
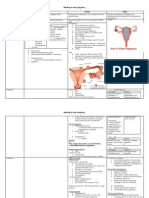
Early First Trimister Bleeding 1
Early First Trimister Bleeding 1
You might also like
- Obgyn UWISE Notes (And Master The Boards)Document8 pagesObgyn UWISE Notes (And Master The Boards)Laura Lopez Roca100% (5)
- Jerome Cauthen V3 PCDocument4 pagesJerome Cauthen V3 PCSammy ChegeNo ratings yet
- OBgyn ShelfDocument10 pagesOBgyn ShelfHassan R. G.100% (1)
- RCOG Green Top Notes 1Document48 pagesRCOG Green Top Notes 1Anonymous LnLvsb100% (1)
- Comparison and Summary of Types of ArthritisDocument2 pagesComparison and Summary of Types of ArthritisShaz Chindhy50% (2)
- Diagnosis of Ectopic PregnancyDocument17 pagesDiagnosis of Ectopic PregnancykushalNo ratings yet
- Early Pregnancy CME Hyrax 2.10Document31 pagesEarly Pregnancy CME Hyrax 2.10Alice KaariaNo ratings yet
- Basics: Abortion, Spontaneous (Miscarriage)Document9 pagesBasics: Abortion, Spontaneous (Miscarriage)Blinkeen WoodsNo ratings yet
- Early Pregnancy CME CBD 14.6Document29 pagesEarly Pregnancy CME CBD 14.6Alice KaariaNo ratings yet
- Obsandgyne Tables 200pagesDocument221 pagesObsandgyne Tables 200pagesRashed ShatnawiNo ratings yet
- Preventive Medicine in Obstetrics Regarding Pregnancy Loss: Dr. Mohammed Abdalla Domiat General HospitalDocument44 pagesPreventive Medicine in Obstetrics Regarding Pregnancy Loss: Dr. Mohammed Abdalla Domiat General HospitalCosmina Alina MoscuNo ratings yet
- Fetal Measures PresentationDocument6 pagesFetal Measures Presentationjeelani saima100% (1)
- RH IsoimmunizationDocument47 pagesRH IsoimmunizationDuncan JacksonNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Obstetrics Summary 1-5Document45 pagesObstetrics Summary 1-5weammshagbaqNo ratings yet
- Preeclampsia-Eclampsia and Chronic HypertensionDocument6 pagesPreeclampsia-Eclampsia and Chronic HypertensionCraikingNo ratings yet
- ObGyn Case FilesDocument27 pagesObGyn Case Filesyanks1120100% (3)
- THROMBOCYTOPENIADocument26 pagesTHROMBOCYTOPENIARokr125No ratings yet
- Abnormal Uterine BleedingDocument22 pagesAbnormal Uterine BleedingAde JuandaNo ratings yet
- Management of PPHDocument24 pagesManagement of PPHMutabazi SharifNo ratings yet
- Management of Pregnancy JaundiceDocument28 pagesManagement of Pregnancy JaundiceShailani Thakur100% (1)
- Ns - Fitrio Deviantony S.Kep Emergency Department Stikes Widyagama HusadaDocument33 pagesNs - Fitrio Deviantony S.Kep Emergency Department Stikes Widyagama HusadadesyNo ratings yet
- OB/GynDocument11 pagesOB/GynAnonymous TYyF7Ul9o100% (2)
- Trauma in OB Bedside Tool Modified ScribdDocument18 pagesTrauma in OB Bedside Tool Modified ScribdmoehowieNo ratings yet
- Thromboembolism & ThromboprophylaxisDocument48 pagesThromboembolism & Thromboprophylaxisazida90No ratings yet
- Early Pregnancy Problems: Presented byDocument28 pagesEarly Pregnancy Problems: Presented byMalk OmryNo ratings yet
- RPL2 ReportDocument66 pagesRPL2 ReportJoseph DavidNo ratings yet
- Hypertension in Pregnancy CompiledDocument67 pagesHypertension in Pregnancy CompiledRaiza Love Caparas-PablicoNo ratings yet
- Amenorrhea Ovarian TumorsDocument18 pagesAmenorrhea Ovarian TumorsJeremy ShimlerNo ratings yet
- By:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDocument26 pagesBy:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDyn AdrianiNo ratings yet
- Pre Eclampsia and Eclampsia: A Review and Recent UpdatesDocument38 pagesPre Eclampsia and Eclampsia: A Review and Recent UpdatesHan OWNo ratings yet
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypatriciaatan1497No ratings yet
- Mother Baby Final Exam ReviewDocument14 pagesMother Baby Final Exam ReviewAngelina mendezNo ratings yet
- Uti in PregnancyDocument42 pagesUti in Pregnancydeepak122No ratings yet
- Thrombo Embolism and PregnancyDocument9 pagesThrombo Embolism and Pregnancysangeetha francisNo ratings yet
- Hypertensive Disorders in PregnancyDocument5 pagesHypertensive Disorders in PregnancyHanya BelajarNo ratings yet
- Hypertensive Disorders of Pregnancy PDFDocument9 pagesHypertensive Disorders of Pregnancy PDFMohammed AbdNo ratings yet
- OB - CPG HTN in Pregnancy BEADocument138 pagesOB - CPG HTN in Pregnancy BEAEllieAdlerNo ratings yet
- OB Intern's Review - Dra LeeDocument214 pagesOB Intern's Review - Dra LeeKathleenZunigaNo ratings yet
- Bleeding in Early PregnancyDocument4 pagesBleeding in Early Pregnancynur1146No ratings yet
- Ectopic PregnancyDocument27 pagesEctopic Pregnancyاحمد احمدNo ratings yet
- Obsetrics and GynaecologyDocument7 pagesObsetrics and GynaecologyAbedinego MalukaNo ratings yet
- Management of Pre - EclampsiaDocument22 pagesManagement of Pre - Eclampsiaapi-3705046No ratings yet
- Hypertensive Disorder in Pregnancy-5-19-2015-ZimbabweDocument39 pagesHypertensive Disorder in Pregnancy-5-19-2015-ZimbabwedanielNo ratings yet
- Anc 1Document128 pagesAnc 1Naila OmerNo ratings yet
- Low-Molecular-Weight Heparin Added To Aspirin in The Prevention of Recurrent Early-Onset Pre-Eclampsia in Women With Inheritable Thrombophilia: The FRUIT-RCTDocument9 pagesLow-Molecular-Weight Heparin Added To Aspirin in The Prevention of Recurrent Early-Onset Pre-Eclampsia in Women With Inheritable Thrombophilia: The FRUIT-RCTNimas Luthfiana HapsariNo ratings yet
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateDocument22 pages1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonNo ratings yet
- CCD Obstetric GynecologyDocument43 pagesCCD Obstetric GynecologyHanif GandohNo ratings yet
- Abortion: DEFINITION-Abortion Is The Separation Partial orDocument77 pagesAbortion: DEFINITION-Abortion Is The Separation Partial orPadmaNo ratings yet
- Nancy E Fay MD Facog Division of Reproductive MedicineDocument32 pagesNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoNo ratings yet
- Narrative Report ContentsDocument15 pagesNarrative Report ContentsGladie Ann Dela RosaNo ratings yet
- B Saranya Sree Balaji Medical College Hospital IndiaDocument33 pagesB Saranya Sree Balaji Medical College Hospital IndiaRosiNo ratings yet
- Antenatal Case - Jonathan Matthews - November 2013Document25 pagesAntenatal Case - Jonathan Matthews - November 2013Anusree AnusreervNo ratings yet
- Bad Obstetric History - Suchitra PanditDocument62 pagesBad Obstetric History - Suchitra PanditameenNo ratings yet
- GYN Module 3 Case 1: Gestational Trophoblastic NeoplasiaDocument21 pagesGYN Module 3 Case 1: Gestational Trophoblastic NeoplasiaElaine Marie Rendon PalmejarNo ratings yet
- Antenatal Assessment of Fetal WellbeingDocument52 pagesAntenatal Assessment of Fetal Wellbeing6ixSideCreate MNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- 2.1 Philippine History of MedicineDocument17 pages2.1 Philippine History of Medicinejessica callNo ratings yet
- FPCS-QI TOR - Guideline - Dr. NizamDocument13 pagesFPCS-QI TOR - Guideline - Dr. NizamSaidur Rahman MilonNo ratings yet
- Archives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisDocument13 pagesArchives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisBHUENDOCRINE SRNo ratings yet
- Janitor Test GuideDocument8 pagesJanitor Test Guidejhae510No ratings yet
- Mapeh: Fourth QuarterDocument6 pagesMapeh: Fourth QuarterWensyl Mae De GuzmanNo ratings yet
- Violence Against Women in The PhilippinesDocument2 pagesViolence Against Women in The PhilippinesJhonavil ReyesNo ratings yet
- Quehanna Boot Camp-2 1Document10 pagesQuehanna Boot Camp-2 1api-508753814No ratings yet
- Community Cares Provider List - Sept 2016Document966 pagesCommunity Cares Provider List - Sept 2016ArizonaBennieNo ratings yet
- Manual Eating Disorders Military PopulationsDocument27 pagesManual Eating Disorders Military PopulationsMonique SousaNo ratings yet
- Nisrin Binti Zaifulsham - Paper CritiqueDocument7 pagesNisrin Binti Zaifulsham - Paper Critiquenisrin zaifulshamNo ratings yet
- Overcoming The Triple Burden of Malnutrition in China: July 2020Document5 pagesOvercoming The Triple Burden of Malnutrition in China: July 2020natasya amabelNo ratings yet
- Edited GANGA Action PlanDocument14 pagesEdited GANGA Action PlanJash ShethiaNo ratings yet
- Lecture 8 (Food Safety and Security)Document35 pagesLecture 8 (Food Safety and Security)Hafiza Emu100% (1)
- Jurnal AzizahDocument6 pagesJurnal AzizahazizahlubisNo ratings yet
- PE MELCs Grade 8Document4 pagesPE MELCs Grade 8Laysa Falsis100% (1)
- Checklist Osce Blok 14Document2 pagesChecklist Osce Blok 14Agung Rizka PratamaNo ratings yet
- Factory Efficiency Comes To The Hospital - The New York TimesDocument7 pagesFactory Efficiency Comes To The Hospital - The New York Timesprasanna020391No ratings yet
- Lung Cancer - NCPDocument2 pagesLung Cancer - NCPChen BernardoNo ratings yet
- Internal Medicine 2 ModuleDocument228 pagesInternal Medicine 2 ModuleØffiçìãl Mãxlìkêr100% (1)
- Handwashing With Soap-Katie G.Document30 pagesHandwashing With Soap-Katie G.YermiNo ratings yet
- Family-Based Treatment of Childhood Anxiety Disorders: Golda S. Ginsburg & Margaret C. SchlossbergDocument12 pagesFamily-Based Treatment of Childhood Anxiety Disorders: Golda S. Ginsburg & Margaret C. Schlossbergthaislane_No ratings yet
- CHAPTER 16 Nursing Informatics and Healthcare PolicyDocument9 pagesCHAPTER 16 Nursing Informatics and Healthcare PolicyAllyssa Leila Estrebillo OrbeNo ratings yet
- Case StudiesDocument3 pagesCase Studiessaranyavijay0% (1)
- GMC Patient - Questionnaire PDF - 48210488Document2 pagesGMC Patient - Questionnaire PDF - 48210488adybutucNo ratings yet
- Sho Exam Workshop - 17 Oct 2021Document60 pagesSho Exam Workshop - 17 Oct 2021hew ka yee100% (2)
- Acute Ischemic Stroke Management: Dr. Aldrin C Leman, SpsDocument25 pagesAcute Ischemic Stroke Management: Dr. Aldrin C Leman, SpsRizky MaulydaNo ratings yet
- While Nurse Susie Was Going To The Hospital, I Studied EnglishDocument6 pagesWhile Nurse Susie Was Going To The Hospital, I Studied EnglishNurul AuliaNo ratings yet
- Week 16Document6 pagesWeek 16Sal MiahNo ratings yet






















































































Download as pdf or txt
You might also like
- Obgyn UWISE Notes (And Master The Boards)Document8 pagesObgyn UWISE Notes (And Master The Boards)Laura Lopez Roca100% (5)
- Jerome Cauthen V3 PCDocument4 pagesJerome Cauthen V3 PCSammy ChegeNo ratings yet
- OBgyn ShelfDocument10 pagesOBgyn ShelfHassan R. G.100% (1)
- RCOG Green Top Notes 1Document48 pagesRCOG Green Top Notes 1Anonymous LnLvsb100% (1)
- Comparison and Summary of Types of ArthritisDocument2 pagesComparison and Summary of Types of ArthritisShaz Chindhy50% (2)
- Diagnosis of Ectopic PregnancyDocument17 pagesDiagnosis of Ectopic PregnancykushalNo ratings yet
- Early Pregnancy CME Hyrax 2.10Document31 pagesEarly Pregnancy CME Hyrax 2.10Alice KaariaNo ratings yet
- Basics: Abortion, Spontaneous (Miscarriage)Document9 pagesBasics: Abortion, Spontaneous (Miscarriage)Blinkeen WoodsNo ratings yet
- Early Pregnancy CME CBD 14.6Document29 pagesEarly Pregnancy CME CBD 14.6Alice KaariaNo ratings yet
- Obsandgyne Tables 200pagesDocument221 pagesObsandgyne Tables 200pagesRashed ShatnawiNo ratings yet
- Preventive Medicine in Obstetrics Regarding Pregnancy Loss: Dr. Mohammed Abdalla Domiat General HospitalDocument44 pagesPreventive Medicine in Obstetrics Regarding Pregnancy Loss: Dr. Mohammed Abdalla Domiat General HospitalCosmina Alina MoscuNo ratings yet
- Fetal Measures PresentationDocument6 pagesFetal Measures Presentationjeelani saima100% (1)
- RH IsoimmunizationDocument47 pagesRH IsoimmunizationDuncan JacksonNo ratings yet
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Obstetrics Summary 1-5Document45 pagesObstetrics Summary 1-5weammshagbaqNo ratings yet
- Preeclampsia-Eclampsia and Chronic HypertensionDocument6 pagesPreeclampsia-Eclampsia and Chronic HypertensionCraikingNo ratings yet
- ObGyn Case FilesDocument27 pagesObGyn Case Filesyanks1120100% (3)
- THROMBOCYTOPENIADocument26 pagesTHROMBOCYTOPENIARokr125No ratings yet
- Abnormal Uterine BleedingDocument22 pagesAbnormal Uterine BleedingAde JuandaNo ratings yet
- Management of PPHDocument24 pagesManagement of PPHMutabazi SharifNo ratings yet
- Management of Pregnancy JaundiceDocument28 pagesManagement of Pregnancy JaundiceShailani Thakur100% (1)
- Ns - Fitrio Deviantony S.Kep Emergency Department Stikes Widyagama HusadaDocument33 pagesNs - Fitrio Deviantony S.Kep Emergency Department Stikes Widyagama HusadadesyNo ratings yet
- OB/GynDocument11 pagesOB/GynAnonymous TYyF7Ul9o100% (2)
- Trauma in OB Bedside Tool Modified ScribdDocument18 pagesTrauma in OB Bedside Tool Modified ScribdmoehowieNo ratings yet
- Thromboembolism & ThromboprophylaxisDocument48 pagesThromboembolism & Thromboprophylaxisazida90No ratings yet
- Early Pregnancy Problems: Presented byDocument28 pagesEarly Pregnancy Problems: Presented byMalk OmryNo ratings yet
- RPL2 ReportDocument66 pagesRPL2 ReportJoseph DavidNo ratings yet
- Hypertension in Pregnancy CompiledDocument67 pagesHypertension in Pregnancy CompiledRaiza Love Caparas-PablicoNo ratings yet
- Amenorrhea Ovarian TumorsDocument18 pagesAmenorrhea Ovarian TumorsJeremy ShimlerNo ratings yet
- By:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDocument26 pagesBy:Dr Herbert Sihite Spog: Divisi Feto Maternal FK Usu /rs HamDyn AdrianiNo ratings yet
- Pre Eclampsia and Eclampsia: A Review and Recent UpdatesDocument38 pagesPre Eclampsia and Eclampsia: A Review and Recent UpdatesHan OWNo ratings yet
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypatriciaatan1497No ratings yet
- Mother Baby Final Exam ReviewDocument14 pagesMother Baby Final Exam ReviewAngelina mendezNo ratings yet
- Uti in PregnancyDocument42 pagesUti in Pregnancydeepak122No ratings yet
- Thrombo Embolism and PregnancyDocument9 pagesThrombo Embolism and Pregnancysangeetha francisNo ratings yet
- Hypertensive Disorders in PregnancyDocument5 pagesHypertensive Disorders in PregnancyHanya BelajarNo ratings yet
- Hypertensive Disorders of Pregnancy PDFDocument9 pagesHypertensive Disorders of Pregnancy PDFMohammed AbdNo ratings yet
- OB - CPG HTN in Pregnancy BEADocument138 pagesOB - CPG HTN in Pregnancy BEAEllieAdlerNo ratings yet
- OB Intern's Review - Dra LeeDocument214 pagesOB Intern's Review - Dra LeeKathleenZunigaNo ratings yet
- Bleeding in Early PregnancyDocument4 pagesBleeding in Early Pregnancynur1146No ratings yet
- Ectopic PregnancyDocument27 pagesEctopic Pregnancyاحمد احمدNo ratings yet
- Obsetrics and GynaecologyDocument7 pagesObsetrics and GynaecologyAbedinego MalukaNo ratings yet
- Management of Pre - EclampsiaDocument22 pagesManagement of Pre - Eclampsiaapi-3705046No ratings yet
- Hypertensive Disorder in Pregnancy-5-19-2015-ZimbabweDocument39 pagesHypertensive Disorder in Pregnancy-5-19-2015-ZimbabwedanielNo ratings yet
- Anc 1Document128 pagesAnc 1Naila OmerNo ratings yet
- Low-Molecular-Weight Heparin Added To Aspirin in The Prevention of Recurrent Early-Onset Pre-Eclampsia in Women With Inheritable Thrombophilia: The FRUIT-RCTDocument9 pagesLow-Molecular-Weight Heparin Added To Aspirin in The Prevention of Recurrent Early-Onset Pre-Eclampsia in Women With Inheritable Thrombophilia: The FRUIT-RCTNimas Luthfiana HapsariNo ratings yet
- 1 - Presentation - Management of Preclamplsia, Mild and ModerateDocument22 pages1 - Presentation - Management of Preclamplsia, Mild and ModeratesharonNo ratings yet
- CCD Obstetric GynecologyDocument43 pagesCCD Obstetric GynecologyHanif GandohNo ratings yet
- Abortion: DEFINITION-Abortion Is The Separation Partial orDocument77 pagesAbortion: DEFINITION-Abortion Is The Separation Partial orPadmaNo ratings yet
- Nancy E Fay MD Facog Division of Reproductive MedicineDocument32 pagesNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoNo ratings yet
- Narrative Report ContentsDocument15 pagesNarrative Report ContentsGladie Ann Dela RosaNo ratings yet
- B Saranya Sree Balaji Medical College Hospital IndiaDocument33 pagesB Saranya Sree Balaji Medical College Hospital IndiaRosiNo ratings yet
- Antenatal Case - Jonathan Matthews - November 2013Document25 pagesAntenatal Case - Jonathan Matthews - November 2013Anusree AnusreervNo ratings yet
- Bad Obstetric History - Suchitra PanditDocument62 pagesBad Obstetric History - Suchitra PanditameenNo ratings yet
- GYN Module 3 Case 1: Gestational Trophoblastic NeoplasiaDocument21 pagesGYN Module 3 Case 1: Gestational Trophoblastic NeoplasiaElaine Marie Rendon PalmejarNo ratings yet
- Antenatal Assessment of Fetal WellbeingDocument52 pagesAntenatal Assessment of Fetal Wellbeing6ixSideCreate MNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- 2.1 Philippine History of MedicineDocument17 pages2.1 Philippine History of Medicinejessica callNo ratings yet
- FPCS-QI TOR - Guideline - Dr. NizamDocument13 pagesFPCS-QI TOR - Guideline - Dr. NizamSaidur Rahman MilonNo ratings yet
- Archives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisDocument13 pagesArchives of Osteoporosis, 2021, 16, 102 - The Indian Society For Bone and Mineral Research (ISBMR) Position Statement For The DiagnosisBHUENDOCRINE SRNo ratings yet
- Janitor Test GuideDocument8 pagesJanitor Test Guidejhae510No ratings yet
- Mapeh: Fourth QuarterDocument6 pagesMapeh: Fourth QuarterWensyl Mae De GuzmanNo ratings yet
- Violence Against Women in The PhilippinesDocument2 pagesViolence Against Women in The PhilippinesJhonavil ReyesNo ratings yet
- Quehanna Boot Camp-2 1Document10 pagesQuehanna Boot Camp-2 1api-508753814No ratings yet
- Community Cares Provider List - Sept 2016Document966 pagesCommunity Cares Provider List - Sept 2016ArizonaBennieNo ratings yet
- Manual Eating Disorders Military PopulationsDocument27 pagesManual Eating Disorders Military PopulationsMonique SousaNo ratings yet
- Nisrin Binti Zaifulsham - Paper CritiqueDocument7 pagesNisrin Binti Zaifulsham - Paper Critiquenisrin zaifulshamNo ratings yet
- Overcoming The Triple Burden of Malnutrition in China: July 2020Document5 pagesOvercoming The Triple Burden of Malnutrition in China: July 2020natasya amabelNo ratings yet
- Edited GANGA Action PlanDocument14 pagesEdited GANGA Action PlanJash ShethiaNo ratings yet
- Lecture 8 (Food Safety and Security)Document35 pagesLecture 8 (Food Safety and Security)Hafiza Emu100% (1)
- Jurnal AzizahDocument6 pagesJurnal AzizahazizahlubisNo ratings yet
- PE MELCs Grade 8Document4 pagesPE MELCs Grade 8Laysa Falsis100% (1)
- Checklist Osce Blok 14Document2 pagesChecklist Osce Blok 14Agung Rizka PratamaNo ratings yet
- Factory Efficiency Comes To The Hospital - The New York TimesDocument7 pagesFactory Efficiency Comes To The Hospital - The New York Timesprasanna020391No ratings yet
- Lung Cancer - NCPDocument2 pagesLung Cancer - NCPChen BernardoNo ratings yet
- Internal Medicine 2 ModuleDocument228 pagesInternal Medicine 2 ModuleØffiçìãl Mãxlìkêr100% (1)
- Handwashing With Soap-Katie G.Document30 pagesHandwashing With Soap-Katie G.YermiNo ratings yet
- Family-Based Treatment of Childhood Anxiety Disorders: Golda S. Ginsburg & Margaret C. SchlossbergDocument12 pagesFamily-Based Treatment of Childhood Anxiety Disorders: Golda S. Ginsburg & Margaret C. Schlossbergthaislane_No ratings yet
- CHAPTER 16 Nursing Informatics and Healthcare PolicyDocument9 pagesCHAPTER 16 Nursing Informatics and Healthcare PolicyAllyssa Leila Estrebillo OrbeNo ratings yet
- Case StudiesDocument3 pagesCase Studiessaranyavijay0% (1)
- GMC Patient - Questionnaire PDF - 48210488Document2 pagesGMC Patient - Questionnaire PDF - 48210488adybutucNo ratings yet
- Sho Exam Workshop - 17 Oct 2021Document60 pagesSho Exam Workshop - 17 Oct 2021hew ka yee100% (2)
- Acute Ischemic Stroke Management: Dr. Aldrin C Leman, SpsDocument25 pagesAcute Ischemic Stroke Management: Dr. Aldrin C Leman, SpsRizky MaulydaNo ratings yet
- While Nurse Susie Was Going To The Hospital, I Studied EnglishDocument6 pagesWhile Nurse Susie Was Going To The Hospital, I Studied EnglishNurul AuliaNo ratings yet
- Week 16Document6 pagesWeek 16Sal MiahNo ratings yet