Download as pdf or txt
You might also like
- Effects of Social Media On Mental Health: A Case StudyDocument12 pagesEffects of Social Media On Mental Health: A Case StudyTialena Evans100% (1)
- CDC Covering The Basics Rhetorical Analysis EssayDocument4 pagesCDC Covering The Basics Rhetorical Analysis EssayAllechia JonesNo ratings yet
- Social Media in HealthcareDocument9 pagesSocial Media in HealthcareTibi SátorNo ratings yet
- Preventing Chronic Disease: Social Media Use Among Parents and Women of Childbearing Age in The USDocument5 pagesPreventing Chronic Disease: Social Media Use Among Parents and Women of Childbearing Age in The USİpek DemirbeyNo ratings yet
- Jurnal EducationDocument7 pagesJurnal EducationriyadhNo ratings yet
- Social Media's Role in Health CareDocument8 pagesSocial Media's Role in Health CareAmit ChoudharyNo ratings yet
- Parental Use of Social MediaDocument11 pagesParental Use of Social Mediahicham lekfifiNo ratings yet
- The Impact of Social Media On Young People's Health and Wellbeing: Evidence, Guidelines and Actions.Document27 pagesThe Impact of Social Media On Young People's Health and Wellbeing: Evidence, Guidelines and Actions.Jagdish Singh Sohal100% (1)
- Kiy 1Document15 pagesKiy 1MAGOMU DAN DAVIDNo ratings yet
- 1 s2.0 S1386505617301636 MainDocument12 pages1 s2.0 S1386505617301636 MainNoor JaafarNo ratings yet
- Research Chapter 1 Abm A Group 3Document9 pagesResearch Chapter 1 Abm A Group 3Kc RondaNo ratings yet
- The Ubiquitous Social Media Landscape: Gaps in Understanding The Effect of Health MisinformationDocument4 pagesThe Ubiquitous Social Media Landscape: Gaps in Understanding The Effect of Health MisinformationSintia KristianiNo ratings yet
- Health Literacy Among Older Adults A Systematic Literature ReviewDocument4 pagesHealth Literacy Among Older Adults A Systematic Literature ReviewcmaqqsrifNo ratings yet
- Evaluation of Acceptance and Adoption of Health-Care Information On Twitter by University StudentsDocument51 pagesEvaluation of Acceptance and Adoption of Health-Care Information On Twitter by University StudentsDaniel ObasiNo ratings yet
- Research Article: Association Between Social Media Use and Depression Among U.S. Young AdultsDocument9 pagesResearch Article: Association Between Social Media Use and Depression Among U.S. Young AdultsAisyah IzzatiNo ratings yet
- Facebook As A Platform For Health Information and Communication: A Case Study of A Diabetes GroupDocument12 pagesFacebook As A Platform For Health Information and Communication: A Case Study of A Diabetes GroupDragos IordacheNo ratings yet
- Kim 2015Document10 pagesKim 2015cekNo ratings yet
- Health Information-Seeking Behaviors, Health Indicators, and Health RisksDocument6 pagesHealth Information-Seeking Behaviors, Health Indicators, and Health RisksC. R. PintoNo ratings yet
- SelfDocument10 pagesSelfZaid MarwanNo ratings yet
- We're Still acc-WPS OfficeDocument8 pagesWe're Still acc-WPS OfficeGeorge TwambaNo ratings yet
- 2023 - Influence of Social Media Uses and GratificationsDocument12 pages2023 - Influence of Social Media Uses and Gratificationsyuliia.catraisNo ratings yet
- Harnessing Social Media For HealthDocument10 pagesHarnessing Social Media For HealthMona HelouNo ratings yet
- Chapter 1 Mariam1Document6 pagesChapter 1 Mariam1oluwasegunnathaniel0No ratings yet
- Anna Bohigians Hot Topic Presentation 1-11Document9 pagesAnna Bohigians Hot Topic Presentation 1-11api-547181616No ratings yet
- Research 2Document16 pagesResearch 2Steph VistalNo ratings yet
- BODY RESEARCH 3 Copy - EditedDocument78 pagesBODY RESEARCH 3 Copy - EditedG09. Ditan, Zyann Kris B.No ratings yet
- Harnessing Social Media For Behavioural ChangeDocument10 pagesHarnessing Social Media For Behavioural ChangeAbril Herrera100% (1)
- Distributed Health Literacy in The Maternal Health Context in VietnamDocument12 pagesDistributed Health Literacy in The Maternal Health Context in Vietnamhairun hairunNo ratings yet
- MapehresearchDocument12 pagesMapehresearchShane CarambacanNo ratings yet
- Inquiry ProjectDocument3 pagesInquiry Projectapi-361876616No ratings yet
- Presentation 10Document7 pagesPresentation 10Jose hade valeza ReyesNo ratings yet
- How Does The Circulation of Misinformation Create A Massive Public Health IssueDocument2 pagesHow Does The Circulation of Misinformation Create A Massive Public Health IssueKenneth Roy MatuguinaNo ratings yet
- ArticleDocument19 pagesArticleKITTIVONGSAK VONGSUTHEP KEITHNo ratings yet
- Outline Defense-1Document5 pagesOutline Defense-1Gogs Ediza AlejoNo ratings yet
- Critical Reading: Pair Reading Project - Term 3Document3 pagesCritical Reading: Pair Reading Project - Term 3Nhật LệNo ratings yet
- Current Challenge in Consumer Health Informatics PDFDocument10 pagesCurrent Challenge in Consumer Health Informatics PDFAyres EvangNo ratings yet
- TransgenderadolescentsDocument6 pagesTransgenderadolescentsFio ChNo ratings yet
- Utiliting Social Medias As A Health Promotion Tools To Engage Millennials: A Systematic ReviewDocument2 pagesUtiliting Social Medias As A Health Promotion Tools To Engage Millennials: A Systematic ReviewaishaysNo ratings yet
- FWD Mariel Sunderland Contemporary Challenges in Health and Social CareDocument13 pagesFWD Mariel Sunderland Contemporary Challenges in Health and Social Carehoodyfoody09No ratings yet
- Dietary Supplement Users Vary in Attitudes and Sources of Dietary Supplement Information in East and West Geographic Regions: A Cross-Sectional StudyDocument10 pagesDietary Supplement Users Vary in Attitudes and Sources of Dietary Supplement Information in East and West Geographic Regions: A Cross-Sectional StudyfsfNo ratings yet
- Physicians, Patients, and Facebook: Could You? Would You? Should You?Document16 pagesPhysicians, Patients, and Facebook: Could You? Would You? Should You?Oscar Iván Negrete RodríguezNo ratings yet
- Inflammatory Bowel Disease Patient Leaders' Responsibility For Disseminating Health Information OnlineDocument12 pagesInflammatory Bowel Disease Patient Leaders' Responsibility For Disseminating Health Information OnlinebthoehNo ratings yet
- Exploring The Use of Social Networking Platforms As A Tool For Disseminating Information On World Health Day 2023Document6 pagesExploring The Use of Social Networking Platforms As A Tool For Disseminating Information On World Health Day 2023International Journal of Innovative Science and Research TechnologyNo ratings yet
- Strengthening Health Information Systems To Address Health Equity ChallengesDocument16 pagesStrengthening Health Information Systems To Address Health Equity ChallengesAhlidin S.No ratings yet
- Lideta Catholic Cathedral SchoolDocument2 pagesLideta Catholic Cathedral SchoolmarkohabtamuNo ratings yet
- Social Media: How Hospitals Use It, and Opportunities For Future UseDocument14 pagesSocial Media: How Hospitals Use It, and Opportunities For Future UseFaizaNadeemNo ratings yet
- Presentation 1Document11 pagesPresentation 1musman00880No ratings yet
- Response & ReflectionDocument2 pagesResponse & ReflectioncintiabarokahNo ratings yet
- SOP, Hypothesis, RRLDocument7 pagesSOP, Hypothesis, RRLHavier EsparagueraNo ratings yet
- Day 056Document11 pagesDay 056Angelia Reza DevantyNo ratings yet
- Jurnal Internasional - Angelia Reza D - 6411420035Document11 pagesJurnal Internasional - Angelia Reza D - 6411420035Angelia Reza DevantyNo ratings yet
- Annotated Bibliograph1Document6 pagesAnnotated Bibliograph1bertchen123No ratings yet
- Lstewart Community Health Project 201730 Summernurs492 32489Document14 pagesLstewart Community Health Project 201730 Summernurs492 32489api-466983597No ratings yet
- Komunikasi KesehatanDocument14 pagesKomunikasi Kesehatanprita erlanggaNo ratings yet
- Zhang Et Al 2017Document15 pagesZhang Et Al 2017Mahmoud Abdelfatah MahgoubNo ratings yet
- Essay 3 Final Eng1302Document6 pagesEssay 3 Final Eng1302api-708111083No ratings yet
- Social Science & Medicine: Sian K. Smith, Ann Dixon, Lyndal Trevena, Don Nutbeam, Kirsten J. MccafferyDocument8 pagesSocial Science & Medicine: Sian K. Smith, Ann Dixon, Lyndal Trevena, Don Nutbeam, Kirsten J. MccafferySteven WoodheadNo ratings yet
- Sidani Et Al, 2016Document16 pagesSidani Et Al, 2016DeepaNo ratings yet
- The Role of Social Media Among College StudentsDocument3 pagesThe Role of Social Media Among College StudentsTherese Melchie SantuyoNo ratings yet
- PHY 462-Atomic PhysicsDocument3 pagesPHY 462-Atomic PhysicsAnil karela100% (1)
- WebpdfDocument272 pagesWebpdfMariangela Petrizzo PáezNo ratings yet
- Rotenberg, The Metropolis and Everyday LifeDocument9 pagesRotenberg, The Metropolis and Everyday LifeAngie Tatiana Camelo BautistaNo ratings yet
- Activity 2 Grammar TaskDocument11 pagesActivity 2 Grammar TaskAnnalisa ChenNo ratings yet
- Marketing Research: Ninth EditionDocument44 pagesMarketing Research: Ninth EditionSara DassouliNo ratings yet
- Why Is Field Trip A Learning Experience That Is Highly Recommendable For Children?Document3 pagesWhy Is Field Trip A Learning Experience That Is Highly Recommendable For Children?Bab SitaNo ratings yet
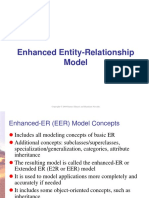
- DBMS - Part 2 - Enhanced Entity Relationship ModelDocument21 pagesDBMS - Part 2 - Enhanced Entity Relationship ModelINN ChannelNo ratings yet
- Okeefe Courtney Self-Care Final Eval Spring 2022Document7 pagesOkeefe Courtney Self-Care Final Eval Spring 2022api-606420000No ratings yet
- Modes of Protest in Ngugi's A Grain of Wheat: AbstractDocument10 pagesModes of Protest in Ngugi's A Grain of Wheat: AbstractAuron AthanasNo ratings yet
- THE2300 Tartuffe AnalysisDocument2 pagesTHE2300 Tartuffe AnalysisVladShukrutaNo ratings yet
- Licodaine (Drug Study)Document4 pagesLicodaine (Drug Study)2BSN19Manuel, Rhadalie V.No ratings yet
- We'Ve Always Been Distracted, or at Least Worried That We Are Aeon EssaysDocument10 pagesWe'Ve Always Been Distracted, or at Least Worried That We Are Aeon EssaysJeffery TaylorNo ratings yet
- Digital Signal Processor Based Vbyf Control of Speed of Induction MotorDocument24 pagesDigital Signal Processor Based Vbyf Control of Speed of Induction MotorManu JainNo ratings yet
- Prevod: Treacherous, I Didn't Ever Believe You'd Put Yourself Into This Sort of Squalid MuddleDocument17 pagesPrevod: Treacherous, I Didn't Ever Believe You'd Put Yourself Into This Sort of Squalid MuddleMarina TanovićNo ratings yet
- Meridian SystemDocument34 pagesMeridian SystemYaqueli Mayta100% (2)
- Website AndalanDocument9 pagesWebsite AndalanRIZKI PUTRA PRATAMANo ratings yet
- Repaso Bachillerato - EjerciciosDocument5 pagesRepaso Bachillerato - EjerciciosAnonymous qmwoKAfNo ratings yet
- Lecture 6: The Greeks and Basic Hedging: Sources Avellaneda and Laurence J HullDocument20 pagesLecture 6: The Greeks and Basic Hedging: Sources Avellaneda and Laurence J HullJNo ratings yet
- To Daffodils Robert Herrick Literary AnaDocument5 pagesTo Daffodils Robert Herrick Literary AnaMoustafa AbdullahNo ratings yet
- Cs Poster Project RubricDocument1 pageCs Poster Project Rubricapi-485771211No ratings yet
- Curses and Smoke: A Novel of Pompeii by Vicky Alvear Shecter (Excerpt)Document25 pagesCurses and Smoke: A Novel of Pompeii by Vicky Alvear Shecter (Excerpt)I Read YANo ratings yet
- Toji Fushiguro Jujutsu Kaisen Wiki FandomDocument1 pageToji Fushiguro Jujutsu Kaisen Wiki Fandomcadenglenn1023No ratings yet
- Tutorial 3: - LGSI Zee in Bending: Z 12 X 2.5 14g, F 50ksi - ObjectiveDocument11 pagesTutorial 3: - LGSI Zee in Bending: Z 12 X 2.5 14g, F 50ksi - ObjectivekhayatNo ratings yet
- In Praise of Creation - LessonDocument9 pagesIn Praise of Creation - LessonMuzic WuzicNo ratings yet
- Lee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Document181 pagesLee - Chinese People's Diplomacy and Developmental Relations With East Asia - Trends in The Xi Jinping Era-Routledge (2020)Ralph Romulus FrondozaNo ratings yet
- Guru Vachaka Kovai - Sri Muruganar - Trans. Sri SadDocument405 pagesGuru Vachaka Kovai - Sri Muruganar - Trans. Sri Sadappamana5576No ratings yet
- Assignment 2 - Employment and CPI PDFDocument3 pagesAssignment 2 - Employment and CPI PDFscarlet dangNo ratings yet
- Arrived at School: Go To The Bathroom and Take A BathDocument1 pageArrived at School: Go To The Bathroom and Take A Bathmarriette joy abadNo ratings yet
- The Great Red GanapatiDocument4 pagesThe Great Red GanapatiJust JoolzNo ratings yet
- Human Values and Contemporary IssuesDocument11 pagesHuman Values and Contemporary IssuesGajanan Shirke AuthorNo ratings yet