
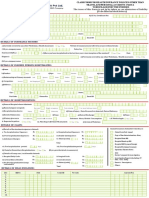
Page From Insured
Page From Insured
You might also like
- Sub-Dispatcher Agreement: ARNDTECH Solutions IncDocument2 pagesSub-Dispatcher Agreement: ARNDTECH Solutions IncNaveed Shehriyar BaigNo ratings yet
- Principles of Risk Management and Insurance: Global EditionDocument18 pagesPrinciples of Risk Management and Insurance: Global EditionAHMAD ALI100% (1)
- IRDA - Claim Form-2Document1 pageIRDA - Claim Form-2Sunny bNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyArunsNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Medi Assist - Claim FormDocument4 pagesMedi Assist - Claim FormMAHESH PATLENo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormVeena K VNo ratings yet
- ClaimFormDocument4 pagesClaimFormharshaapple007No ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Reimbursement Claim Form-1Document7 pagesReimbursement Claim Form-1Mayuresh DalviNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part AkannagamNo ratings yet
- ReimbursementFormA B2016Document7 pagesReimbursementFormA B2016DESIGN CGMPNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- MD India Forms & Policy DocumentDocument42 pagesMD India Forms & Policy DocumentYagantiGaneshRaghuveerNo ratings yet
- Health Claim Form Part BDocument3 pagesHealth Claim Form Part BShubham PandeyNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicySudipta DeNo ratings yet
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone No ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormOmpalNo ratings yet
- ClaimFormDocument6 pagesClaimFormKanhaiya Lal SahuNo ratings yet
- Reimbursement CLaim Form IRDADocument5 pagesReimbursement CLaim Form IRDADhaval ThakkarNo ratings yet
- Claim Registered 26 11 2023 12 16 35 PM 478373Document3 pagesClaim Registered 26 11 2023 12 16 35 PM 4783732K19-CO-026 Abhishek TyagiNo ratings yet
- Aditya Birla Health Insurance Co. LimitedDocument4 pagesAditya Birla Health Insurance Co. LimitedAdeep MathurNo ratings yet
- CARE FORM - ReimbuDocument12 pagesCARE FORM - ReimbuPradyumna Singh RathoreNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Health Insurance Claim FormDocument4 pagesHealth Insurance Claim Formaditya TestNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyMruthunjaya Reddy LakkamNo ratings yet
- United India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim FormDocument2 pagesUnited India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim Form'Θκ'βύτ-Ίισνέγσύ.No ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistorySwapnil NageNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Physiomodalities Catlog NewDocument2 pagesPhysiomodalities Catlog NewRKNo ratings yet
- Secure (Personal Accident Insurance Product) Claim FormDocument10 pagesSecure (Personal Accident Insurance Product) Claim Formmestry.om05No ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- Health Insurance - Claim Form - Part A (To Be Filled by Insured)Document4 pagesHealth Insurance - Claim Form - Part A (To Be Filled by Insured)Shaikh AyyubNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Health Claim Form - EnglishDocument11 pagesHealth Claim Form - Englishharsh sahuNo ratings yet
- Pravasi Bharatiya Bima YojanaDocument2 pagesPravasi Bharatiya Bima YojanaMadhava Reddy MunagalaNo ratings yet
- Claim Form & Other Documents To Be Submitted To Lic Branch/ Divisional Offices OnlyDocument1 pageClaim Form & Other Documents To Be Submitted To Lic Branch/ Divisional Offices OnlyAnonymous W9VINoTza100% (1)
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Claim Form - Part A & BDocument5 pagesClaim Form - Part A & BNauman MalikNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- MediPrime Claim FormDocument8 pagesMediPrime Claim Formrahul0105100% (1)
- Reimbursement A PDFDocument4 pagesReimbursement A PDFAniruddha ShivalNo ratings yet
- Details of Primary Insured: Bajaj Allianz General Insurance Company LimitedDocument3 pagesDetails of Primary Insured: Bajaj Allianz General Insurance Company LimitedBellapu Durga vara prasadNo ratings yet
- Reliance Claim Form BDocument2 pagesReliance Claim Form BAbhay HarkanchiNo ratings yet
- Claim Form Part ADocument8 pagesClaim Form Part AJos'fAntonyRinoNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- Understanding Named, Automatic and Additional Insureds in the CGL PolicyFrom EverandUnderstanding Named, Automatic and Additional Insureds in the CGL PolicyNo ratings yet
- Obamacare: Complete Law, Latest Statistics & Republican's CounterproposalFrom EverandObamacare: Complete Law, Latest Statistics & Republican's CounterproposalNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- Process of Filing ITR-1 Under New Income Tax E-Filing Portal 2.0Document19 pagesProcess of Filing ITR-1 Under New Income Tax E-Filing Portal 2.0Narayanan RNo ratings yet
- Documents Used in International TradeDocument31 pagesDocuments Used in International Tradeelite76No ratings yet
- Fundamental and Technical Anlaysis of Private Bank SectorDocument51 pagesFundamental and Technical Anlaysis of Private Bank SectorShirish TawdeNo ratings yet
- ReportDocument19 pagesReportGambar GambarNo ratings yet
- Appl Form OCLDocument2 pagesAppl Form OCLNikki Gaskins CampbellNo ratings yet
- TYBCOM Direct Tax (INTRODUCTION & DEDUCTION)Document6 pagesTYBCOM Direct Tax (INTRODUCTION & DEDUCTION)jay prakeshNo ratings yet
- Board Clerk AgreementDocument7 pagesBoard Clerk AgreementKyle PfannenstielNo ratings yet
- PRUShield eBrochure-Apr2020 PDFDocument21 pagesPRUShield eBrochure-Apr2020 PDFC KNo ratings yet
- Star Health Denial LetterDocument3 pagesStar Health Denial LettersabumathewNo ratings yet
- Benefit Illustration - Metlife Guaranteed Savings Plan (Uin No. 117N096V01)Document6 pagesBenefit Illustration - Metlife Guaranteed Savings Plan (Uin No. 117N096V01)NAVEEN CHANDRANo ratings yet
- TIA 2/FM Seminar A.2 ProblemsDocument36 pagesTIA 2/FM Seminar A.2 ProblemsPrisco Say100% (1)
- Intangible Assets (Chapter 4)Document14 pagesIntangible Assets (Chapter 4)Atif KhosoNo ratings yet
- Nyse FFG 2005Document140 pagesNyse FFG 2005Bijoy AhmedNo ratings yet
- Swim Waver FormDocument2 pagesSwim Waver FormSelva NarayNo ratings yet
- CH 03Document71 pagesCH 03martinus linggo100% (1)
- Requirements For The Release of Title 123456Document1 pageRequirements For The Release of Title 123456Junnel Ninto LptNo ratings yet
- Proforma To Be Executed On A Rs.20/-Non-Judicial Stamp Paper If The Dividend Is Rs.2500/ - and AboveDocument1 pageProforma To Be Executed On A Rs.20/-Non-Judicial Stamp Paper If The Dividend Is Rs.2500/ - and AboveKarthi KeyanNo ratings yet
- Case Digest AssignmentDocument5 pagesCase Digest AssignmentRikka ReyesNo ratings yet
- Employment: Complete An Employment' Page For Each Employment or DirectorshipDocument2 pagesEmployment: Complete An Employment' Page For Each Employment or DirectorshipDick WilliamsNo ratings yet
- Chapter 06 - Share of Profit From Association of PersonsDocument6 pagesChapter 06 - Share of Profit From Association of PersonsSuniel JamilNo ratings yet
- Only Statement 1Document45 pagesOnly Statement 1Helen AlvaradoNo ratings yet
- A Study in Mutual Funds in IndiaDocument91 pagesA Study in Mutual Funds in IndiaNazir Ahmad AmirNo ratings yet
- Quiz+Answer+Key++11 23 2021Document5 pagesQuiz+Answer+Key++11 23 2021cgstvqf6g9No ratings yet
- Religare Enterprises LTD - Annual ReportDocument383 pagesReligare Enterprises LTD - Annual ReportPujitNo ratings yet
- CORITANA Research 1Document2 pagesCORITANA Research 1Jade CoritanaNo ratings yet
- PD No. 1460, As Amended by RA 10607: Insurance LawDocument35 pagesPD No. 1460, As Amended by RA 10607: Insurance Lawmarizenoc100% (1)
- Bajaj Future Gain Web PDFDocument17 pagesBajaj Future Gain Web PDFPhanindra YellapragadaNo ratings yet
- Life Insurance MCQ Guide For IC 38Document17 pagesLife Insurance MCQ Guide For IC 38Shahnawaz AnsariNo ratings yet
























































































Download as pdf or txt
You might also like
- Sub-Dispatcher Agreement: ARNDTECH Solutions IncDocument2 pagesSub-Dispatcher Agreement: ARNDTECH Solutions IncNaveed Shehriyar BaigNo ratings yet
- Principles of Risk Management and Insurance: Global EditionDocument18 pagesPrinciples of Risk Management and Insurance: Global EditionAHMAD ALI100% (1)
- IRDA - Claim Form-2Document1 pageIRDA - Claim Form-2Sunny bNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyArunsNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Medi Assist - Claim FormDocument4 pagesMedi Assist - Claim FormMAHESH PATLENo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormVeena K VNo ratings yet
- ClaimFormDocument4 pagesClaimFormharshaapple007No ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Reimbursement Claim Form-1Document7 pagesReimbursement Claim Form-1Mayuresh DalviNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part AkannagamNo ratings yet
- ReimbursementFormA B2016Document7 pagesReimbursementFormA B2016DESIGN CGMPNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- MD India Forms & Policy DocumentDocument42 pagesMD India Forms & Policy DocumentYagantiGaneshRaghuveerNo ratings yet
- Health Claim Form Part BDocument3 pagesHealth Claim Form Part BShubham PandeyNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicySudipta DeNo ratings yet
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone No ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- Reimbursement Claim FormDocument2 pagesReimbursement Claim FormOmpalNo ratings yet
- ClaimFormDocument6 pagesClaimFormKanhaiya Lal SahuNo ratings yet
- Reimbursement CLaim Form IRDADocument5 pagesReimbursement CLaim Form IRDADhaval ThakkarNo ratings yet
- Claim Registered 26 11 2023 12 16 35 PM 478373Document3 pagesClaim Registered 26 11 2023 12 16 35 PM 4783732K19-CO-026 Abhishek TyagiNo ratings yet
- Aditya Birla Health Insurance Co. LimitedDocument4 pagesAditya Birla Health Insurance Co. LimitedAdeep MathurNo ratings yet
- CARE FORM - ReimbuDocument12 pagesCARE FORM - ReimbuPradyumna Singh RathoreNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Health Insurance Claim FormDocument4 pagesHealth Insurance Claim Formaditya TestNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyMruthunjaya Reddy LakkamNo ratings yet
- United India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim FormDocument2 pagesUnited India Insurance Co. LTD.,: Mediclaim Insurance Policy Reimbursement Claim Form'Θκ'βύτ-Ίισνέγσύ.No ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistorySwapnil NageNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Physiomodalities Catlog NewDocument2 pagesPhysiomodalities Catlog NewRKNo ratings yet
- Secure (Personal Accident Insurance Product) Claim FormDocument10 pagesSecure (Personal Accident Insurance Product) Claim Formmestry.om05No ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- Health Insurance - Claim Form - Part A (To Be Filled by Insured)Document4 pagesHealth Insurance - Claim Form - Part A (To Be Filled by Insured)Shaikh AyyubNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Health Claim Form - EnglishDocument11 pagesHealth Claim Form - Englishharsh sahuNo ratings yet
- Pravasi Bharatiya Bima YojanaDocument2 pagesPravasi Bharatiya Bima YojanaMadhava Reddy MunagalaNo ratings yet
- Claim Form & Other Documents To Be Submitted To Lic Branch/ Divisional Offices OnlyDocument1 pageClaim Form & Other Documents To Be Submitted To Lic Branch/ Divisional Offices OnlyAnonymous W9VINoTza100% (1)
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Claim Form - Part A & BDocument5 pagesClaim Form - Part A & BNauman MalikNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- MediPrime Claim FormDocument8 pagesMediPrime Claim Formrahul0105100% (1)
- Reimbursement A PDFDocument4 pagesReimbursement A PDFAniruddha ShivalNo ratings yet
- Details of Primary Insured: Bajaj Allianz General Insurance Company LimitedDocument3 pagesDetails of Primary Insured: Bajaj Allianz General Insurance Company LimitedBellapu Durga vara prasadNo ratings yet
- Reliance Claim Form BDocument2 pagesReliance Claim Form BAbhay HarkanchiNo ratings yet
- Claim Form Part ADocument8 pagesClaim Form Part AJos'fAntonyRinoNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- Understanding Named, Automatic and Additional Insureds in the CGL PolicyFrom EverandUnderstanding Named, Automatic and Additional Insureds in the CGL PolicyNo ratings yet
- Obamacare: Complete Law, Latest Statistics & Republican's CounterproposalFrom EverandObamacare: Complete Law, Latest Statistics & Republican's CounterproposalNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- Process of Filing ITR-1 Under New Income Tax E-Filing Portal 2.0Document19 pagesProcess of Filing ITR-1 Under New Income Tax E-Filing Portal 2.0Narayanan RNo ratings yet
- Documents Used in International TradeDocument31 pagesDocuments Used in International Tradeelite76No ratings yet
- Fundamental and Technical Anlaysis of Private Bank SectorDocument51 pagesFundamental and Technical Anlaysis of Private Bank SectorShirish TawdeNo ratings yet
- ReportDocument19 pagesReportGambar GambarNo ratings yet
- Appl Form OCLDocument2 pagesAppl Form OCLNikki Gaskins CampbellNo ratings yet
- TYBCOM Direct Tax (INTRODUCTION & DEDUCTION)Document6 pagesTYBCOM Direct Tax (INTRODUCTION & DEDUCTION)jay prakeshNo ratings yet
- Board Clerk AgreementDocument7 pagesBoard Clerk AgreementKyle PfannenstielNo ratings yet
- PRUShield eBrochure-Apr2020 PDFDocument21 pagesPRUShield eBrochure-Apr2020 PDFC KNo ratings yet
- Star Health Denial LetterDocument3 pagesStar Health Denial LettersabumathewNo ratings yet
- Benefit Illustration - Metlife Guaranteed Savings Plan (Uin No. 117N096V01)Document6 pagesBenefit Illustration - Metlife Guaranteed Savings Plan (Uin No. 117N096V01)NAVEEN CHANDRANo ratings yet
- TIA 2/FM Seminar A.2 ProblemsDocument36 pagesTIA 2/FM Seminar A.2 ProblemsPrisco Say100% (1)
- Intangible Assets (Chapter 4)Document14 pagesIntangible Assets (Chapter 4)Atif KhosoNo ratings yet
- Nyse FFG 2005Document140 pagesNyse FFG 2005Bijoy AhmedNo ratings yet
- Swim Waver FormDocument2 pagesSwim Waver FormSelva NarayNo ratings yet
- CH 03Document71 pagesCH 03martinus linggo100% (1)
- Requirements For The Release of Title 123456Document1 pageRequirements For The Release of Title 123456Junnel Ninto LptNo ratings yet
- Proforma To Be Executed On A Rs.20/-Non-Judicial Stamp Paper If The Dividend Is Rs.2500/ - and AboveDocument1 pageProforma To Be Executed On A Rs.20/-Non-Judicial Stamp Paper If The Dividend Is Rs.2500/ - and AboveKarthi KeyanNo ratings yet
- Case Digest AssignmentDocument5 pagesCase Digest AssignmentRikka ReyesNo ratings yet
- Employment: Complete An Employment' Page For Each Employment or DirectorshipDocument2 pagesEmployment: Complete An Employment' Page For Each Employment or DirectorshipDick WilliamsNo ratings yet
- Chapter 06 - Share of Profit From Association of PersonsDocument6 pagesChapter 06 - Share of Profit From Association of PersonsSuniel JamilNo ratings yet
- Only Statement 1Document45 pagesOnly Statement 1Helen AlvaradoNo ratings yet
- A Study in Mutual Funds in IndiaDocument91 pagesA Study in Mutual Funds in IndiaNazir Ahmad AmirNo ratings yet
- Quiz+Answer+Key++11 23 2021Document5 pagesQuiz+Answer+Key++11 23 2021cgstvqf6g9No ratings yet
- Religare Enterprises LTD - Annual ReportDocument383 pagesReligare Enterprises LTD - Annual ReportPujitNo ratings yet
- CORITANA Research 1Document2 pagesCORITANA Research 1Jade CoritanaNo ratings yet
- PD No. 1460, As Amended by RA 10607: Insurance LawDocument35 pagesPD No. 1460, As Amended by RA 10607: Insurance Lawmarizenoc100% (1)
- Bajaj Future Gain Web PDFDocument17 pagesBajaj Future Gain Web PDFPhanindra YellapragadaNo ratings yet
- Life Insurance MCQ Guide For IC 38Document17 pagesLife Insurance MCQ Guide For IC 38Shahnawaz AnsariNo ratings yet