Download as pdf or txt
You might also like
- Maxillofacial Prosthodontics CourseDocument98 pagesMaxillofacial Prosthodontics CourseFBI LUC1FeR80% (10)
- Anatomy and Physiology 6th Edition Marieb Solutions Manual Full Chapter PDFDocument41 pagesAnatomy and Physiology 6th Edition Marieb Solutions Manual Full Chapter PDFserenafinnodx100% (11)
- Head and Neck: Muscle Charts: Cheat Sheet (English Terminology)Document14 pagesHead and Neck: Muscle Charts: Cheat Sheet (English Terminology)Galo Pillajo100% (1)
- Oral Maxillofacial Surgery Displacement Complications: Gerald Alexander,, Hany AttiaDocument8 pagesOral Maxillofacial Surgery Displacement Complications: Gerald Alexander,, Hany AttiaKamilla MoraisNo ratings yet
- Head and Neck: Muscle Charts: Cheat Sheet (English Terminology)Document14 pagesHead and Neck: Muscle Charts: Cheat Sheet (English Terminology)kaji clappNo ratings yet
- AnaPhy 8-Special SensesDocument67 pagesAnaPhy 8-Special SensesAmielsimon Ngo100% (2)
- Optha Eyelids Orbit Lacrimal DR - Hernando L. Cruz JRDocument11 pagesOptha Eyelids Orbit Lacrimal DR - Hernando L. Cruz JRJack Ortega PuruggananNo ratings yet
- 7 Special SensesDocument99 pages7 Special SensesShaine S. Dimailig0% (1)
- BI 232 Lab 11Document12 pagesBI 232 Lab 11Cj LinceNo ratings yet
- Visual and Lacrimal AppratusDocument45 pagesVisual and Lacrimal AppratusAzman Bin KadirNo ratings yet
- 11 - NS4 Eye Visual System All Sites (Handout) F2022 (Exported)Document43 pages11 - NS4 Eye Visual System All Sites (Handout) F2022 (Exported)Lucky NguyenNo ratings yet
- Orbital Apex Syndrome. A ReviewDocument10 pagesOrbital Apex Syndrome. A ReviewAndrés Faúndez TeránNo ratings yet
- Eye and OrbitDocument2 pagesEye and OrbitCarlo BarriosNo ratings yet
- Anatomi, Fisiologi Mata Serta Overview RZDocument44 pagesAnatomi, Fisiologi Mata Serta Overview RZEuginia Yosephine100% (1)
- Muscle Proximal Attachment (Origin) Distal Attachment (Insertion) Innervation Main Actions Blood Supply Muscle GroupDocument4 pagesMuscle Proximal Attachment (Origin) Distal Attachment (Insertion) Innervation Main Actions Blood Supply Muscle GroupGus LionsNo ratings yet
- Anatomy and Physiology of EyelidDocument19 pagesAnatomy and Physiology of EyelidSonali JainNo ratings yet
- Ophthalmology V Eye Anatomy and FunctionDocument45 pagesOphthalmology V Eye Anatomy and FunctionEndale AschenakiNo ratings yet
- Anatomy and Physiology of EyeDocument44 pagesAnatomy and Physiology of EyetarshaNo ratings yet
- Magic Book 150 Sureshots DR NikitaDocument265 pagesMagic Book 150 Sureshots DR Nikitaprateek varshneyNo ratings yet
- Step 1: Lecture NotesDocument7 pagesStep 1: Lecture NotesHo Hoang VuNo ratings yet
- Upper Ex MusclesDocument18 pagesUpper Ex MusclesKatreena VillarenteNo ratings yet
- The Musculature of The HeadDocument92 pagesThe Musculature of The Headrenzvalorant28No ratings yet
- Efferent Visual System (Ocular Motor Pathways)Document38 pagesEfferent Visual System (Ocular Motor Pathways)riskhapangestika100% (1)
- List of Skeletal Muscles of The Human Body - Wikipedia PDFDocument96 pagesList of Skeletal Muscles of The Human Body - Wikipedia PDFSyed Noor Ul HassanNo ratings yet
- Cranial Nerve ChartDocument1 pageCranial Nerve ChartMarshallMcGoughNo ratings yet
- Anatomy and Physiology of The EyeDocument3 pagesAnatomy and Physiology of The EyecarminaduriasNo ratings yet
- Anatomy and Physiology 2023 2 HourDocument26 pagesAnatomy and Physiology 2023 2 HourPeter MubiNo ratings yet
- Nerve Supply of FaceDocument1 pageNerve Supply of FaceYusri Arif100% (2)
- Scalp Dural Venous Sinus Cavernous Sinus 21 Apr 2024Document8 pagesScalp Dural Venous Sinus Cavernous Sinus 21 Apr 2024kamalarupa180No ratings yet
- Muscles AnatomyDocument14 pagesMuscles AnatomyJiya JithinNo ratings yet
- Cranial NervesDocument4 pagesCranial NervesDenis QosjaNo ratings yet
- The Special Senses: Part A: Prepared by Janice Meeking, Mount Royal CollegeDocument60 pagesThe Special Senses: Part A: Prepared by Janice Meeking, Mount Royal CollegeRaul ReynosoNo ratings yet
- Anatomy Cranial NervesDocument3 pagesAnatomy Cranial NervesMedShare100% (1)
- Anatomy and Physiology 6th Edition Marieb Solutions ManualDocument20 pagesAnatomy and Physiology 6th Edition Marieb Solutions Manualstephenthanh1huo100% (31)
- Marrow ErrataDocument268 pagesMarrow ErrataDr.Ebenesar DhasarathanNo ratings yet
- Rongga ObitaDocument27 pagesRongga ObitaFadli LatamaNo ratings yet
- Methodic Materials MovementDocument20 pagesMethodic Materials MovementKapil PancholiNo ratings yet
- Cranial NervesDocument17 pagesCranial Nervesdankirsh100% (17)
- Anatomy MRDocument40 pagesAnatomy MRYayu INDONESIANo ratings yet
- L 01 Ocular AnatomyDocument13 pagesL 01 Ocular Anatomydoni anandaNo ratings yet
- Regional Anesthesiaposter UpperandlowerextremityDocument4 pagesRegional Anesthesiaposter UpperandlowerextremityNS Biomendical Equipments service pvt ltdNo ratings yet
- Regional Anesthesiaposter Upperandlowerextremity PrintDocument4 pagesRegional Anesthesiaposter Upperandlowerextremity PrintAhmedNo ratings yet
- Anatomi MATADocument40 pagesAnatomi MATAadil sipahutarNo ratings yet
- 1 Anatomy & Physiology of Eye For Ophthalmic NursesDocument124 pages1 Anatomy & Physiology of Eye For Ophthalmic NursesSMEY204100% (1)
- Work Sheet 7 The Muscular System A28 Group1Document5 pagesWork Sheet 7 The Muscular System A28 Group1Japet Floyd AlipioNo ratings yet
- Abducens Nerve - Cranial Nerve VI AtfDocument4 pagesAbducens Nerve - Cranial Nerve VI AtfCathy SolivarNo ratings yet
- Anestesia - Handbook of Regional Anesthesia - ESRA 2007Document130 pagesAnestesia - Handbook of Regional Anesthesia - ESRA 2007Irene Cristina100% (3)
- Cranial Nerve III - Oculomotor Nerve - FRCEM SuccessDocument1 pageCranial Nerve III - Oculomotor Nerve - FRCEM SuccessJohn CoxNo ratings yet
- Lab 2 - Answers MSDocument8 pagesLab 2 - Answers MSMikeNo ratings yet
- Evaluation of Ocular Surface Disease in Asian Patients With PrimaryDocument11 pagesEvaluation of Ocular Surface Disease in Asian Patients With PrimaryPriscaNo ratings yet
- Cranial Nerves Atlas Part 2Document26 pagesCranial Nerves Atlas Part 2Катерина ЛяшинаNo ratings yet
- ANATOMY Lec 4 Face Dr. SingcoDocument5 pagesANATOMY Lec 4 Face Dr. SingcoMarc Lyndon CafinoNo ratings yet
- Eye Model LabeledDocument12 pagesEye Model LabeledGrecia Vazquez SegoviaNo ratings yet
- Cranial Nerves: Romulo U. EsagundeDocument72 pagesCranial Nerves: Romulo U. EsagundeLoisen Nathan DanielNo ratings yet
- Anatomy of The Image-Forming EyeDocument23 pagesAnatomy of The Image-Forming EyekupukupuNo ratings yet
- Myofascial Meridians As Anatomical Evidence of AcuDocument9 pagesMyofascial Meridians As Anatomical Evidence of AcuTo MNo ratings yet
- BMS 3 EyeDocument18 pagesBMS 3 Eye058 Rayhan Alkumanonu AmrizalNo ratings yet
- Learn To Draw Animals PDFDocument58 pagesLearn To Draw Animals PDFArindam Chakma75% (4)
- Anatomyofnoseandparanasalsinus 100616084243 Phpapp02Document33 pagesAnatomyofnoseandparanasalsinus 100616084243 Phpapp02Igor Quarmina HesseNo ratings yet
- Multiple Choice Questions: A. B. C. DDocument37 pagesMultiple Choice Questions: A. B. C. DwanderagroNo ratings yet
- (9-2) THT - KL Anatomi 2020Document88 pages(9-2) THT - KL Anatomi 2020ayurhrdiniNo ratings yet
- Opthalmology NotesDocument43 pagesOpthalmology NotesKashif Khan100% (2)
- Questions ComaDocument2 pagesQuestions ComaFlowerNo ratings yet
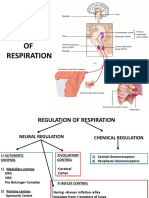
- Neural Regulation of RespirationDocument22 pagesNeural Regulation of RespirationDhanush SatheeshNo ratings yet
- The Somatic Nervous System The Autonomic Nervous System - The Enteric Nervous SystemDocument5 pagesThe Somatic Nervous System The Autonomic Nervous System - The Enteric Nervous SystemMarissa AsimNo ratings yet
- Neurology 4-Years MCQsDocument5 pagesNeurology 4-Years MCQsPlutonic HeartNo ratings yet
- Viva NotesDocument210 pagesViva NotesIsaac Tan Yieng LerNo ratings yet
- NCM IO3 Eye ExaminationDocument50 pagesNCM IO3 Eye ExaminationNicole NipasNo ratings yet
- Root of The Neck (Gross)Document21 pagesRoot of The Neck (Gross)Kimsha ConcepcionNo ratings yet
- Gambaran Kebiasaan Buruk Dan Kejadian Maloklusi Pada Siswa Sekolah Dasar Negeri 19 PemecutanDocument5 pagesGambaran Kebiasaan Buruk Dan Kejadian Maloklusi Pada Siswa Sekolah Dasar Negeri 19 PemecutanRega RegiawanNo ratings yet
- Facial MusclesDocument16 pagesFacial Musclesmonica saddadiNo ratings yet
- Fascial Space InfectionsDocument15 pagesFascial Space Infectionsali tiwanaNo ratings yet
- Anatomy & Physiology of Lacrimal Secretion & Outflow: Presented by DR Rohit RaoDocument60 pagesAnatomy & Physiology of Lacrimal Secretion & Outflow: Presented by DR Rohit RaoHenok BirukNo ratings yet
- 4 9 Myfriend 1Document2 pages4 9 Myfriend 1OmarNo ratings yet
- CT PNSDocument22 pagesCT PNSHany85No ratings yet
- Self Study Intraoral Anatomy RadiologyDocument80 pagesSelf Study Intraoral Anatomy RadiologydeenmNo ratings yet
- Mandibular Movements FDocument37 pagesMandibular Movements Fhamidjigar100% (1)
- AIC CatalogueDocument18 pagesAIC CatalogueshuNo ratings yet
- Anatomy and Pathology of The Cerebellar PeduncleDocument9 pagesAnatomy and Pathology of The Cerebellar PeduncleJulius Dominique L. AnjaoNo ratings yet
- Anatomy and Physiology of LarynxDocument13 pagesAnatomy and Physiology of LarynxAmin MasromNo ratings yet
- Deep Neck Infection1deep Neck Space InfectionDocument53 pagesDeep Neck Infection1deep Neck Space Infectionwhitelotusoo7No ratings yet
- Panfacial FracturesDocument35 pagesPanfacial FracturesMARISOL GALLEGO DUQUENo ratings yet
- Anatomy and Physiology of The EarDocument46 pagesAnatomy and Physiology of The EarRoni Ananda Perwira HarahapNo ratings yet
- Fiber Dissection Technique: Lateral Aspect of The Brain: Surgical Anatomy and TechniqueDocument11 pagesFiber Dissection Technique: Lateral Aspect of The Brain: Surgical Anatomy and TechniqueRafaelNo ratings yet
- Cerebral Dominance (Auditory Perception)Document7 pagesCerebral Dominance (Auditory Perception)shruthipeeyemNo ratings yet