCough NCPMYLENE GRACE ELARCOSANo ratings yet
- Hypovolemic Shock Sample NCPDocument14 pagesHypovolemic Shock Sample NCPRENEROSE TORRES100% (1)
- Nursing Care Plan - ProdigalidadDocument5 pagesNursing Care Plan - ProdigalidadZxiayieee JeonNo ratings yet
- Nurses Notes Date Focus Data Action Response: SubjectiveDocument2 pagesNurses Notes Date Focus Data Action Response: SubjectiveGILIANNE MARIE JIMENEANo ratings yet
- Funda Sample ScenarioDocument2 pagesFunda Sample ScenarioGadez JeanpelNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationMykel FloresNo ratings yet
- NCP PediatricDocument5 pagesNCP PediatricSL Hanna NebridaNo ratings yet
- ASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoDocument1 pageASSESSMENT S: "Nanghihina Ako, Hindi Ko Magawa Yung Mga GustoCherie MayNo ratings yet
- NCP - PneumoniaDocument3 pagesNCP - PneumoniaNikiNo ratings yet
- Saransamun Jonaisah M. NCPDocument2 pagesSaransamun Jonaisah M. NCPJames Conrad SalengaNo ratings yet
- NCP (Acute Pain)Document2 pagesNCP (Acute Pain)jennilois100% (1)
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- 2 NCP Formulated From Case Study LUCI DONNA MAE V.Document8 pages2 NCP Formulated From Case Study LUCI DONNA MAE V.Harlene Joyce ReyNo ratings yet
- MONIS, Clemcy Pearl A. (NCP 103)Document5 pagesMONIS, Clemcy Pearl A. (NCP 103)Clemcy Pearl MonisNo ratings yet
- NCP - BSN12F - Pumbaya (Module 4)Document3 pagesNCP - BSN12F - Pumbaya (Module 4)Ellah PumbayaNo ratings yet
- 1BSN3 GRP 2 Worksheet 3Document5 pages1BSN3 GRP 2 Worksheet 3ysa.antonio12No ratings yet
- Forro Intestinal ObstructionDocument3 pagesForro Intestinal ObstructionShiehan Mae ForroNo ratings yet
- Mirana BSN2-7 NCPDocument3 pagesMirana BSN2-7 NCPCrystal MiranaNo ratings yet
- NCP ADocument2 pagesNCP AMarithe Joi Abarico AberosNo ratings yet
- Group-5 NCM-107 NCPDocument4 pagesGroup-5 NCM-107 NCPbulok netflakes100% (1)
- HydroceleDocument10 pagesHydroceleRyan ReNo ratings yet
- Concept Map Good ExampleDocument1 pageConcept Map Good Examplekellymk2584No ratings yet
- Uti Nursing Care Plan FinalDocument18 pagesUti Nursing Care Plan FinalAmit RanjanNo ratings yet
- Ehr PDFDocument31 pagesEhr PDFNicolai MabituinNo ratings yet
- NCP & DSDocument4 pagesNCP & DSKyla Marie TejadaNo ratings yet
- NCP With Eval Dewara BSN3FDocument2 pagesNCP With Eval Dewara BSN3FPrincess Faniega SugatonNo ratings yet
- Patient Name: Lorna Dimagiba Age: 84 Years Old Gender: Female C.S: Widow BED#: #1Document3 pagesPatient Name: Lorna Dimagiba Age: 84 Years Old Gender: Female C.S: Widow BED#: #1Girlie MebañaNo ratings yet
- SKYLA FIESTA NCP (Acute Pancreatitis)Document4 pagesSKYLA FIESTA NCP (Acute Pancreatitis)Skyla FiestaNo ratings yet
- NCP Kenezo, Female 17Document2 pagesNCP Kenezo, Female 17labanesstephanyNo ratings yet
- NCP Ectopic-Pregnancy1Document9 pagesNCP Ectopic-Pregnancy1Jullian PloyaNo ratings yet
- ASSESSMENT SummerDocument1 pageASSESSMENT SummerThoyotsukha Faeldan123No ratings yet
- NCP G7Document2 pagesNCP G7katt.edlessNo ratings yet
- Appendix D Nursing Care PlanDocument8 pagesAppendix D Nursing Care PlanVinz OñoNo ratings yet
- Postpartum SimulationDocument2 pagesPostpartum SimulationEarly SaribaNo ratings yet
- Soak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyFrom EverandSoak It In: Hydrotherapy Treatments In 20 Minutes or Less for Health and BeautyNo ratings yet
- 14-54 8m-Inetermediate-3Document10 pages14-54 8m-Inetermediate-3epdsan3dNo ratings yet
- 18CS731Document438 pages18CS731Sangeetha NNo ratings yet
- Online Marketing EssentialsDocument508 pagesOnline Marketing EssentialsElena BotezatuNo ratings yet
- Science Internet ResourcesDocument4 pagesScience Internet ResourcesGabriela D CostescuNo ratings yet
- Course Curriculum of PGP Renewable EnergyDocument6 pagesCourse Curriculum of PGP Renewable EnergyRonanki RaviNo ratings yet
- Finding and Correcting Mistakes Exercise 1. The Boss From HellDocument6 pagesFinding and Correcting Mistakes Exercise 1. The Boss From HellKhiêm Trần ThịNo ratings yet
- MDR11 InstructionsDocument4 pagesMDR11 Instructionsjuan tellezNo ratings yet
- Total Marks: 25 Duration: One Hour: Xii-Msths Case Study Questions - Test Term-IDocument8 pagesTotal Marks: 25 Duration: One Hour: Xii-Msths Case Study Questions - Test Term-ISABARI SRINIVAS ANo ratings yet
- Tilt TableDocument2 pagesTilt TablenikhilNo ratings yet
- Evangelism 1Document4 pagesEvangelism 1Horace Owiti O.No ratings yet
- Safety Instrumented Systems: GlobalDocument410 pagesSafety Instrumented Systems: Globalmohammed el erianNo ratings yet
- Smoke DetectorDocument1 pageSmoke DetectorTarikNo ratings yet
- A289A289M-97 (2013) Standard Specification For Alloy Steel Forgings For Nonmagnetic Retaining Rings For GeneratorsDocument3 pagesA289A289M-97 (2013) Standard Specification For Alloy Steel Forgings For Nonmagnetic Retaining Rings For GeneratorsShico1983No ratings yet
- Unit 7-Chemical Reactions NotesDocument55 pagesUnit 7-Chemical Reactions Notesapi-182809945No ratings yet
- 216B2, 226B2, 232B2, 236B2, 242B2, Electrical System 247B2 and 257B2 Multi-Terrain Loader and 252B2 Skid Steer LoaderDocument4 pages216B2, 226B2, 232B2, 236B2, 242B2, Electrical System 247B2 and 257B2 Multi-Terrain Loader and 252B2 Skid Steer LoaderAirton SenaNo ratings yet
- PC/SC Partial Documentation of The API: PMDZ061-AE 24/09/2009Document32 pagesPC/SC Partial Documentation of The API: PMDZ061-AE 24/09/2009manskebe6121No ratings yet
- Surface Preparation Standards JotunDocument2 pagesSurface Preparation Standards JotunbacabacabacaNo ratings yet
- What Is Big DataDocument2 pagesWhat Is Big DatasanjnaNo ratings yet
- IT 16 - Neurogenic Bladder - SMDocument31 pagesIT 16 - Neurogenic Bladder - SMRurie Awalia SuhardiNo ratings yet
- 2023 - ECON422 - TURKISH ECONOMY - HOMEWORK - Final VersionDocument3 pages2023 - ECON422 - TURKISH ECONOMY - HOMEWORK - Final VersionsenaNo ratings yet
- Internet Banking (E-Banking)Document16 pagesInternet Banking (E-Banking)Saurabh G0% (2)
- Filtration Solution To Problems - Pdf-Midterm-Exam-AnswerDocument7 pagesFiltration Solution To Problems - Pdf-Midterm-Exam-AnswerDubu Kim100% (1)
- 61cm InfoDocument4 pages61cm InfoHow to do anything By HimanshuNo ratings yet
- PHD Syllabus AMUDocument2 pagesPHD Syllabus AMUMohd ShahidNo ratings yet
- Volume 7 No 8 2018Document142 pagesVolume 7 No 8 2018Salhi AmaraNo ratings yet
- System Path VariablesDocument5 pagesSystem Path VariablesUnessNo ratings yet
- Gravimetric Determination of Barium SulfateDocument3 pagesGravimetric Determination of Barium SulfateArmiee InfiniteNo ratings yet
- DB Nutrition GuideDocument59 pagesDB Nutrition GuideBárbara Leite100% (2)