Download as pdf or txt
You might also like
- Maxillary Injection Techniques PPT I Sas 11-14Document45 pagesMaxillary Injection Techniques PPT I Sas 11-14mavirosemandawe08No ratings yet
- BLoC Case Study Colgate 2021Document6 pagesBLoC Case Study Colgate 2021NAVEEN SNo ratings yet
- Biomedical Final PaperDocument6 pagesBiomedical Final PaperMiss DNo ratings yet
- PPM Informed Consent in Anesthesia WITH FORMSDocument10 pagesPPM Informed Consent in Anesthesia WITH FORMSbalab2311No ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi100% (4)
- RPD Questions For ExamDocument5 pagesRPD Questions For ExamKatarina Skodra0% (1)
- Running Head: Research and Evidence: Support The Need For A Change 1Document6 pagesRunning Head: Research and Evidence: Support The Need For A Change 1writemyessay freeNo ratings yet
- Ethics Assignment: Libyan International Medical University Faculty of DentistryDocument6 pagesEthics Assignment: Libyan International Medical University Faculty of DentistryMazen T. ShembeshNo ratings yet
- BAPSDocument21 pagesBAPSayron600No ratings yet
- Medical Ethics NotesDocument11 pagesMedical Ethics NotesMuhammad Waqar RehanNo ratings yet
- Ethical Dilemmas in End of Life CareDocument41 pagesEthical Dilemmas in End of Life Careوجد عمرNo ratings yet
- Ethical Issues in Palliative CareDocument16 pagesEthical Issues in Palliative CarevassalliNo ratings yet
- 2-3 Samillano-SamontegeronDocument19 pages2-3 Samillano-SamontegeronLance_Joshua_7907No ratings yet
- Section Five - Practice ManagementDocument15 pagesSection Five - Practice ManagementKomal TalrejaNo ratings yet
- Fiel Angelo G. Mallari, RNDocument68 pagesFiel Angelo G. Mallari, RNfiel mallariNo ratings yet
- Lesson 2:: Medical ANDDocument38 pagesLesson 2:: Medical ANDKAH' CHISMISSNo ratings yet
- 08 PDFDocument16 pages08 PDFMădălina RădulescuNo ratings yet
- ##2022 Informed Consent NotesDocument11 pages##2022 Informed Consent NotesSANTHIYA A/P MOHANA SUNDARAM MoeNo ratings yet
- Informed ConsentDocument24 pagesInformed ConsentNoona PlaysNo ratings yet
- AD Advis Visor ORY YDocument4 pagesAD Advis Visor ORY YAhmadNo ratings yet
- Maybe Not For Me: Ethics in OrthodonticsDocument1 pageMaybe Not For Me: Ethics in OrthodonticsDominikaSkórkaNo ratings yet
- Ethical Legal IssuesDocument29 pagesEthical Legal IssueslisalovNo ratings yet
- Rle TypeDocument15 pagesRle TypeMajkel Benche CustodioNo ratings yet
- Legal and Ethical Issues in GeriatricsDocument5 pagesLegal and Ethical Issues in GeriatricsStephy Sojan100% (2)
- Decision MakingDocument13 pagesDecision Makingsyafi'udinNo ratings yet
- Bioethics Lesson 3Document11 pagesBioethics Lesson 3Jewell Nivera CarpioNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument8 pagesDr. Ali's Uworld Notes For Step 2 CKnaimNo ratings yet
- Admission Procedure For The Critically Ill PatientDocument3 pagesAdmission Procedure For The Critically Ill Patientgeorgeloto12100% (1)
- Beneficence and AutonomyDocument3 pagesBeneficence and AutonomyJini Donguines GulmaticoNo ratings yet
- Ethics Short Essay 3Document4 pagesEthics Short Essay 3api-284664489No ratings yet
- What Is Informed ConsentDocument2 pagesWhat Is Informed ConsentMerva LaurenteNo ratings yet
- The Underlying Principles of Ethical Patient CareDocument7 pagesThe Underlying Principles of Ethical Patient CareGulshanNo ratings yet
- Access To Special Care Dentistry, Part 3. Consent and CapacityDocument11 pagesAccess To Special Care Dentistry, Part 3. Consent and CapacityMostafa FayadNo ratings yet
- Informed ConsentDocument4 pagesInformed Consentnnaesor_1091No ratings yet
- Autonomy & VeracityDocument3 pagesAutonomy & VeracityLovie Japhet LopezNo ratings yet
- Definition of Ethics in Dental ClinicDocument6 pagesDefinition of Ethics in Dental Clinichazemelpop26No ratings yet
- Dashboard Library Study Plans Qbank Analysis Account Help Center & Legal InfoDocument42 pagesDashboard Library Study Plans Qbank Analysis Account Help Center & Legal InfoGauri SurnerNo ratings yet
- Two Ethics Case ScenariosDocument3 pagesTwo Ethics Case ScenariosEguia NielNo ratings yet
- Legal and Ethical Considerations of Informed ConsentDocument16 pagesLegal and Ethical Considerations of Informed ConsentKim DimaanoNo ratings yet
- Theology 3 FinalDocument3 pagesTheology 3 FinalCharlene BinaraoNo ratings yet
- Earl Scenario 1Document2 pagesEarl Scenario 1Elaiza HerreraNo ratings yet
- Principles of Healthcare EthicsDocument15 pagesPrinciples of Healthcare EthicsSaddamix AL OmariNo ratings yet
- 2011 08 Bioethics Benefecience TranxDocument3 pages2011 08 Bioethics Benefecience TranxdtimtimanNo ratings yet
- Informed Consent and Informed Refusal in Dentistry: by Dianne Glasscoe Watterson, RDH, BS, MbaDocument10 pagesInformed Consent and Informed Refusal in Dentistry: by Dianne Glasscoe Watterson, RDH, BS, MbaSanniie NuansaNo ratings yet
- Key Principles in Dental EthicsDocument4 pagesKey Principles in Dental EthicsNuzullia JamalNo ratings yet
- Informed Consent As An Ethical Issue in NursingDocument4 pagesInformed Consent As An Ethical Issue in NursingJIMOH Shamsudeen JideNo ratings yet
- How Is Advance Care Planning Different From Advance Directives?Document109 pagesHow Is Advance Care Planning Different From Advance Directives?BGNo ratings yet
- BioethicsDocument110 pagesBioethicsvincent_tang_30No ratings yet
- AutonomyDocument3 pagesAutonomyMae Jane AuzaNo ratings yet
- Solving Ethical Dilemmas in Dental Hygiene Practice: by Marcy Ortiz, RDH, BADocument11 pagesSolving Ethical Dilemmas in Dental Hygiene Practice: by Marcy Ortiz, RDH, BAHAMIDNo ratings yet
- Beginning and Ending of DoctorDocument3 pagesBeginning and Ending of DoctorShahrulazman_J_5980No ratings yet
- Ethical Matters in PsychiatryDocument19 pagesEthical Matters in PsychiatryZainab Ali HassanNo ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi0% (1)
- Ethics L2Document63 pagesEthics L2Karim ElmakasNo ratings yet
- Physician Integrity: Why It Is InviolableDocument3 pagesPhysician Integrity: Why It Is InviolableAndrea Villagran100% (1)
- Doctor Patient RelationshipDocument58 pagesDoctor Patient RelationshipPavan chowdaryNo ratings yet
- Sxetika Me Palliative CareDocument2 pagesSxetika Me Palliative CareKatrin DemertziNo ratings yet
- Ethics &medico Legal in Obg GynDocument26 pagesEthics &medico Legal in Obg GynSastry Bsrln100% (2)
- PracticeDocument4 pagesPracticejinny1_0No ratings yet
- MARCOS - Legal Issues of ElderlyDocument2 pagesMARCOS - Legal Issues of ElderlyArian May MarcosNo ratings yet
- Guideline On Informed Consent: Originating Council Review Council Adopted RevisedDocument3 pagesGuideline On Informed Consent: Originating Council Review Council Adopted RevisedMonaNo ratings yet
- Ethics in Medical PracticeDocument35 pagesEthics in Medical PracticeMohammed AadeelNo ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- Int Endodontic J - 2022 - Matoug Elwerfelli - Vital Pulp Treatment For Traumatized Permanent Teeth A Systematic ReviewDocument17 pagesInt Endodontic J - 2022 - Matoug Elwerfelli - Vital Pulp Treatment For Traumatized Permanent Teeth A Systematic Review吳國豪No ratings yet
- Andreasen 1971Document64 pagesAndreasen 1971crispompittas41No ratings yet
- 1107 11410802081G PDFDocument8 pages1107 11410802081G PDFBlack EyeNo ratings yet
- Clinical Evaluation of A New Bonded Space MaintainerDocument7 pagesClinical Evaluation of A New Bonded Space Maintainerpaper kitaNo ratings yet
- Sivakumar 2012Document5 pagesSivakumar 2012Adriiana Jaimes JaimesNo ratings yet
- Trabajo de Aula de Inmersion Guia 16 Correccion Manuel Alejandro Reyes Galindo 803)Document3 pagesTrabajo de Aula de Inmersion Guia 16 Correccion Manuel Alejandro Reyes Galindo 803)Manuel Alejandro Reyes GalindoNo ratings yet
- CXX PDFDocument5 pagesCXX PDFKty SinistNo ratings yet
- Composite PDFDocument5 pagesComposite PDFruchikaNo ratings yet
- 2.malaysian Guidelines On Radiation Safety in Dentistry PDFDocument33 pages2.malaysian Guidelines On Radiation Safety in Dentistry PDFMahdy AlShammariNo ratings yet
- Ansari 1997Document4 pagesAnsari 1997SkAliHassanNo ratings yet
- Philosophies of RPD DesigningDocument8 pagesPhilosophies of RPD DesigningThenmozhiNo ratings yet
- Dentofacial Effects of Asymmetric Headgear and Cervical Headgear With Removable Plate On Unilateral Molar DistalizationDocument9 pagesDentofacial Effects of Asymmetric Headgear and Cervical Headgear With Removable Plate On Unilateral Molar Distalizationaa bbNo ratings yet
- Pre-Activity: Saint Augustine SchoolDocument6 pagesPre-Activity: Saint Augustine SchoolShaina AragonNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument8 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Treatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceDocument9 pagesTreatment of An Ankylosed Central Incisor by Single Tooth Dento-Osseous Osteotomy and A Simple Distraction DeviceJuan Carlos MeloNo ratings yet
- Lecture - 6-4 - Methods of The Pulpitis TreatmentDocument35 pagesLecture - 6-4 - Methods of The Pulpitis TreatmentA.J. YounesNo ratings yet
- Dentinal Hypersensitivity: Guided By: Dr.P.Karunakar DR - Umrana Faizuddin DR - Ashish JainDocument144 pagesDentinal Hypersensitivity: Guided By: Dr.P.Karunakar DR - Umrana Faizuddin DR - Ashish Jainrasagna reddyNo ratings yet
- Advantages and Disadvantages of Rotary Niti Advantages DisadvantagesDocument3 pagesAdvantages and Disadvantages of Rotary Niti Advantages DisadvantagesheenalvNo ratings yet
- 10 1016@j JDSR 2020 08 003Document8 pages10 1016@j JDSR 2020 08 003maulana harahapNo ratings yet
- A Modification To The Incisor Classification of MalocclusionDocument5 pagesA Modification To The Incisor Classification of Malocclusioneden elza thomasNo ratings yet
- Extrusion of Debris From Primary Molar Root Canals Following Instrumentation With Traditional and New File SystemsDocument6 pagesExtrusion of Debris From Primary Molar Root Canals Following Instrumentation With Traditional and New File Systemssyed fazluddinNo ratings yet
- FCD (SA) Orthod Part II Past Papers - 2012 Mar 19-3-2014Document2 pagesFCD (SA) Orthod Part II Past Papers - 2012 Mar 19-3-2014matentenNo ratings yet
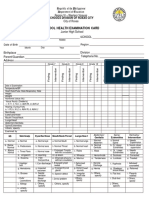
- School Health Examination Form EDITEDDocument2 pagesSchool Health Examination Form EDITEDjustine mae villaruelNo ratings yet
- Document (Denture Over Denture)Document39 pagesDocument (Denture Over Denture)Saifurahman TarakiNo ratings yet
- Kim2017.Pdfmarginal and Internal Gaps of Cobalt-Chromium (Co-Cr) Alloy Copings Fabricated Using Subtractive and Additive ManufacturingDocument9 pagesKim2017.Pdfmarginal and Internal Gaps of Cobalt-Chromium (Co-Cr) Alloy Copings Fabricated Using Subtractive and Additive ManufacturingdentureNo ratings yet
- NHS Greater Glasgow & Clyde Medical Staffing Guide To Clinical AttachmentsDocument3 pagesNHS Greater Glasgow & Clyde Medical Staffing Guide To Clinical AttachmentsUma MounaNo ratings yet
- Aditek Catalogue Ed.04 - EnglishDocument64 pagesAditek Catalogue Ed.04 - EnglishhabeebNo ratings yet