Download as pdf or txt
You might also like
- Pediatric Drugs MKDDocument3 pagesPediatric Drugs MKDquixoticdreamer100% (7)
- Case Investigation Forms - Pidsrmop3ed 1Document16 pagesCase Investigation Forms - Pidsrmop3ed 1RHU Dupax del Sur100% (3)
- Measles CIF 2014Document2 pagesMeasles CIF 2014RionaMarieMagbutayNo ratings yet
- MuscleHack Supplement Guide PDFDocument44 pagesMuscleHack Supplement Guide PDFJohn BeckettNo ratings yet
- Case Investigation Form - Measles-RubellaDocument2 pagesCase Investigation Form - Measles-Rubellaclaverialc10No ratings yet
- Case Report Form For HFMDDocument2 pagesCase Report Form For HFMDMendez RhuNo ratings yet
- CRF HFMD AsmghDocument2 pagesCRF HFMD AsmghRyeowook RyeNo ratings yet
- Cif Zika - 2016 PDFDocument3 pagesCif Zika - 2016 PDFNicholai CabadduNo ratings yet
- Cif NTDocument2 pagesCif NTIvy marie BonNo ratings yet
- CDC Covid-19 Report FormDocument2 pagesCDC Covid-19 Report FormiggybauNo ratings yet
- Measles Case Reporting Form I.Case Identification/ Demographic DetailsDocument2 pagesMeasles Case Reporting Form I.Case Identification/ Demographic DetailsActivity ManagerNo ratings yet
- Pui FormDocument2 pagesPui FormBotez ElviraNo ratings yet
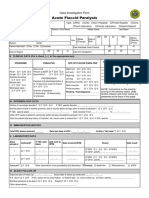
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormPaul Angelo E. Caliva0% (1)
- Case Investigation Form - Acute Flaccid ParalysisDocument2 pagesCase Investigation Form - Acute Flaccid Paralysisclaverialc10No ratings yet
- Barangay Assisted Booking Form: CODE: D1ADocument4 pagesBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNo ratings yet
- ReportForm TyphoidDocument2 pagesReportForm TyphoidSundarajan ManiNo ratings yet
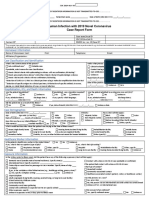
- Human Infection With 2019 Novel Coronavirus Case Report FormDocument2 pagesHuman Infection With 2019 Novel Coronavirus Case Report FormRicardo F. BernardinelliNo ratings yet
- SBI Recording Form 1Document12 pagesSBI Recording Form 1Maybel Din0% (1)
- Medical Attendants Certificate17062019Document2 pagesMedical Attendants Certificate17062019PrathameshNo ratings yet
- Discharge Planning TBDocument2 pagesDischarge Planning TBNurida LatipahNo ratings yet
- Cuestionario de SaludDocument1 pageCuestionario de SaludLuis Sosa GodoyNo ratings yet
- Acute Flaccid Paralysis: Case Investigation FormDocument2 pagesAcute Flaccid Paralysis: Case Investigation FormBarbie CincoNo ratings yet
- RabiesDocument2 pagesRabiesninzah wanzahNo ratings yet
- Malaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)Document2 pagesMalaria Case Surveillance Report: Yrs. Mos. Wks. Days (Circle Units)Pramod gameNo ratings yet
- Viral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDDocument3 pagesViral Haemorrhagic Fever - Case Investigation Form: Date of Detection of The Case Case IDSalihu MustaphaNo ratings yet
- FP Form1 V3.0 2016Document3 pagesFP Form1 V3.0 2016Lorenz Joey Ricarte100% (2)
- 11 Trauma Emergency Form 19102023Document2 pages11 Trauma Emergency Form 19102023Marjorie BricenioNo ratings yet
- Recording Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationDocument1 pageRecording Form 1: Masterlist of Grade 1 Students: School-Based ImmunizationJesse100% (1)
- FWRI Form ReviseDocument3 pagesFWRI Form ReviseJm uniteNo ratings yet
- CIF MALARIA - Rev4 As July 4 2016 - LatestDocument3 pagesCIF MALARIA - Rev4 As July 4 2016 - LatestNicholai Cabaddu100% (2)
- Dr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0Document3 pagesDr. Eutiquio Ll. Atanacio Jr. Memorial Hospital, Inc: DOH-EB-AEHMD-FWRIPIS-2021-0deamhi nursing serviceNo ratings yet
- COVID-19 QuestionnaireDocument2 pagesCOVID-19 QuestionnairePower of Stock Market100% (1)
- English - AFP Investigation Form - Version - 1st - Dec - 2020Document2 pagesEnglish - AFP Investigation Form - Version - 1st - Dec - 2020Tella AdedamolaNo ratings yet
- Pediatric Intake Form SampleDocument10 pagesPediatric Intake Form SampleТравма ЮніверсумNo ratings yet
- Medical Health RecordDocument1 pageMedical Health RecordNikay SerdeñaNo ratings yet
- SBI Recording and Consolidation FormDocument46 pagesSBI Recording and Consolidation FormLee-Ann ZerimarNo ratings yet
- PFIZER 5 17 All in 1 FormDocument3 pagesPFIZER 5 17 All in 1 Formrenz jNo ratings yet
- Malaria Identification and Counseling FormDocument1 pageMalaria Identification and Counseling FormTewodros TafereNo ratings yet
- HPV Template MasterlistDocument1 pageHPV Template Masterlistmarialovella.gonzagaNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Anthrax CifDocument2 pagesAnthrax CifMary Anne Grace GarridoNo ratings yet
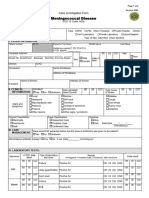
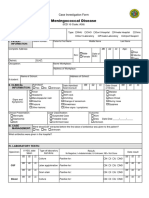
- CIF-Meningococcal DiseaseDocument2 pagesCIF-Meningococcal DiseaseIvy marie BonNo ratings yet
- Fwri Cif FormDocument3 pagesFwri Cif FormMHO GloriaNo ratings yet
- Health FormsDocument9 pagesHealth Formserika luna romanNo ratings yet
- CIF PertussisDocument2 pagesCIF PertussisDan Joseph AguilarNo ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- SBI Recording and Consolidation Form LatestDocument46 pagesSBI Recording and Consolidation Form LatestMannielle MeNo ratings yet
- Case Investigation Form - Meningococcal DiseaseDocument2 pagesCase Investigation Form - Meningococcal Diseaseclaverialc10No ratings yet
- B0146 CashlessDocument1 pageB0146 CashlessSubhajit BhoiNo ratings yet
- Nigeria ART Program Evaluation Data Extraction TooDocument9 pagesNigeria ART Program Evaluation Data Extraction TooALEMAYEHU SHIFERAWNo ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Lindo Gondales Jr.No ratings yet
- Obstetrics History General DataDocument7 pagesObstetrics History General DataColeen NeyraNo ratings yet
- FWRI 2023 CIF v2Document3 pagesFWRI 2023 CIF v2Terence John ChebatNo ratings yet
- James Madison University Immunization FormDocument1 pageJames Madison University Immunization FormMiguel EspirituNo ratings yet
- Revised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)Document3 pagesRevised Case Report Form For Confirmed Novel Coronavirus COVID-19 (Report To WHO Within 48 Hours of Case Identification)テレビスマートNo ratings yet
- Gegm Medical Report Physician FormDocument2 pagesGegm Medical Report Physician FormJohn SlowNo ratings yet
- Vi Virgo Masterlist MeaslesDocument57 pagesVi Virgo Masterlist Measlesbess0910No ratings yet
- CovidreportformDocument1 pageCovidreportformapi-460314063No ratings yet
- Afp 2013Document2 pagesAfp 2013rhu silagoNo ratings yet
- School-Based Immunization Masterlist of Learners GradeDocument9 pagesSchool-Based Immunization Masterlist of Learners GradeRamuel Edrian Tugade PelayoNo ratings yet
- Operation Ugly Truth Nurse Firsthand account of the NYC Pandemic 2020From EverandOperation Ugly Truth Nurse Firsthand account of the NYC Pandemic 2020No ratings yet
- Classroom Management - Wikipedia PDFDocument53 pagesClassroom Management - Wikipedia PDFIbtisam ButtNo ratings yet
- Heliyon: Govind Soni, Ketaki Kale, Saritha Shetty, M.K. Gupta, Khushwant S. YadavDocument10 pagesHeliyon: Govind Soni, Ketaki Kale, Saritha Shetty, M.K. Gupta, Khushwant S. YadavRicardo AndradeNo ratings yet
- Dental Enamel Formation and Implications For Oral Health and DiseaseDocument56 pagesDental Enamel Formation and Implications For Oral Health and DiseaseNonoNo ratings yet
- 3rd Semester Food TechnologyDocument3 pages3rd Semester Food Technologyparthumadineni4No ratings yet
- 2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno TeratozoospermiaDocument12 pages2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno Teratozoospermiakong_666064846No ratings yet
- Rules of Roza (Fasting) in RamadanDocument28 pagesRules of Roza (Fasting) in RamadanDr. Izzat Husain100% (1)
- FFMI and FMI Y. Schutz, 2002Document8 pagesFFMI and FMI Y. Schutz, 2002Mandrake1972No ratings yet
- Test Bank For Nursing Leadership Management and Professional Practice 6th Edition Tamara R DahlkemperDocument24 pagesTest Bank For Nursing Leadership Management and Professional Practice 6th Edition Tamara R DahlkemperDonaldSmithwrmc100% (39)
- Julia Ortiz Luis National High School: Sagaba, Santo DomingoDocument6 pagesJulia Ortiz Luis National High School: Sagaba, Santo DomingoNunag Romel P.No ratings yet
- Jurnal SkripsiDocument9 pagesJurnal SkripsiismihrpNo ratings yet
- Ultimate Ab Burnout Tappbrothers 11Document12 pagesUltimate Ab Burnout Tappbrothers 11Filisha BridgeNo ratings yet
- Le MartDocument4 pagesLe Martbiswasdipankar7025No ratings yet
- Argument Legal SuicideDocument6 pagesArgument Legal SuicideAnda_Ilinca_BooksNo ratings yet
- Clinical Case Asthma WONCA 2019 RevDocument51 pagesClinical Case Asthma WONCA 2019 RevMarvi LashariNo ratings yet
- A School Eye Health Rapid Assessment (SEHRA) Planning Tool: Module To Survey The Magnitude and Nature of Local NeedsDocument9 pagesA School Eye Health Rapid Assessment (SEHRA) Planning Tool: Module To Survey The Magnitude and Nature of Local NeedsOfkom UnhasNo ratings yet
- ProfessionalPractice - FAQ (For BEM's Website) PDFDocument17 pagesProfessionalPractice - FAQ (For BEM's Website) PDFgilbert850507No ratings yet
- Osteoporosis Literature ReviewDocument5 pagesOsteoporosis Literature Reviewafmzinuvouzeny100% (1)
- Handbook On Gender Responsive Police Services enDocument529 pagesHandbook On Gender Responsive Police Services enTim McGuinnessNo ratings yet
- Autism Spectrum DisorderDocument2 pagesAutism Spectrum DisorderMarissa AsimNo ratings yet
- Safety and HealthDocument58 pagesSafety and Healthkhairuddin shamsudinNo ratings yet
- Reviewed Post Training SurveyDocument2 pagesReviewed Post Training SurveyOlawaleAbolarinNo ratings yet
- Quiz 4 Bme4aDocument15 pagesQuiz 4 Bme4aUsman YounasNo ratings yet
- Biological-DeterminismDocument3 pagesBiological-DeterminismRaven SiaNo ratings yet
- I0911thpghs Limpet d6Document2 pagesI0911thpghs Limpet d6Mohammed HamedNo ratings yet
- Wellness Kinesiology: by Wayne W. ToppingDocument15 pagesWellness Kinesiology: by Wayne W. Toppingj.j100% (2)
- Easy Emg A Guide To Performing Nerve Conduction Studies and Electromyography 3Rd Edition Lyn D Weiss Full ChapterDocument52 pagesEasy Emg A Guide To Performing Nerve Conduction Studies and Electromyography 3Rd Edition Lyn D Weiss Full Chapterbenjamin.legg448100% (7)
- Training and Competence Assessment Approved Guideline-Second EditionDocument60 pagesTraining and Competence Assessment Approved Guideline-Second EditionВалерия БедоеваNo ratings yet
- Colorful Organic Child Psychology PresentationDocument15 pagesColorful Organic Child Psychology Presentationلانا ويسNo ratings yet