Professional Documents
Culture Documents
Immune Mediated Myelopathies.11
Immune Mediated Myelopathies.11
Uploaded by
Mayra AldecoaOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Immune Mediated Myelopathies.11
Immune Mediated Myelopathies.11
Uploaded by
Mayra AldecoaCopyright:
Available Formats
REVIEW ARTICLE
Immune-Mediated
C O N T I N UU M A UD I O
I NT E R V I E W A V AI L A B L E
ONLINE
Myelopathies
By Michael Levy, MD, PhD, FAAN
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
ABSTRACT
OBJECTIVE: Immune-mediated myelopathies are conditions in which the
CITE AS:
CONTINUUM (MINNEAP MINN) immune system attacks the spinal cord. This article describes the
2024;30(1, SPINAL CORD distinguishing characteristics of immune-mediated myelopathies and
DISORDERS):180–198.
treatment strategies for patients affected by these disorders.
Address correspondence to
Dr Michael Levy, 65 LATEST DEVELOPMENTS:New biomarkers, such as aquaporin 4 and myelin
Landsdowne St, Lab 500,
Cambridge, MA 02139,
oligodendrocyte glycoprotein antibodies, in the blood and spinal fluid
MLEVY11@mgh.harvard.edu. have led to the identification of antigen-specific immune-mediated
myelopathies and approved therapies to prevent disease progression.
RELATIONSHIP DISCLOSURE:
Dr Levy has received personal
compensation in the range of ESSENTIAL POINTS: Thefirst step in the diagnosis of an immune-mediated
$500 to $4999 for serving as a myelopathy is confirming that the immune system is the cause of the attack
consultant for Mitsubishi
Tanabe Pharma America, Inc, by excluding non–immune-mediated causes. The second step is to narrow
and UCB, Inc, and as an editor, the differential diagnosis based on objective biomarkers such as serology
associate editor, or editorial
and MRI patterns. The third step is to treat the specific immune-mediated
advisory board member for
Elsevier; in the range of $5000 to myelopathy by using evidence-based medicine.
$9999 for serving as a
consultant for Sanofi and
serving on scientific advisory or
data safety monitoring boards INTRODUCTION
for Alexion Pharmaceuticals, Inc,
Genentech, Inc, and Horizon Immune-mediated myelopathies are conditions in which spinal cord dysfunction
Therapeutics plc; and in the results from damage caused by the immune system. The scope of this article is
range of $10,000 to $49,999 for limited to immune-mediated conditions outside of the context of an infection,
serving as an expert witness for
various law firms. The institution including multiple sclerosis (MS), antigen-specific autoimmune diseases,
of Dr Levy has received inflammatory myelitis, neurosarcoidosis, and paraneoplastic diseases. Infections
research support from the
National Institutes of Health (R01
in the spinal cord and the damage that occurs as a result of the infection plus
AI153068). the immune response are included in the article “Infectious Myelopathies” by
Anita M. Fletcher, MD, and Shamik Bhattacharyya, MD, FAAN,1 in this issue
UNLABELED USE OF
PRODUCTS/INVESTIGATIONAL
of Continuum. Immune-mediated myelopathies are often included in the
USE DISCLOSURE: differential diagnosis of other disorders of the spinal cord, particularly those
Dr Levy discusses the use of included in the article “Vascular Myelopathies” by Ashutosh P. Jadhav, MD,
azathioprine, corticosteroids,
cyclophosphamide, infliximab, PhD, FAAN,2 and a detailed algorithm for diagnosing spinal cord disorders can
intravenous immunoglobulins be found in the article “Clinical Approach to Myelopathy Diagnosis” by Carlos A.
(IVIg), mycophenolate mofetil,
Pardo, MD,3 both of which can also be found in this issue of Continuum. CASE 8-1
and rituximab, none of which
are approved by the US Food is an example of a typical case of an immune-mediated myelopathy.
and Drug Administration for the
treatment of immune-mediated
myelopathies. GENERAL PRINCIPLES OF IMMUNE-MEDIATED MYELOPATHIES
The immune system can lead to nervous system dysfunction in two ways. First,
© 2024 American Academy the inflammatory process can disrupt the function of white matter tracts and
of Neurology. neuronal activity. Even when the tracts remain anatomically intact and
180 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
myelinated, saltatory conduction may be impaired because of changes in the
surrounding electrolyte balance, and synaptic transmission may be disrupted by
cytokines and antibodies. Second, inflammation can cause anatomic damage in
the spinal cord, ranging from demyelination to necrosis. In the first mechanism,
reversal of inflammation typically leads to rapid recovery of function whereas
when anatomic damage occurs recovery is delayed by a longer remyelinating
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
process.4
The immune-mediated myelopathies discussed in the article share many
features and can be difficult to distinguish without a thorough workup. In many
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
cases, the diagnosis is easier to make in retrospect because clues emerge from
both the acute attack and the recovery period. Clinical equipoise and empiric
treatment based on clinical judgment are common principles in the workup and
treatment of immune-mediated myelopathies in the real world.
A 46-year-old woman from Haiti with a history of Sjögren syndrome CASE 8-1
presented to the emergency department with sudden neck pain,
followed by arm and leg weakness over 24 hours. While in the emergency
department, she developed urinary retention requiring catheterization.
Her Sjögren syndrome history included dry eyes and a previous episode
of vision loss in her right eye that was ascribed to Sjögren optic neuritis.
She had been using hydroxychloroquine and occasionally corticosteroids
for flares of her Sjögren syndrome.
Her physical examination revealed a normal mental status. Her cranial
nerves were intact except for 20/200 visual acuity covering most of her
visual field in her right eye. She had 3/5 strength in her arms and 2/5
strength from her hips to her toes in both legs. Reflexes were reduced in
her arms, absent in her legs, and mute in her toes. Sensation was
markedly reduced to light touch in her legs with a sensory level at C5. She
was unable to ambulate.
MRI of her spinal cord showed a longitudinally extensive lesion from C1
to C5 with avid contrast enhancement at C2 and C3. Serologies were sent
for antinuclear antibodies (she was previously positive for Sjögren
syndrome antigens A and B), anti–aquaporin 4 (AQP4) antibodies,
anti–myelin oligodendrocyte glycoprotein (MOG) antibodies, and
anticardiolipin antibodies. Spinal fluid identified the presence of 120
white blood cells/mm3, 99% of which were lymphocytes, mildly elevated
protein and glucose, and negative Gram stain for bacteria.
This case highlights a typical presentation of an immune-mediated COMMENT
myelopathy. Evidence of inflammation in the spinal cord was confirmed by
both spinal fluid analysis and MRI. While awaiting serology results, she was
appropriately started on treatment with high-dose corticosteroids. After
her AQP4 antibody returned positive, she was diagnosed with
neuromyelitis optica spectrum disorder and escalated to therapy with
plasma exchange.
CONTINUUMJOURNAL.COM 181
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
COMMON FEATURES OF IMMUNE-MEDIATED MYELOPATHIES
The clues that neurologists rely on in the workup of immune-mediated
myelopathies are broadly categorized into a history of present illness, including
the time course, CSF analysis, MRI, and serology. Although spinal fluid analysis is
not always readily available, MRI with contrast and serology are vital parts of the
workup for immune-mediated myelopathy and should always be included in the
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
workup if possible.
When the immune system causes spinal cord inflammation, it can be acute and
severe, such as the attacks associated with neuromyelitis optica spectrum disorder
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
(NMOSD). These attacks can progress rapidly to a nadir of complete paralysis
within a few hours. More commonly, immune-mediated attacks of the spinal cord
tend to occur over hours to days. In 2002, the Transverse Myelitis Consortium
Working Group5 defined the time course of idiopathic inflammatory myelitis as at
least 4 hours but not more than 21 days to nadir. The 4-hour time minimum is
intended to exclude vascular myelopathies, which can take minutes in arterial
strokes to hours for venous strokes. The 21-day limit was intended to distinguish
subacute and chronic conditions such as arteriovenous malformations, which can
evolve over months. Paraneoplastic diseases also typically present in a subacute to
chronic time course. The time from onset to nadir is included as a major clue in
each section below to help organize the differential diagnoses.
Other important features of immune-mediated myelopathies that should be
captured in the history of present illness are immune triggers, co-occurring
autoimmunity or cancer, and family history. Triggers commonly include infections
and vaccines. These triggers are not yet known to be specific to a particular vaccine
or infection or a particular central nervous system (CNS) antigen. In contrast,
molecular mimicry has been shown to be the mechanism responsible for acute
peripheral nerve demyelination in Guillain Barre syndrome following infection with
Campylobacter, for example.6 Thus, there may be an element of molecular mimicry
to many different antigens that all lead to a common downstream clinical
presentation of myelopathy. Another explanation is that the immune triggers may
be nonspecific stimulants to a broader immune response whereby the rogue element
that attacks the spinal cord is given a boost sufficient to induce a clinical attack. This
latter explanation is supported by the wide number of immune triggers that have
been associated with immune-mediated myelopathies.7
Co-occurring autoimmunity is a clue that a patient may be predisposed to an
immune-mediated myelopathy. A good example is a patient with known
systemic lupus erythematosus who presents with an acute myelopathic
syndrome. Systemic lupus erythematosus has significant overlap with NMOSD,
and patients with this disorder commonly test positive after a transverse myelitis
attack for the aquaporin 4 (AQP4) antibody associated with NMOSD.8,9 Sjögren
syndrome is also tied to NMOSD and inflammatory myelitis.10,11 A history of N-
methyl-D-aspartate (NMDA) receptor encephalitis is associated with a higher
risk of NMOSD and myelin oligodendrocyte glycoprotein (MOG) antibody
disease.12 Sarcoidosis in the lungs is strongly linked to neurosarcoidosis in the
brain and spinal cord.13 Even without a link, co-occurring autoimmunity raises
the level of suspicion that a myelopathy may be autoimmune. Similarly, a known
history of cancer, especially small cell lung cancer, breast cancer, and thymomas,
should prompt consideration of paraneoplastic conditions.14
Family history may be useful in specific scenarios. MS has more than 200
known genetic factors.15 If one identical twin has MS, the other twin has an
182 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
approximately 30% risk of also developing the same disorder.16 Mothers with KEY POINT
MS transmit an approximately 5% risk of developing MS to their children, and
● The four major clues in
fathers pass down an approximately 3% risk.17 MS presents with a myelitis the diagnosis of
attack in approximately 62% to 80% of cases; 80% of people with MS have a visible immune-mediated
lesion in their spinal cord at diagnosis.18,19 In 2018, a familial form of idiopathic myelopathies are the time
inflammatory myelitis was described as related to variants in the family of genes course of disease, spinal
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
fluid analysis, MRI features,
that control vesicle and exosome handling.20 There are a few patient families with
and serology.
NMOSD21 but as yet no reports of hereditary MOG antibody disease.
The blood-brain barrier (and blood-spine barrier) maintains an
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
immune-privileged zone in the CNS. Typically, only select immune cells are
permitted to traffic in and out; these include monocytes and T cells. No more
than 5 white blood cells/mm3 of CSF is expected in healthy lumbar puncture
samples. More than 5 white blood cells/mm3 indicates that a pathologic process is
occurring or has recently occurred. In some nonimmune myelopathies, including
trauma and vascular myelopathy, a mild pleocytosis (>5 white blood cells/mm3)
has been observed.22-24 Myelopathies with more than 100 white blood cells/mm3
must be considered to have an immune-mediated or infectious etiology until
proven otherwise.25 Immune cell counts and other CSF characteristics are useful
clues in distinguishing among the causes of immune-mediated myelopathies
described in more detail in the individual sections that follow.
MRI can be useful in distinguishing immune-mediated myelopathies from
other etiologies. Immune-mediated lesions in the spinal cord are expected to
enhance with gadolinium during the acute phase of an attack. In
immune-mediated myelopathies, enhancement on MRI indicates that the lesion
is actively inflamed, which is an important treatment consideration.
Nonenhancing lesions can also be immune mediated, especially early or late in
the course of an attack and when associated with pleocytosis on CSF analysis.26
The length and location of a lesion within the spinal cord provide additional
clues. For example, short lesions, which also tend to localize to white matter
tracts, are characteristically seen in MS. Long lesions are generally observed in
NMOSD and vascular myelopathies.27 Vascular myelopathies may localize by
vascular territory: a lesion covering the anterior two-thirds of the spinal cord is
consistent with a stroke of the anterior spinal artery.22 Neurosarcoidosis lesions
usually appear nodular on MRI and maintain a border with the meninges,
occasionally demonstrating the trident sign.28
Finally, positive serologies can be useful in diagnosis. The specificity of a
positive serum AQP4 antibody test is nearly 100% if performed with a cell-based
assay. The high specificity of this test allows any immune-mediated myelopathy
case, regardless of the clinical history; lesion length, location, or enhancement
pattern on MRI; or spinal fluid characteristics, to be considered for a diagnosis of
NMOSD. There is a very high bar for excluding NMOSD in the context of a
positive AQP4 antibody test.29 The MOG antibody cell-based assay is highly
specific when the titer is greater than 1:100; lower titers may be associated with
false positives, particularly in the context of MS.30,31 Other useful serologic
markers are described in more detail in the later sections.
MULTIPLE SCLEROSIS
A typical presentation of an MS attack in the spinal cord is a week of numbness or
heaviness in one leg. Most people with MS who develop these symptoms already
have a diagnosis of MS, and the presumption is that the symptoms are the result
CONTINUUMJOURNAL.COM 183
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
of a new immune-mediated myelopathy.18 Red flags in the history include a
severe presentation such as paralysis or a rapid progression occurring over hours.
Fever and other systemic symptoms may indicate the symptoms may be caused
by an older lesion rather than a new attack.32 Such presentations, referred to as
pseudorelapses, are stereotypical and can be familiar to the patient. Neurologic
symptoms during pseudorelapses are thought to be caused by the loss of
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
compensation or reduced neurologic reserve and should resolve with the
treatment of the underlying systemic problem.32
The workup of a myelopathy in a person with established MS would not
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
necessarily require imaging or testing unless there is some uncertainty about the
MS diagnosis or if the symptoms are particularly severe or fluctuating. On MRI, a
lesion in a person with MS is usually small (around 1 cm), focal, and localized to
the white matter tracts such as the posterior columns of the spinal cord.27
Enhancement of the lesion indicates that the attack is recent.33 If the MRI is not
consistent with an MS attack, further workup may be indicated.
Approximately 50% of cases of acute inflammatory myelitis are caused by
MS.34 In these cases, the workup commonly shows a small, focal lesion in the
spinal cord in the context of typical ovoid periventricular lesions in the brain.
CSF is positive for oligoclonal bands in more than 87% of cases,35 and serology for
AQP4 and MOG antibodies should be negative. Because spinal cord lesions
contribute to much of the disability over the lifetime of a person with MS,
aggressive disease-modifying treatment has been advocated for these patients.36
There is no consensus on the need for treatment of an acute MS attack in the
spinal cord. Data from long-term observational studies in MS suggest that
patients with attacks in the CNS may recover faster with corticosteroid
treatment; however, in the long term, there may be little to no benefit from
corticosteroids.37 It is not clear if these data can be extrapolated to lesions in the
spinal cord. Studies show a long-term benefit to acute treatment of MS attacks in
the spinal cord starting with corticosteroids and, when needed, escalating to
plasma exchange.38 Generally, severe attacks are treated whereas mild attacks
can be observed depending on the individual presentation.
NEUROMYELITIS OPTICA SPECTRUM DISORDER
NMOSD is a rare autoimmune disease in which the immune system targets the
AQP4 water channel. Although this channel is present throughout the body, the
immune attacks occur only in the CNS, primarily in the optic nerves and spinal
cord. Accepted clinical criteria for the diagnosis of NMOSD in the presence of a
positive AQP4 antibody test requires only a single attack of the spinal cord, optic
nerve, or brainstem.39 The typical presentation of an NMOSD attack of the spinal
cord is clinically severe because of the associated necrotic inflammation. NMOSD
in the spinal cord presents with severe weakness or paralysis of limbs, loss of
sensation, and loss of bowel and bladder control. Because the lesions are large,
most patients present with both weakness and numbness in multiple limbs.
Progression over 4 to 48 hours is common, but evolution can occur over 2 to
4 weeks because myelopathies may not be recognized early by patients and their
doctors. The earlier an NMOSD attack of the spinal cord is diagnosed and treated,
the better the outcomes are for the patient.40,41
The damage caused by NMOSD rarely heals completely, and most patients are
left with residual symptoms. These include persistent weakness and sensory
dysfunction but also neuropathic pain and spasticity. Fluctuation in some or all
184 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
these symptoms is very common in NMOSD and can sometimes feel like a KEY POINTS
relapse to the patient because of the intensity.42 In these situations, MRI is useful
● Neuromyelitis optica
to exclude inflammation (seen as contrast enhancement on MRI). spectrum disorder is
Lesions in NMOSD are usually not subtle on MRI. They are typically associated with a positive
longitudinally extensive, defined as spanning at least 3 vertebral segments, as serologic test for the
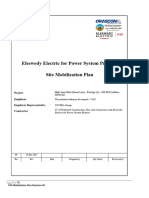
shown in CASE 8-1 and FIGURE 8-1.43 Axially, lesions are large and extend across aquaporin 4 antibody.
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
white and gray matter, often involving both sides of the spinal cord at several
● Spinal cord injury after
levels. In the acute stage, these lesions are expected to enhance although the attacks of neuromyelitis
extent of enhancement is usually shorter than the T2-hyperintense lesion. Even optica spectrum disorder is
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
after treatment, NMOSD lesions remain visible as a T2-hyperintense scar on MRI usually severe, and recovery
for many years. T2-hyperintense lesions associated with T1 hypointensities and is often poor.
atrophy indicate permanent damage to the spinal cord.44
Spinal fluid analysis is not usually required in the workup for NMOSD because
a longitudinally extensive NMOSD lesion and a positive AQP4 antibody are
sufficient to make the diagnosis. In cases in which spinal fluid has been analyzed,
acute attacks show significant pleocytosis with greater than 50 white blood cells/
mm3, which are predominantly lymphocytes but also granulocytes including
eosinophils.45 The high number of immune cells often prompts a workup for
infectious diseases, which may be useful but should not delay treatment for
NMOSD. Oligoclonal bands are rare in NMOSD; however, one study detected a
single monoclonal band unique to CSF in 18% of patients with NMOSD.8 AQP4
antibody testing is not routinely done with spinal fluid because the serum titer is
usually 250 to 400 times higher and the number of mismatches between spinal
fluid and serum is low.46
The specificity of the cell-based AQP4 antibody test is nearly 100%.29 That
means that any person who tests positive must be considered for a diagnosis of
NMOSD. Rare cases in which a false-positive AQP4 antibody test has been
reported are mostly related to low titers with enzyme-linked immunosorbent
FIGURE 8-1
Longitudinally extensive myelitis. A, Sagittal T2-weighted spine MRI shows a longitudinal
cord hyperintensity (arrows) from C1 to C5. B, Sagittal precontrast T1-weighted MRI shows a
T1 hypointense region (arrows) in the same area. C, Sagittal postcontrast T1-weighted MRI
shows an avid area of enhancement (arrows) at C2 and C3.
CONTINUUMJOURNAL.COM 185
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
assay (ELISA).47 Some cases of double-positive AQP4 and MOG have been
reported as well.48 Antibody titers in the cell-based assay do not predict the
prognosis of the disease course.49 Because NMOSD is lifelong, once a person tests
positive and a diagnosis is confirmed, repeat testing is not necessary.
All NMOSD attacks should be treated without exception. An untreated attack
will typically lead to permanent neurologic disability.50 The treatment should
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
begin with high-dose corticosteroids for 3 to 5 days, and in most cases,
therapeutic plasma exchange is indicated and helpful particularly when no
clinical benefit is achieved with corticosteroid alone.50 Other treatments such as
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
IV immunoglobulin (IVIg) and cyclophosphamide have shown benefit in small
studies.51,52 Despite prompt and appropriate treatment, most NMOSD attacks in
the spinal cord leave residual damage, and persistent deficits are common.
During the recovery process, neuropathic pain occurs in more than 60% of
patients and can severely limit rehabilitation.53 Neuropathic pain usually requires
combined medical and nonmedical treatment approaches that serve to reduce,
but not eliminate, the pain, which may subside over time.54 Similarly, muscle
spasms in previously weakened muscles are common during recovery.
Treatment with muscle relaxants may help but can exacerbate weakness.
Given poor outcomes after NMO attacks, preventive treatment is key to
improving long-term outcomes. All AQP4 antibody–positive patients with
NMOSD should be on preventive medications to avoid future attacks. Although
relapses may still occur on preventive therapy, immunosuppressive medications
can reduce the severity of breakthrough attacks.55 Three preventive therapies for
NMOSD are US Food and Drug Administration (FDA) approved: eculizumab,
satralizumab, and inebilizumab.
Eculizumab is a terminal C5 complement inhibitor that was shown to reduce
the risk of relapse by 94% over background immunosuppressive therapy for
AQP4 antibody–seropositive patients with NMOSD56 It is infused intravenously
every 2 weeks and causes very few side effects other than headache and occasional
upper respiratory infection. However, inhibiting complement increases the risk of
infection with encapsulated organisms, specifically Neisseria meningitidis. In
addition to vaccination against Neisseria, prophylactic antibiotics may be required.
Satralizumab is an interleukin-6 receptor blocker that was shown to reduce the
risk of relapse in AQP4 antibody–seropositive patients with NMOSD by 79%.57 It
is not approved for the treatment of seronegative NMOSD because of a lack of
demonstrated efficacy. The drug is injected subcutaneously once per month and
has very few side effects except for injection site reaction and occasional
laboratory abnormalities, including neutropenia and elevated lipids in
approximately 10% of patients.
Inebilizumab is a CD19 monoclonal antibody that depletes B cells along with
plasmablasts and some short-lived plasma cells. It was shown to reduce the risk of
relapse by 77% in AQP4 antibody–seropositive patients.58 It is not approved for
the treatment of seronegative NMOSD because of insufficient data in that
population. The drug is infused intravenously every 6 months and is very well
tolerated compared with rituximab. Before the approval of inebilizumab,
rituximab was widely used off-label because it was first suggested to be beneficial
in observational case series.59 In Japan, a trial of rituximab (the RIN-1 study)
demonstrated that 1000 mg of rituximab 2 times a year and low-dose
corticosteroids was superior to low-dose corticosteroids alone in preventing
relapses in AQP4 seropositive NMOSD, leading to approval in that country.60
186 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
MYELIN OLIGODENDROCYTE GLYCOPROTEIN ANTIBODY DISEASE KEY POINTS
MOG antibody disease is a relatively newly recognized clinical entity that overlaps
● In patients with
both NMOSD and MS but is also emerging as an autoimmune disease with neuromyelitis optica
distinctive features. MOG is expressed on the outer surface of the myelin sheath spectrum disorder,
and is only found in the CNS.61 Immunity to MOG has long been known to cause preventive treatment with
an inflammatory CNS disease in rodents and other animals, but the recognition immunosuppressive
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
medications is key to
that MOG immunity causes disease in humans was hampered by poor specificity
preventing attack-related
of early MOG antibody assays.62 Since 2015 with the improvement of the test, neurologic disability.
MOG antibody disease is now defined as an autoimmune disease with monophasic
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
or relapsing inflammatory attacks of the CNS.63 In children, the most common ● Among children with
clinical presentations are acute disseminated encephalomyelitis (ADEM) and demyelinating disease,
myelin oligodendrocyte
optic neuritis.64 In adults, optic neuritis accounts for more than half of attacks with glycoprotein (MOG)
inflammatory myelitis occurring in about 18% of patients.65 Myelitis may be the antibody disease is
initial event in MOG antibody disease, presenting with bladder retention, leg especially prevalent and
weakness, and sensory changes in the pelvis and legs when associated with a low commonly presents with
acute disseminated
thoracic lesion.66 Myelopathies associated with MOG antibody disease can occur encephalomyelitis (ADEM).
throughout the spinal cord and can be mild, moderate, or severe. Some cases of
MOG antibody disease present identically to NMOSD in severity of initial onset ● Spinal cord attacks in
whereas other cases are mild and more similar to MS. In addition to myelitis, MOG antibody disease can
present with severe
MOG antibody disease can cause an aseptic meningitis presentation with typical
symptoms and disability, but
features including headache and neck stiffness.66 patients generally recover
Some features of MOG antibody disease are more obvious in retrospect. If the well over time.
initial attack resembles NMOSD, the antibody tests for AQP4 and MOG are
critical to making the correct diagnosis quickly. However, with hindsight,
clinicians can distinguish MOG and NMOSD by the degree of recovery. Recovery
from NMOSD attacks is often limited as described earlier, but patients who have
MOG attacks tend to recover well.67 It is not unusual for a patient with MOG
antibody disease to be hospitalized for complete paralysis due to a thoracic
myelitis and return to the clinic in 3 to 6 months with the ability to walk again,
often unassisted.
In patients with a known history of MOG antibody disease, a new myelitis
attack is suspected when new symptoms are associated with changes on
neurologic examination that persist for more than a day. MRI of the spinal cord
typically confirms the relapse with the presence of a new or enhancing lesion.68
Lesions can be either longitudinally extensive (FIGURE 8-2) or focal and can
involve both gray and white matter tracts. A distinctive MRI finding in MOG
antibody disease is that recovery after myelitis tends to normalize the spinal
cord lesion so that old lesions may not be visualized on subsequent scans. This
has led to the notion that MOG antibody disease may be the cause of “MRI-
negative myelitis” in which patients with suspected inflammatory myelitis do
not have a lesion on MRI.69
Although the most common cause of inflammatory myelitis in the US
population is MS, consideration of NMOSD and MOG is particularly relevant
when the brain is radiographically spared on MRI. Given the ease of antibody
testing and the widely different treatment plans among NMOSD, MS, and MOG
antibody disease, there is a consensus that AQP4 and MOG antibodies should be
tested in all initial cases of inflammatory myelitis.
Oligoclonal bands are rare in MOG antibody disease.62 In cases where MOG
antibody disease and MS are both high on the differential diagnosis, a positive
oligoclonal band test can help push the diagnosis toward MS. Similar to CSF
CONTINUUMJOURNAL.COM 187
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
findings during acute attacks in
NMOSD, MOG attacks can
present with marked pleocytosis
(>50 white blood cells/mm3),
predominantly lymphocytes.70
Such white blood cell elevations
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
are rare in MS.
The MOG antibody test was
improved in 2015 to minimize the
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
false positive tests that plagued the
assay since it was originally
published in 1999.71 The new assay
uses a cell-based approach with
the full-length extracellular
FIGURE 8-2 portion of MOG rather than an
Myelin oligodendrocyte glycoprotein (MOG) ELISA using MOG peptides. In
antibody–seropositive optic neuritis. This axial addition, the detection of human
postcontrast T1-weighted brain MRI shows avid
contrast enhancement extending a little more
MOG antibodies with this method
than half the length of the optic nerve (arrows) screens out IgM antibodies, which
primarily in the anterior portion and sparing are commonly found in healthy
the chiasm. people. In some laboratories, only
IgG1 antibodies to MOG are
considered positive for this assay
whereas in others the IgG is considered positive if above a specific titer. Titer
appears to be important in MOG antibody disease in two ways. First, a high titer
bolsters specificity with levels of 1:1000 or greater being 100% specific.30,31
Lower MOG antibody levels should prompt consideration of other conditions,
including MS. Second, MOG antibody titers can be tracked over time because
those whose MOG antibody assays normalize have a lower risk of
subsequent relapse.72
There are no approved therapies for MOG antibody disease, either for acute
relapse or for preventive use. Treatment of relapses seems to respond to high
doses of corticosteroids.73 Patients typically receive 3 to 5 days of high-dose IV
steroids followed by a 2- to 3-month taper. The taper ensures continued
anti-inflammatory effect but also prevents a steroid-withdrawal relapse to which
patients with MOG antibody disease are prone. New data also suggest that IVIg
may be effective in suppressing acute inflammation and can spare the associated
toxicity of 2 to 3 months of steroid treatment.
Preventively, many patients with MOG antibody disease are administered
IVIg every 4 weeks. Depending on the dose, the risk of relapse can be reduced
60% to 80%.74 Aseptic meningitis and blood clots are potential side effects of
IVIg, but they can be mitigated by using a subcutaneous route.75 Mycophenolate
mofetil and azathioprine have been used in the treatment of MOG antibody
disease, especially in children, with generally good outcomes.76
Two medications are being developed for preventive uses in MOG antibody
disease. Rozanolixizumab is a neonatal Fc receptor (FcRn) monoclonal antibody
that blocks the ability of FcRn to prevent intravascular antibodies from being
destroyed and recycled.77 A phase 3, randomized, placebo-controlled trial is
underway to test the ability of rozanolixizumab to prevent relapses in MOG
antibody disease. A phase 3, randomized, placebo-controlled trial of
188 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
satralizumab, which is already approved for NMOSD (see above), is also KEY POINTS
underway to test its ability to prevent relapses in MOG antibody disease.78
● The criteria for MOG
Both trials are expected to report results in 2025 to 2026. antibody disease depends
on the MOG antibody titer
OTHER ANTIBODY-ASSOCIATED AUTOIMMUNE DISEASES level; high-titer positive
Rare cases of immune-mediated myelopathies occur in the context of other MOG antibody tests confer a
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
diagnosis of MOG antibody
known autoantibodies. Most notably, glial fibrillary acidic protein (GFAP)
disease.
encephalomyelitis is among the more common of these rare conditions.79
GFAP encephalomyelitis is a monophasic immune-mediated attack on the ● Seronegative relapsing
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
astrocyte protein GFAP, which typically presents as an acute encephalitis, inflammatory myelitis likely
meningoencephalitis, or encephalomyelitis. Like for other forms of autoimmune includes a mix of different
conditions that have yet to
myelitis, treatment of GFAP encephalomyelitis starts with high-dose IV be specifically defined.
corticosteroids and a prolonged oral taper; plasma exchange may be helpful
when corticosteroids are insufficient.79 Although outcomes are generally good
after treatment, patients with spinal cord involvement may have residual
myelopathic symptoms.
Other autoantibodies that have been reported in association with myelitis
include anti-glutamic acid decarboxylase (GAD),80 antiglycine receptor in the
context of progressive encephalomyelitis with rigidity and myoclonus,81,82 and
antiamphiphysin antibodies.83,84
SERONEGATIVE RELAPSING INFLAMMATORY MYELITIS
With improvements in the cell-based assays for AQP4, MOG, and paraneoplastic
antibodies, new cases of seronegative relapsing transverse myelitis are becoming
more rare. A select number of cases remain seronegative despite repeated testing
in the setting of recurrent inflammatory attacks of the spinal cord. This might
reflect the limited sensitivity of these assays, incorrect diagnosis, or other
autoantibodies that may have not been discovered.
Among other causes of myelopathy, neurosarcoidosis, discussed later in this
article, and vascular myelopathies should be given special consideration. For more
information about vascular myelopathy, refer to the article “Vascular Myelopathies”
by Ashutosh P. Jadhav, MD, PhD, FAAN,2 in this issue of Continuum.
There is a consensus that a single event of seronegative inflammatory myelitis
does not necessarily predict a relapsing disease course.85 However, a spatially and
temporally distinct second attack is a good indication that the disease is relapsing.
Even if persistently seronegative, the trend in the field is to offer preventive
medication to prevent a third attack. Additionally, if patients relapse despite an
adequate trial of an appropriate medication, they are usually switched to a
different mechanism of treatment. For example, if a patient with a history of
seronegative relapsing inflammatory myelitis has a new inflammatory lesion in
the spinal cord while B cell counts are zero following treatment with rituximab,
the presumption is that B cell depletion is not going to be an effective preventive
therapy for the patient.
The clinical presentation of seronegative inflammatory myelitis ranges from
NMOSD to MS in severity, location, and chronicity. Although it might be
easy to categorize seronegative inflammatory myelitis as part of MS, patients
with seronegative inflammatory myelitis usually have been spared brain disease
both clinically and radiologically. They also have no oligoclonal bands in the
CSF and thus do not easily meet the criteria for MS. There has been a tendency
to pigeonhole these patients into “NMOSD-like” versus “MOG antibody
CONTINUUMJOURNAL.COM 189
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
disease–like” categories based on their MRI patterns and responses to
treatments. Patients with lesions that remain bright on T2-weighted MRI long
after an attack and who seem to respond clinically to B cell therapies are
considered to have an “NMOSD-like” presentation whereas those whose spinal
cord lesions recover well over time and do not respond well to B cell therapies
may be labeled as having an “MOG antibody disease–like” presentation. In
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
addition to B cell–depletion therapies, other patients with an “NMOSD-like”
presentation may respond to interleukin 6 blockers such as tocilizumab.
“MOG antibody disease–like” therapy includes IVIg. Patients may opt for
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
a broad immunosuppressive approach such as mycophenolate mofetil or
azathioprine.
MONOPHASIC IDIOPATHIC INFLAMMATORY MYELITIS
Monophasic idiopathic inflammatory myelitis refers to a single inflammatory
attack of the spinal cord that is not the result of MS, NMOSD, or MOG antibody
disease. Originally coined in 1948,86 the term transverse myelitis was used to define
an inflammatory attack of the spinal cord that presented with bilateral symptoms
due to disease across a transverse section of the spinal cord and corresponding
dermatomal distribution. In 2002, the bilateral requirement was incorporated
into the Transverse Myelitis Working Group’s formalized criteria for the
diagnosis of inflammatory myelitis, which, although now somewhat outdated,
attempted to distinguish inflammatory from noninflammatory etiologies.5 MRI
visualization of lesions negated the bilateral requirement that was previously
helpful to spinal cord localization.
Triggers for inflammatory myelitis have historically included vaccines and
infections of many different kinds.87 The COVID-19 pandemic provided a unique
situation in which to study immunologic triggers because testing was widely
available and infections were documented. Also, large populations received the
vaccine essentially at the same time. In one of the most closely watched trials of
one COVID-19 vaccine, the first COVID-19 vaccine trial to be published, three
people developed inflammatory myelitis during the study, only one of which was
determined to be caused by the vaccine.88 In addition to vaccines, infections may
also trigger attacks. For example, there are a similar number of case reports of
inflammatory myelitis following COVID-19 infection as there are following
COVID-19 vaccination, both of which were low frequency in the
general population.89,90
MRI lesions of idiopathic inflammatory myelitis vary in size and location.
Longitudinally extensive lesions are more commonly associated with NMOSD
and MOG than with idiopathic inflammatory myelitis, which tends to span less
than three vertebral lengths.42 Transverse myelitis does not preferentially target
gray versus white matter tracts as MS does. Gadolinium enhancement is
associated with active inflammation in inflammatory myelitis although, in some
cases of severe inflammatory myelitis, persistent enhancement is seen
throughout recovery. Over time, inflammatory myelitis lesion scars transition to
a residual nonenhancing T2 hyperintensity.
Spinal fluid analysis may be used in place of MRI contrast enhancement to
confirm the presence of an inflammatory process. The presence of pleocytosis is
not exclusive to immune-mediated myeloapthies; many nonimmune
myelopathies can cause damage to the spinal cord, which recruits an immune
cellular response. However, a higher number of cells, particularly greater than
190 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
50 white blood cells/mm3, should be worked up for a primary immune- KEY POINTS
mediated myelopathy.
● Broad-spectrum
Treatment for idiopathic inflammatory myelitis begins with suppression of the immunosuppression can be
inflammatory process by using high-dose corticosteroids. Escalated therapy to useful in preventing relapses
therapeutic plasma exchange or cyclophosphamide or both should be considered of seronegative relapsing
when the response to steroids is poor.91 Once the inflammation subsides, the inflammatory myelitis.
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
recovery can take 6 to 18 months or more depending on the extent of damage.
● Monophasic idiopathic
Recovery is rarely complete, and patients are frequently left with some degree of inflammatory myelitis is a
weakness, numbness, and neuropathic pain. The one-third prognosis rule was one-time immunologic event
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
published in the early 1980s based on an observational case series in which about that leads to spinal cord
one-third of patients recovered well, one-third made some recovery back to injury.
walking with assistance, and one-third had a poor outcome.92 With modernized ● A link between
and more intensive immunosuppressive therapy initiated as early as possible in the inflammatory myelitis and
course of the condition, the expectation is that patients will have better recoveries. vaccines has been
Even in patients who do not make meaningful recoveries, initiating treatment speculated but not
confirmed.
for idiopathic inflammatory myelitis appears to blunt the progressive decline in
neurologic function. Nearly all studies in transverse myelitis using various forms ● Neurosarcoidosis in the
of immunosuppression show that the nadir of disease is reached just before spinal cord should be
treatment is started. This pattern suggests that, without treatment, some patients suspected in cases with MRI
lesions that are persistently
would have continued to progress in their disease course. Some patients present
enhancing over a long
too late for treatment. If the inflammation has already subsided naturally as period.
indicated by stable neurologic deficits, nonenhancing lesion on MRI, and no
pleocytosis on CSF analysis, there is a reduced expectation that ● Steroids are often
immunosuppressive therapy would be helpful. sufficient to treat
neurosarcoidosis of the
After inflammation subsides and recovery begins, physical therapy is spinal cord, but newer
important to optimizing long-term neurologic function.93 treatments, such as anti–
tumor necrosis factor
NEUROSARCOIDOSIS medications, are available.
Neurosarcoidosis is a granulomatous inflammatory disease that affects the CNS.
● The differential diagnosis
In the spine, non-necrotizing epithelioid granulomas slowly grow into the CNS of immune-mediated
parenchyma from the spinal meninges triggering a lymphocytic inflammatory myelopathies can be
reaction leading to a subacute or chronic myelopathy.94 In the basal meninges, narrowed by workup that
uses imaging, serology,
neurosarcoidosis can cause cranial neuropathies in addition to headaches and
spinal fluid analysis, and
papilledema due to increased intracranial pressure depending on where the sometimes histopathology.
granulomas grow. Ninety percent of cases of neurosarcoidosis occur in the
context of systemic sarcoidosis, usually in the lung, but it is frequently the
neurologic symptoms that prompt the workup.95
The clinical presentations of neurosarcoidosis depend on the location of the
granulomatous inflammation, but in most cases, the progression of decline is
subacute or chronic, occurring over weeks to months. Because granulomas
usually grow into the cord from the meninges, white matter tracts are affected
more commonly than gray matter, leading to long tract signs that affect motor
and sensory function below the level of the lesion.
The gold standard for diagnosis is biopsy of the CNS lesion with demonstration
of a noncaseating granuloma, which is usually surrounded by a ring of fibroblasts
mixed with lymphocytes. In most cases, workup of neurosarcoidosis identifies
other granulomas, such as in the lung and spleen, that are easier to biopsy than
in the CNS; positive findings confer a diagnosis of probable neurosarcoidosis.
When neurosarcoidosis is diagnosed on clinical grounds without biopsy
confirmation, it is considered possible neurosarcoidosis.96 Clinical grounds to
CONTINUUMJOURNAL.COM 191
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
make a diagnosis depend on the rest of the workup by MRI, positron emission
tomography (PET), and CSF and blood testing.
On MRI, neurosarcoid lesions are avidly enhancing with gadolinium, and they
almost always attach to the meninges in the basal cisterns or spinal column.97
In the axial plane, the pattern resembles a trident because of confluent central
canal and dorsal subpial enhancement. They are nodular in appearance and can
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
include a longitudinally extensive T2-hyperintense halo depending on how
inflamed the granuloma is. Even after the start of the treatment, neurosarcoid
lesions distinguish themselves from other causes of immune-mediated
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
myelopathies in that they remain persistently contrast enhancing for at least
6 weeks, and often more than that.98 They tend to shrink in size over time with
ongoing immunosuppressive treatments and eventually disappear.
In the initial workup, fludeoxyglucose (FDG)-PET is useful in two ways.
First, FDG avidity of the spinal cord lesion supports the diagnosis of
neurosarcoidosis and the decision to pursue a spine biopsy.99 Usually, a biopsy
of the meninges is sufficient to find a granuloma, and the spinal cord can be
spared. Second, even when the spinal cord lesion is avid, scans of the chest and
abdomen often identify an avid lesion in the lungs or spleen that would provide
for an easier biopsy target than the spine or brain.
Spinal fluid analysis usually demonstrates a mix of pleocytosis and low
glucose. Neurosarcoidosis is distinctive among immune-mediated
(noninfectious) causes of myelopathy in causing glucose levels in the low range
of 20 mg/dL to 40 mg/dL (reference range, 60 mg/dL to 100 mg/dL).94 CSF
angiotensin-converting enzyme, produced by macrophages within the
granuloma, is a relatively specific finding in neurosarcoidosis but has low
sensitivity.100 Blood testing for angiotensin-converting enzyme has a lower
specificity than the CSF and is generally not recommended in the workup for
neurosarcoidosis. Soluble interleukin 2 released by activated T cells has been
proposed recently as a marker for sarcoidosis with a sensitivity and specificity
of 88% and 85% in biopsy-proven cases.101,102 However, when tested in the CSF
for neurosarcoidosis, soluble interleukin 2 was not specific except to help
exclude MS.103
Although mild cases of systemic sarcoidosis may not require treatment,
neurosarcoidosis is almost always treated to reverse neurologic symptoms and
prevent progression. Severe or acute cases of myelopathy should be treated with
high doses of corticosteroids, similar to the treatment for inflammatory myelitis,
although the expectation in neurosarcoidosis is that immunosuppressive
treatment for several months or even years may be necessary to achieve full
remission.94 Corticosteroids can be converted to lower oral doses, but in the long
term, the required doses of corticosteroids may cause significant side
effects.94,104 Steroid-sparing agents, such as mycophenolate and methotrexate,
may be added to permit lower doses of steroids. Infliximab, a tumor necrosis
factor inhibitor, is effective and safe in neurosarcoidosis, even in cases that are
not responsive to corticosteroids.105 More recently, JAK/STAT inhibitors have
been shown to be useful in systemic sarcoidosis.106
PARANEOPLASTIC DISEASE
Paraneoplastic myelopathy should be suspected in any patient with myelopathy
in the setting of cancer. The most common cancer associated with paraneoplastic
myelopathy is small cell lung cancer, and associated autoantibodies are usually
192 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
anti-Hu, collapsin response mediator protein-5 (CRMP5), or amphiphysin
antibodies.107
Myelopathy can be the initial presentation leading to the diagnosis of cancer.
In patients older than 55 who present with myelopathy, vascular and
paraneoplastic myelopathy should be considered the differential diagnosis,
especially with a weeks- to months-long history of unintended weight loss, night
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
sweats, or both. MRI features that favor paraneoplastic myelopathy include
longitudinally extensive lesions that appear to track along the white matter in the
spinal cord, brainstem, or brain, which is called tractopathy.108 Another MRI
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
feature of paraneoplastic myelopathy is necrotic destruction with contrast
enhancement and T1 hypointensity.109 Necrotizing myelopathy in paraneoplastic
disease is a poor prognostic sign.110 Some cases of aggressive paraneoplastic
myelopathy can overlap with AQP4-seropositive NMOSD.111,112
Detection of serologic antibodies to Hu, CRMP5, or amphiphysin should
prompt a cancer workup, including imaging of the chest and abdomen by CT,
PET, or both. Treatment is directed at the underlying cancer, which is usually
immunosuppressive as well. Even when the cancer is treatable, neurologic
damage may be permanent, particularly in the cerebellum and spinal cord.
CONCLUSION
Immune-mediated myelopathies share a common mechanism of immune
dysfunction that targets the spinal cord. There are many other causes of
myelopathy that can mimic immune-mediated myelopathies. In distinguishing
among the several specific causes of immune-mediated myelopathies, a workup
that includes objective data in the form of serology, imaging, spinal fluid analysis,
and, in some cases, histopathology is helpful in narrowing the differential
diagnosis. Newly approved and emerging therapies are available for specific
immune-mediated myelopathies, with more in development.
ACKNOWLEDGMENT
This work was supported by a grant from the National Institutes of Health
(R01 AI153068).
REFERENCES
1 Fletcher A, Bhattacharyya S. Infectious 5 Transverse Myelitis Consortium Working Group.
myelopathies. Continuum (Minneap Minn) 2024; Proposed diagnostic criteria and nosology of
30(1, Spinal Cord Disorders):133-159. acute transverse myelitis. Neurology 2002;59(4):
499-505. doi:10.1212/wnl.59.4.499
2 Jadhav A. Vascular myelopathies. Continuum
(Minneap Minn) 2024;30(1, Spinal Cord 6 Nachamkin I, Allos BM, Ho T. Campylobacter
Disorders):160-179. species and Guillain-Barré syndrome. Clin
Microbiol Rev 1998;11(3):555-567. doi:10.1128/
3 Pardo CA. Clinical approach to myelopathy
CMR.11.3.555
diagnosis. Continuum (Minneap) (Minn) 2024;
30(1, Spinal Cord Disorders):14-52. 7 Zrzavy T, Kollaritsch H, Rommer PS, et al.
Vaccination in multiple sclerosis: friend or foe?
4 Stadelmann C, Timmler S, Barrantes-Freer A,
Front Immunol 2019;10:1883. doi:10.3389/
Simons M. Myelin in the central nervous system:
fimmu.2019.01883
structure, function, and pathology. Physiol Rev
2019;99(3):1381-1431. doi:10.1152/
physrev.00031.2018
CONTINUUMJOURNAL.COM 193
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
8 Mealy MA, Wingerchuk DM, Greenberg BM, Levy 22 Barreras P, Fitzgerald KC, Mealy MA, et al. Clinical
M. Epidemiology of neuromyelitis optica in the biomarkers differentiate myelitis from vascular
United States: a multicenter analysis. Arch Neurol and other causes of myelopathy. Neurology 2018;
2012;69(9):1176-1180. doi:10.1001/ 90(1):e12-e21. doi:10.1212/
archneurol.2012.314 WNL.0000000000004765
9 Polgár A, Rózsa C, Müller V, et al. Devic’s 23 Barry E, Hauser WA. Pleocytosis after status
syndrome and SLE: challenges in diagnosis and epilepticus. Arch Neurol 1994;51(2):190-193.
therapeutic possibilities based on two doi:10.1001/archneur.1994.00540140100019
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
overlapping cases. Autoimmun Rev 2011;10(3):
24 Travlos A, Anton HA, Wing PC. Cerebrospinal
171-174. doi:10.1016/j.autrev.2010.09.021
fluid cell count following spinal cord injury. Arch
10 Pittock SJ, Lennon VA, de Seze J, et al. Phys Med Rehabil 1994;75(3):293-296.
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
Neuromyelitis optica and non organ-specific doi:10.1016/0003-9993(94)90032-9
autoimmunity. Arch Neurol 2008;65(1):78-83.
25 Baunbæk Egelund G, Ertner G, Langholz
doi:10.1001/archneurol.2007.17
Kristensen K, et al. Cerebrospinal fluid
11 Sofat N, Venables PJ. Is Sjogren myelopathy pleocytosis in infectious and noninfectious
Devic disease? Ann Rheum Dis 2008;67(5): central nervous system disease: a retrospective
730-731. doi:10.1136/ard.2007.077883 cohort study. Medicine (Baltimore) 2017;96(18):
e6686. doi:10.1097/MD.0000000000006686
12 Fan S, Xu Y, Ren H, et al. Comparison of myelin
oligodendrocyte glycoprotein (MOG)-antibody 26 Mustafa R, Passe TJ, Lopez-Chiriboga AS, et al.
disease and AQP4-IgG-positive neuromyelitis Utility of MRI enhancement pattern in
optica spectrum disorder (NMOSD) when they myelopathies with longitudinally extensive T2
co-exist with anti-NMDA (N-methyl-D-aspartate) lesions. Neurol Clin Pract 2021;11(5):e601-e611.
receptor encephalitis. Mult Scler Relat Disord doi:10.1212/CPJ.0000000000001036
2018;20:144-152. doi:10.1016/j.msard.2018.01.007
27 Goh C, Desmond PM, Phal PM. MRI in transverse
13 Krumholz A, Stern BJ. Neurologic manifestations myelitis. J Magn Reson Imaging JMRI 2014;40(6):
of sarcoidosis. Handb Clin Neurol 2014;119: 1267-1279. doi:10.1002/jmri.24563
305-333. doi:10.1016/B978-0-7020-4086-3.00021-7
28 Kumar N, Frohman EM. Spinal neurosarcoidosis
14 Lopez Chiriboga S, Flanagan EP. Myelitis and mimicking an idiopathic inflammatory
other autoimmune myelopathies. Continuum demyelinating syndrome. Arch Neurol 2004;61(4):
(Minneap Minn) 2021;27(1, Spinal Cord Disorders): 586-589. doi:10.1001/archneur.61.4.586
62-92. doi:10.1212/CON.0000000000000900
29 Prain K, Woodhall M, Vincent A, et al. AQP4
15 Nourbakhsh B, Mowry EM. Multiple sclerosis risk antibody assay sensitivity comparison in the era
factors and pathogenesis. Continuum (Minneap of the 2015 diagnostic criteria for NMOSD. Front
Minn) 2019;25(3, Neuro-ophthalmology):596-610. Neurol 2019;10:1028. doi:10.3389/
doi:10.1212/CON.0000000000000725 fneur.2019.01028
16 Hawkes CH. Multiple sclerosis genetics is dead. 30 Manzano GS, Salky R, Mateen FJ, et al. Positive
Mult Scler Relat Disord 2013;2(3):156-161. predictive value of MOG-IgG for clinically
doi:10.1016/j.msard.2012.12.006 defined MOG-AD within a real-world cohort.
Front Neurol 2022;13:947630. doi:10.3389/fneur.
17 Ebers GC, Sadovnick AD, Dyment DA, et al.
2022.947630
Parent-of-origin effect in multiple sclerosis:
observations in half-siblings. Lancet Lond Engl 31 Sechi E, Buciuc M, Pittock SJ. Positive predictive
2004;363(9423). doi:10.1016/S0140-6736(04) value of myelin oligodendrocyte glycoprotein
16304-6 autoantibody testing. JAMA Neurol 2021;78(6):
741-746. doi:10.1001/jamaneurol.2021.0912
18 Bot JCJ, Barkhof F, Polman CH, et al. Spinal cord
abnormalities in recently diagnosed MS patients: 32 Repovic P. Management of multiple sclerosis
added value of spinal MRI examination. relapses. Continuum (Minneap Minn) 2019;25(3,
Neurology 2004;62(2):226-233. doi:10.1212/ Multiple Sclerosis and Other CNS Inflammatory
wnl.62.2.226 Diseases):655-669. doi:10.1212/
CON.0000000000000739
19 Bourre B, Zéphir H, Ongagna JC, et al. Long-term
follow-up of acute partial transverse myelitis. 33 Karimian-Jazi K, Neuberger U, Schregel K, et al.
Arch Neurol 2012;69(3):357-362. doi:10.1001/ Diagnostic value of gadolinium contrast
archneurol.2011.949 administration for spinal cord magnetic
resonance imaging in multiple sclerosis patients
20 Mealy MA, Nam TS, Pardo SJ, et al. Familial
and correlative markers of lesion enhancement.
monophasic acute transverse myelitis due to the
Mult Scler J 2021;7(4):20552173211047976.
pathogenic variant in VPS37A. Neurol Genet 2018;
doi:10.1177/20552173211047978
4(1):e213. doi:10.1212/NXG.0000000000000213
34 Young J, Quinn S, Hurrell M, Taylor B. Clinically
21 Matiello M, Kim HJ, Kim W, et al. Familial
isolated acute transverse myelitis: prognostic
neuromyelitis optica. Neurology 2010;75(4):
features and incidence. Mult Scler Houndmills
310-315. doi:10.1212/WNL.0b013e3181ea9f15
Basingstoke Engl 2009;15(11):1295-1302.
doi:10.1177/1352458509345906
194 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
35 Dobson R, Ramagopalan S, Davis A, Giovannoni 46 Majed M, Fryer JP, McKeon A, Lennon VA, Pittock
G. Cerebrospinal fluid oligoclonal bands in SJ. Clinical utility of testing AQP4-IgG in CSF:
multiple sclerosis and clinically isolated guidance for physicians. Neurol Neuroimmunol
syndromes: a meta-analysis of prevalence, Neuroinflammation 2016;3(3):e231. doi:10.1212/
prognosis and effect of latitude. J Neurol NXI.0000000000000231
Neurosurg Psychiatry 2013;84:909-914.
47 Fryer JP, Lennon VA, Pittock SJ, et al. AQP4
36 Bussas M, El Husseini M, Harabacz L, et al. autoantibody assay performance in clinical
Multiple sclerosis lesions and atrophy in the laboratory service. Neurol Neuroimmunol
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
spinal cord: distribution across vertebral levels Neuroinflammation 2014;1(1):e11. doi:10.1212/
and correlation with disability. NeuroImage Clin NXI.0000000000000011
2022;34:103006. doi:10.1016/j.nicl.2022.103006
48 Molazadeh N, Bose G, Lotan I, Levy M.
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
37 Burton JM, O’Connor PW, Hohol M, Beyene J. Autoimmune diseases and cancers overlapping
Oral versus intravenous steroids for treatment of with myelin oligodendrocyte glycoprotein
relapses in multiple sclerosis. Cochrane antibody-associated disease (MOGAD): a
Database Syst Rev 2012;12:CD006921. systematic review. Mult Scler J 2022;8(4):
doi:10.1002/14651858.CD006921.pub3 20552173221128170. doi:10.1177/20552173221128170
38 Weinshenker BG, O’Brien PC, Petterson TM, et al. 49 Jitprapaikulsan J, Fryer JP, Majed M, et al. Clinical
A randomized trial of plasma exchange in acute utility of AQP4-IgG titers and measures of
central nervous system inflammatory complement-mediated cell killing in NMOSD.
demyelinating disease. Ann Neurol 1999;46(6): Neurol Neuroimmunol Neuroinflammation 2020;
878-886. doi:10.1002/1531-8249(199912)46:6<878:: 7(4):e727. doi:10.1212/NXI.0000000000000727
aid-ana10>3.0.co;2-q
50 Kimbrough DJ, Fujihara K, Jacob A, et al.
39 Wingerchuk DM, Banwell B, Bennett JL. Treatment of neuromyelitis optica: review and
International consensus diagnostic criteria for recommendations. Mult Scler Relat Disord 2012;
neuromyelitis optica spectrum disorders. 1(4):180-187. doi:10.1016/j.msard.2012.06.002
Neurology 2015;85(2):177-189. doi:10.1212/
51 Magraner MJ, Coret F, Casanova B. The effect of
WNL.0000000000001729
intravenous immunoglobulin on neuromyelitis
40 Abboud H, Petrak A, Mealy M. Treatment optica. Neurologia 2013;28(2):65-72. doi:10.1016/
of acute relapses in neuromyelitis optica: j.nrl.2012.03.014
steroids alone versus steroids plus plasma
52 Yaguchi H, Sakushima K, Takahashi I, et al.
exchange. Mult Scler 2016;22(2):185-192.
Efficacy of intravenous cyclophosphamide
doi:10.1177/1352458515581438
therapy for neuromyelitis optica spectrum
41 Ipe TS, Raval JS, Fernando LP, et al. Therapeutic disorder. Intern Med Tokyo Jpn 2013;52(9):
plasma exchange for neuromyelitis optica 969-972. doi:10.2169/internalmedicine.52.7885
spectrum disorder: a multicenter retrospective
53 Zhao S, Mutch K, Elsone L, Nurmikko T, Jacob A.
study by the ASFA neurologic diseases
Neuropathic pain in neuromyelitis optica affects
subcommittee. J Clin Apheresis 2020;35(1):25-32.
activities of daily living and quality of life. Mult
doi:10.1002/jca.21754
Scler Houndmills Basingstoke Engl 2014;20(12):
42 Kimbrough DJ, Mealy MA, Simpson A, Levy M. 1658-1661. doi:10.1177/1352458514522103
Predictors of recurrence following an initial
54 Abboud H, Salazar-Camelo A, George N, et al.
episode of transverse myelitis. Neurol
Symptomatic and restorative therapies in
Neuroimmunol Neuroinflammation 2014;1(1):e4.
neuromyelitis optica spectrum disorders.
doi:10.1212/NXI.0000000000000004
J Neurol 2022;269(4). doi:10.1007/s00415-021-
43 Mealy MA, Whetstone A, Orman G, et al. 10783-4
Longitudinally extensive optic neuritis as an MRI
55 Levy M, Fujihara K, Palace J. New therapies for
biomarker distinguishes neuromyelitis optica
neuromyelitis optica spectrum disorder. Lancet
from multiple sclerosis. J Neurol Sci 2015;355(0):
Neurol 2021;20(1):60-67. doi:10.1016/S1474-4422
59-63. doi:10.1016/j.jns.2015.05.013
(20)30392-6
44 Salama S, Levy M. Bright spotty lesions as an
56 Pittock SJ, Berthele A, Fujihara K. Eculizumab in
imaging marker for neuromyelitis optica
aquaporin-4-positive neuromyelitis optica
spectrum disorder. Mult Scler Houndmills
spectrum disorder. N Engl J Med 2019;381(7):
Basingstoke Engl 2022;28(11):1663-1666.
614-625. doi:10.1056/NEJMoa1900866
doi:10.1177/1352458521994259
57 Traboulsee A, Greenberg BM, Bennett JL. Safety
45 Jarius S, Paul F, Franciotta D. Cerebrospinal fluid
and efficacy of satralizumab monotherapy in
findings in aquaporin-4 antibody positive
neuromyelitis optica spectrum disorder: a
neuromyelitis optica: results from 211 lumbar
randomised, double-blind, multicentre,
punctures. J Neurol Sci 2011;306(1-2):82-90.
placebo-controlled phase 3 trial. Lancet Neurol
doi:10.1016/j.jns.2011.03.038
2020;19(5):402-412. doi:10.1016/S1474-4422(20)
30078-8
CONTINUUMJOURNAL.COM 195
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
58 Cree BAC, Bennett JL, Kim HJ. Inebilizumab for 70 Jarius S, Ruprecht K, Kleiter I. MOG-IgG in NMO
the treatment of neuromyelitis optica spectrum and related disorders: a multicenter study of 50
disorder (N-MOmentum): a double-blind, patients. Part 1: frequency, syndrome specificity,
randomised placebo-controlled phase 2/3 trial. influence of disease activity, long-term course,
Lancet 2019;394(10206):1352-1363. doi:10.1016/ association with AQP4-IgG, and origin.
S0140-6736(19)31817-3 J Neuroinflammation 2016;13(1):279. doi:10.1186/
s12974-016-0717-1
59 Levy M, Mealy MA. B-cell targeted treatments
for neuromyelitis optica spectrum disorder: a 71 Waters P, Woodhall M, O’Connor KC. MOG
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
focus on CD19 and CD20. ImmunoTargets Ther cell-based assay detects non-MS patients with
2021;10:325-331. doi:10.2147/ITT.S255722 inflammatory neurologic disease. Neurol
Neuroimmunol Neuroinflamm 2015;2(3):89.
60 Tahara M, Oeda T, Okada K, et al. Safety and
doi:10.1212/NXI.0000000000000089
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
efficacy of rituximab in neuromyelitis optica
spectrum disorders (RIN-1 study): a multicentre, 72 Gastaldi M, Foiadelli T, Greco G, et al. Prognostic
randomised, double-blind, placebo-controlled relevance of quantitative and longitudinal MOG
trial. Lancet Neurol 2020;19(4):298-306. antibody testing in patients with MOGAD: a
doi:10.1016/S1474-4422(20)30066-1 multicentre retrospective study. J Neurol
Neurosurg Psychiatry 2023;94(3):201-210.
61 Delarasse C, Della Gaspera B, Lu CW, et al.
doi:10.1136/jnnp-2022-330237
Complex alternative splicing of the myelin
oligodendrocyte glycoprotein gene is unique to 73 Whittam DH, Karthikeayan V, Gibbons E, et al.
human and non-human primates. J Neurochem Treatment of MOG antibody associated
2006;98(6):1707-1717. doi:10.1111/j.1471-4159.2006. disorders: results of an international survey.
04053.x J Neurol 2020;267(12):3565-3577. doi:10.1007/
s00415-020-10026-y
62 Waters PJ, Komorowski L, Woodhall M. A
multicenter comparison of MOG-IgG cell-based 74 Chen J, Huda S, Hacohen Y, et al.
assays. Neurology 2019;92(11). doi:10.1212/WNL. Association of maintenance intravenous
0000000000007096 immunoglobulin with prevention of relapse in
adult myelin oligodendrocyte glycoprotein
63 Banwell B, Bennett JL, Marignier R, et al.
antibody-associated disease. JAMA Neurol 2022;
Diagnosis of myelin oligodendrocyte
79(5):518-525. doi:10.1001/jamaneurol.2022.0489
glycoprotein antibody-associated disease:
International MOGAD Panel proposed criteria. 75 Sotirchos ES, Vasileiou ES, Salky R, et al.
Lancet Neurol 2023;22(3):268-282. doi:10.1016/ Treatment of myelin oligodendrocyte
S1474-4422(22)00431-8 glycoprotein antibody associated disease with
subcutaneous immune globulin. Mult Scler
64 Otallah S, Banwell B. Pediatric multiple sclerosis:
Relat Disord 2022;57:103462. doi:10.1016/
an update. Curr Neurol Neurosci Rep 2018;18(11):
j.msard.2021.103462
76. doi:10.1007/s11910-018-0886-7
76 Hacohen Y, Wong YY, Lechner C. Disease course
65 Jurynczyk M, Messina S, Woodhall MR. Clinical
and treatment responses in children with
presentation and prognosis in MOG-antibody
relapsing myelin oligodendrocyte glycoprotein
disease: a UK study. Brain 2017;140(12):3128-3138.
antibody-associated disease. JAMA Neurol 2018;
doi:10.1093/brain/awx276
75(4):478-487. doi:10.1001/jamaneurol.2017.4601
66 Salama S, Khan M, Pardo S, Izbudak I, Levy M.
77 ClinicalTrials.gov. A randomized, double-blind,
MOG antibody-associated encephalomyelitis/
placebo-controlled, multicenter, phase 3, pivotal
encephalitis. Mult Scler Houndmills Basingstoke
study with an open-label extension period to
Engl 2019;25(11):1427-1433. doi:10.1177/
evaluate the efficacy and safety of
1352458519837705
rozanolixizumab in adult participants with myelin
67 Ciotti JR, Eby NS, Wu GF, et al. Clinical and oligodendrocyte glycoprotein (mog)
laboratory features distinguishing MOG antibody antibody-associated disease (mog-ad)
disease from multiple sclerosis and AQP4 (NCT05063162). Updated October 13, 2023.
antibody-positive neuromyelitis optica. Mult Accessed November 29, 2023. clinicaltrials.gov/
Scler Relat Disord 2020;45(102399). doi:10.1016/ study/NCT05063162
j.msard.2020.102399
78 ClinicalTrials.gov. A phase III, randomized,
68 Salama S, Khan M, Shanechi A, Levy M, Izbudak I. double-blind, placebo-controlled, multicenter
MRI differences between MOG antibody disease study to evaluate the efficacy, safety,
and AQP4 NMOSD. Mult Scler Houndmills pharmacokinetics, and pharmacodynamics of
Basingstoke Engl 2020;26(14):1854-1865. satralizumab as monotherapy or in addition to
doi:10.1177/1352458519893093 baseline therapy in patients with myelin
oligodendrocyte glycoprotein
69 Sechi E, Krecke KN, Pittock SJ, et al. Frequency
antibody-associated disease (mogad)
and characteristics of MRI-negative myelitis
(NCT05271409). Updated October 26, 2023.
associated with MOG autoantibodies. Mult Scler
Accessed November 29, 2023. clinicaltrials.gov/
Houndmills Basingstoke Engl 2021;27(2):303-308.
study/NCT05271409
doi:10.1177/1352458520907900
196 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
79 Sechi E, Morris PP, McKeon A, et al. Glial fibrillary 91 Greenberg BM, Thomas KP, Krishnan C, et al.
acidic protein IgG related myelitis: Idiopathic transverse myelitis: corticosteroids,
characterisation and comparison with plasma exchange, or cyclophosphamide.
aquaporin-4-IgG myelitis. J Neurol Neurosurg Neurology 2007;68(19):1614-1617. doi:10.1212/
Psychiatry 2019;90(4):488-490. doi:10.1136/ 01.wnl.0000260970.63493.c8
jnnp-2018-318004
92 Berman M, Feldman S, Alter M, Zilber N, Kahana
80 Liu Z, Huang Q, Li H, et al. Glutamic acid E. Acute transverse myelitis: incidence and
decarboxylase antibody in a patient with etiologic considerations. Neurology 1981;31(8):
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
myelitis: a retrospective study. 966-971. doi:10.1212/wnl.31.8.966
Neuroimmunomodulation 2018;25(2):68-72.
93 Sadowsky CL, Becker D, Bosques G, et al.
doi:10.1159/000490530
Rehabilitation in transverse myelitis. Continuum
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
81 Hutchinson M, Waters P, McHugh J, et al. (Minneap Minn) 2011;17(4):816-830. doi:10.1212/
Progressive encephalomyelitis, rigidity, and 01.CON.0000403797.10612.d3
myoclonus: a novel glycine receptor antibody.
94 Bradshaw MJ, Pawate S, Koth LL, Cho TA,
Neurology 2008;71(16):1291-1292. doi:10.1212/
Gelfand JM. Neurosarcoidosis: pathophysiology,
01.wnl.0000327606.50322.f0
diagnosis, and treatment. Neurol Neuroimmunol
82 Woodhall M, Çoban A, Waters P, et al. Glycine Neuroinflammation 2021;8(6):e1084. doi:10.1212/
receptor and myelin oligodendrocyte NXI.0000000000001084
glycoprotein antibodies in Turkish patients with
95 Murphy OC, Salazar-Camelo A, Jimenez JA, et al.
neuromyelitis optica. J Neurol Sci 2013;335(1-2):
Clinical and MRI phenotypes of
221-223. doi:10.1016/j.jns.2013.08.034
sarcoidosis-associated myelopathy. Neurol
83 Chamard L, Magnin E, Berger E, et al. Stiff leg Neuroimmunol Neuroinflammation 2020;7(4):
syndrome and myelitis with anti-amphiphysin e722. doi:10.1212/NXI.0000000000000722
antibodies: a common physiopathology? Eur
96 Stern BJ, Royal W, Gelfand JM, et al. Definition
Neurol 2011;66(5):253-255. doi:10.1159/000331592
and consensus diagnostic criteria for
84 Faissner S, Lukas C, Reinacher-Schick A, et al. neurosarcoidosis: from the neurosarcoidosis
Amphiphysin-positive paraneoplastic myelitis consortium consensus group. JAMA Neurol 2018;
and stiff-person syndrome. Neurol 75(12):1546-1553. doi:10.1001/
Neuroimmunol Neuroinflammation 2016;3(6): jamaneurol.2018.2295
e285. doi:10.1212/NXI.0000000000000285
97 Ginat DT, Dhillon G, Almast J. Magnetic
85 Awad A, Stüve O. Idiopathic transverse myelitis resonance imaging of neurosarcoidosis. J Clin
and neuromyelitis optica: clinical profiles, Imaging Sci 2011;1:15. doi:10.4103/2156-7514.76693
pathophysiology and therapeutic choices.
98 Agnihotri SP, Singhal T, Stern BJ, Cho TA.
Curr Neuropharmacol 2011;9(3):417-428.
Neurosarcoidosis. Semin Neurol 2014;34(4):
doi:10.2174/157015911796557948
386-394. doi:10.1055/s-0034-1390387
86 Suchett-Kaye AI. Acute transverse myelitis
99 Fritz D, van de Beek D, Brouwer MC, Booij J.
complicating pneumonia; report of a case.
Whole-body 18F-FDG PET-CT in the diagnosis of
Lancet Lond Engl 1948;2(6524):417. doi:10.1016/
neurosarcoidosis. Mayo Clin Proc 2020;95(5):
s0140-6736(48)90987-8
1082-1084. doi:10.1016/j.mayocp.2020.01.032
87 Kerr DA, Ayetey H. Immunopathogenesis of
100 Khoury J, Wellik KE, Demaerschalk BM,
acute transverse myelitis. Curr Opin Neurol 2002;
Wingerchuk DM. Cerebrospinal fluid
15(3):339-347. doi:10.1097/00019052-200206000-
angiotensin-converting enzyme for diagnosis of
00019
central nervous system sarcoidosis. Neurologist
88 Voysey M, Clemens SAC, Madhi SA, et al. Safety 2009;15(2):108-111. doi:10.1097/NRL.
and efficacy of the ChAdOx1 nCoV-19 vaccine 0b013e31819bcf84
(AZD1222) against SARS-CoV-2: an interim
101 Dik WA, Heron M. Clinical significance of soluble
analysis of four randomised controlled trials in
interleukin-2 receptor measurement in
Brazil, South Africa, and the UK. Lancet Lond Engl
immune-mediated diseases. Neth J Med 2020;
2021;397(10269):99-111. doi:10.1016/S0140-6736(20)
78(5):220-231.
32661-1
102 Semenzato G, Cipriani A, Trentin L, et al. High
89 Naeem FN, Hasan SFS, Ram MD, et al. The
serum levels of soluble interleukin-2 receptors in
association between SARS-CoV-2 vaccines and
sarcoidosis. Sarcoidosis 1987;4(1):25-27.
transverse myelitis: a review. Ann Med Surg
2022;79:103870. doi:10.1016/j.amsu.2022.103870 103 Otto C, Wengert O, Unterwalder N, Meisel C,
Ruprecht K. Analysis of soluble interleukin-2
90 Román GC, Gracia F, Torres A, et al. Acute
receptor as CSF biomarker for neurosarcoidosis.
transverse myelitis (ATM): clinical review of 43
Neurol Neuroimmunol Neuroinflammation 2020;
Patients with COVID-19-associated ATM and 3
7(4):e725. doi:10.1212/NXI.0000000000000725
post-vaccination ATM serious adverse events
with the ChAdOx1 nCoV-19 vaccine (AZD1222). 104 Bagnato F, Stern BJ. Neurosarcoidosis: diagnosis,
Front Immunol 2021;12:653786. doi:10.3389/ therapy and biomarkers. Expert Rev Neurother
fimmu.2021.653786 2015;15(5):533-548. doi:10.1586/14737175.
2015.1037288
CONTINUUMJOURNAL.COM 197
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
IMMUNE-MEDIATED MYELOPATHIES
105 Fritz D, Timmermans WMC, van Laar JAM, et al. 109 Madhavan AA, Carr CM, Morris PP, et al. Imaging
Infliximab treatment in pathology-confirmed review of paraneoplastic neurologic syndromes.
neurosarcoidosis. Neurol Neuroimmunol AJNR Am J Neuroradiol 2020;41(12):2176-2187.
Neuroinflammation 2020;7(5):e847. doi:10.1212/ doi:10.3174/ajnr.A6815
NXI.0000000000000847
110 Nath U, Grant R. Neurological paraneoplastic
106 Wang A, Singh K, Ibrahim W, King B, Damsky W. syndromes. J Clin Pathol 1998;50:975-980.
The promise of JAK inhibitors for treatment of doi:10.1136/jcp.50.12.975
sarcoidosis and other inflammatory disorders
Downloaded from http://journals.lww.com/continuum by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCyw
111 Cai G, He D, Chu L, et al. Paraneoplastic
with macrophage activation: a review of the
neuromyelitis optica spectrum disorders:
literature. Yale J Biol Med 2020;93(1):187-195.
three new cases and a review of the literature.
107 Galli J, Greenlee J. Paraneoplastic diseases of the Int J Neurosci 2016;126(7):660-668.
CX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC1y0abggQZXdtwnfKZBYtws= on 02/16/2024
central nervous system. F1000Research 2020;9: doi:10.3109/00207454.2015.1054481
F1000 Faculty Rev-167. doi:10.12688/
112 Sepúlveda M, Sola-Valls N, Escudero D, et al.
f1000research.21309.1
Clinical profile of patients with paraneoplastic
108 Flanagan EP, McKeon A, Lennon VA, et al. neuromyelitis optica spectrum disorder and
Paraneoplastic isolated myelopathy: clinical aquaporin-4 antibodies. Mult Scler Houndmills
course and neuroimaging clues. Neurology 2011; Basingstoke Engl 2018;24(13):1753-1759.
76(24):2089-2095. doi:10.1212/ doi:10.1177/1352458517731914
WNL.0b013e31821f468f
198 F E B R U A R Y 2 0 24
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- Activity DesignDocument2 pagesActivity Designsanie50% (2)
- Biologic Therapies: What and When?: ReviewDocument10 pagesBiologic Therapies: What and When?: ReviewRameshKrishnanNo ratings yet
- Metabolic and Toxic Myelopathies.12Document25 pagesMetabolic and Toxic Myelopathies.12Mayra AldecoaNo ratings yet
- Microbiome Derived Metabolome As A PotenDocument3 pagesMicrobiome Derived Metabolome As A PotenJULIETANo ratings yet
- Central Nervous System Infections Complicating Immunosuppression and TransplantationDocument27 pagesCentral Nervous System Infections Complicating Immunosuppression and Transplantationnight.shadowNo ratings yet
- Eisenberg 2012Document13 pagesEisenberg 2012Juan G. Ovalles B.No ratings yet
- Blander 2018 Regulation of The Cell Biology of Antigen Cross PresentationDocument40 pagesBlander 2018 Regulation of The Cell Biology of Antigen Cross PresentationAntonellaNo ratings yet
- Infectious MyelopathiesDocument27 pagesInfectious MyelopathieseziojunionunesNo ratings yet
- 10 1056@NEJMra1911109 PDFDocument11 pages10 1056@NEJMra1911109 PDFMартин ДончевNo ratings yet
- Biomedical ScienceDocument8 pagesBiomedical ScienceBiology BảoNo ratings yet
- Guillain Barr Syndrome.5Document30 pagesGuillain Barr Syndrome.5Romina VillaseñorNo ratings yet
- ICI in OncologyDocument19 pagesICI in Oncologyraxi bacumabNo ratings yet
- Principles of Antimicrobial TherapyDocument12 pagesPrinciples of Antimicrobial TherapyAnne Abejuela ObialNo ratings yet
- (Mackay) Autoimmune Disease OverviewDocument11 pages(Mackay) Autoimmune Disease OverviewrodtobingNo ratings yet
- Advances in Potential Cerebrospinal Fluid Biomarkers For Autoimmune Encephalitis - A ReviewDocument13 pagesAdvances in Potential Cerebrospinal Fluid Biomarkers For Autoimmune Encephalitis - A ReviewAkila SwaminathanNo ratings yet
- Infectious Myelopathies.9Document27 pagesInfectious Myelopathies.9Mayra AldecoaNo ratings yet
- Neuromyelitis Optica Spectrum DIsorder and Other Non-Multiple Sclerosis Central Nervous System Inflammatory DIseasesDocument30 pagesNeuromyelitis Optica Spectrum DIsorder and Other Non-Multiple Sclerosis Central Nervous System Inflammatory DIseasesnight.shadow100% (1)
- Recombinant Peptide Subunit Vaccine Covid 19Document6 pagesRecombinant Peptide Subunit Vaccine Covid 19Marcelo Ricci UvinhaNo ratings yet
- Estrategias Inmunosupresivas de Tumores RabinovichDocument33 pagesEstrategias Inmunosupresivas de Tumores RabinovichLyanna StarkNo ratings yet
- Antimicrobial Drugs: Introduction To Antimicrobial Drugs. (N.D.) - WWW - Cyto.purdue - EduDocument2 pagesAntimicrobial Drugs: Introduction To Antimicrobial Drugs. (N.D.) - WWW - Cyto.purdue - EduAdeniyi AdebanjiNo ratings yet
- Inumnologia + MMDocument12 pagesInumnologia + MMLuis Bonino SanchezNo ratings yet
- Inflammatory Monocytes Suppression of Vaccine Immunity By: References Cites 51 ArticlesDocument11 pagesInflammatory Monocytes Suppression of Vaccine Immunity By: References Cites 51 Articlesthh uuNo ratings yet
- Reumatologia y NeurologiaDocument31 pagesReumatologia y NeurologiaRonald Valverde RodriguezNo ratings yet
- Muscle and Nerve - 2023 - Claytor - Myasthenic Crisis BESTDocument12 pagesMuscle and Nerve - 2023 - Claytor - Myasthenic Crisis BESTAdreanNo ratings yet
- Braun Wald 2008Document12 pagesBraun Wald 2008MedranoReyesLuisinNo ratings yet
- Jaggu 9b01579Document12 pagesJaggu 9b01579Jagjeet GujralNo ratings yet
- Pengembangan Formula Liposom Kationik Sebagai Sistem Penghantaran VaksinDocument49 pagesPengembangan Formula Liposom Kationik Sebagai Sistem Penghantaran VaksinRifqah Haq ArulaNo ratings yet
- Mitochondrial Disease and Anesthesia: Vincent C. Hsieh, MD, Elliot J. Krane, MD, and Philip G. Morgan, MDDocument5 pagesMitochondrial Disease and Anesthesia: Vincent C. Hsieh, MD, Elliot J. Krane, MD, and Philip G. Morgan, MDJZNo ratings yet
- VOL 68, NO I July 1986: The Society Ournal of of HematologyDocument31 pagesVOL 68, NO I July 1986: The Society Ournal of of HematologyNurma FauziahNo ratings yet
- Antibodies The Bodys Defence WarriorsDocument9 pagesAntibodies The Bodys Defence WarriorssarahhannahghanyNo ratings yet
- Pi Is 0025619616308187Document13 pagesPi Is 0025619616308187Anthony M CaballeroNo ratings yet
- Journal 1Document12 pagesJournal 1Angela NataliaNo ratings yet
- Pharmacokinetics and Pharmacodynamics of Antibacterial Agents PDFDocument29 pagesPharmacokinetics and Pharmacodynamics of Antibacterial Agents PDFarmitadewiNo ratings yet
- Vaccines 10 01681 v2Document8 pagesVaccines 10 01681 v2Wesley BrittoNo ratings yet
- ART Action and Resistance Mechanisms of Antibiotics A Guide For CliniciansDocument16 pagesART Action and Resistance Mechanisms of Antibiotics A Guide For CliniciansHECTORIBZAN ACERO SANDOVALNo ratings yet
- Fimmu 12 806560Document9 pagesFimmu 12 806560Orfa Esther Barrios PazosNo ratings yet
- Research Guide: Improve Immunity in Clinical PracticeDocument8 pagesResearch Guide: Improve Immunity in Clinical PracticeNacer BechouNo ratings yet
- Wjco 12 712Document14 pagesWjco 12 712ovatanaNo ratings yet
- Review Beta GlucansDocument11 pagesReview Beta GlucansAyman YounesNo ratings yet
- General Principles of Antibiotic Resistance in BacteriaDocument7 pagesGeneral Principles of Antibiotic Resistance in BacteriaAdeela ZahidNo ratings yet
- Holtzman 2014Document13 pagesHoltzman 2014andikaprtmNo ratings yet
- Harnessing B Cell Responses For Personalized Approaches in HIV ManagementDocument15 pagesHarnessing B Cell Responses For Personalized Approaches in HIV ManagementKIU PUBLICATION AND EXTENSIONNo ratings yet
- Vaccines: Wim Jiskoot, Gideon F. A. Kersten, Enrico Mastrobattista, and Bram SlütterDocument24 pagesVaccines: Wim Jiskoot, Gideon F. A. Kersten, Enrico Mastrobattista, and Bram SlütterSaritaJQM100% (1)
- Objetivo 3 Móvil PDFDocument26 pagesObjetivo 3 Móvil PDFnawal akarmaniNo ratings yet
- Supplementary Lecture - Vaccine 101Document11 pagesSupplementary Lecture - Vaccine 101KarizzaNo ratings yet
- Crisis MiastenicaDocument12 pagesCrisis MiastenicaOsvaldo CortésNo ratings yet
- Cancer Immunotherapy Beyond Checkpoint BlockadeDocument16 pagesCancer Immunotherapy Beyond Checkpoint Blockaderaxi bacumabNo ratings yet
- (PHA) 2.13 Immunopharmacology - Dr. Marbella PDFDocument10 pages(PHA) 2.13 Immunopharmacology - Dr. Marbella PDFpasambalyrradjohndarNo ratings yet
- 1 s2.0 S1896112622000062 MainDocument10 pages1 s2.0 S1896112622000062 MainRonWuNo ratings yet
- Immunogenic Cell Death in Cancer Review 2019Document12 pagesImmunogenic Cell Death in Cancer Review 2019Kudelko MatNo ratings yet
- Addressing Symptom Burden in Myeloproliferative NeoplasmsDocument10 pagesAddressing Symptom Burden in Myeloproliferative Neoplasmsshaza elkourashyNo ratings yet
- Celulas MadresDocument10 pagesCelulas MadresDIOGENESNo ratings yet
- PARANEOPLASTICDocument8 pagesPARANEOPLASTICMuhammad Imran MirzaNo ratings yet
- Monoclonal Antibodies: Molecular Pathology June 2000Document8 pagesMonoclonal Antibodies: Molecular Pathology June 2000AnasNo ratings yet
- Feb 2011 Immusan TexexecsummaryDocument2 pagesFeb 2011 Immusan TexexecsummaryIonescu RaduNo ratings yet
- Systemic Autoinflamatory DiseaseDocument10 pagesSystemic Autoinflamatory DiseaseJair Alexander Quintero PanucoNo ratings yet
- Biomedicines: Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsDocument23 pagesBiomedicines: Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsAlfian_Dwi_SNo ratings yet
- Medical Hierarchy - NEJMDocument4 pagesMedical Hierarchy - NEJMXyzNo ratings yet
- Ru Ella 2013Document25 pagesRu Ella 2013Ruben NatarîșNo ratings yet
- Ansaldo Et Al 2021 Control of Immunity by The MicrobiotaDocument34 pagesAnsaldo Et Al 2021 Control of Immunity by The MicrobiotawalidNo ratings yet
- Immunotherapeutic Strategies for the Treatment of GliomaFrom EverandImmunotherapeutic Strategies for the Treatment of GliomaNo ratings yet
- Fneur 12 706169Document14 pagesFneur 12 706169Mayra AldecoaNo ratings yet
- Writing 8 L10Document1 pageWriting 8 L10Mayra AldecoaNo ratings yet
- Writing 7 L10Document1 pageWriting 7 L10Mayra AldecoaNo ratings yet
- Writing 8Document1 pageWriting 8Mayra AldecoaNo ratings yet
- Guptautkarsh@dsnlu Ac inDocument2 pagesGuptautkarsh@dsnlu Ac inUTKARSH GUPTANo ratings yet
- Personal Hygiene: Tve-ExploratoryDocument3 pagesPersonal Hygiene: Tve-ExploratoryPoseidon NipNo ratings yet
- 2016-06-02 Map Re SVEC PCB Ballasts, Primary ContaminationDocument1 page2016-06-02 Map Re SVEC PCB Ballasts, Primary ContaminationLynsiNo ratings yet
- Association Between Polymorphisms of OCT1 and Metabolic Response To Metformin in Women With Polycystic Ovary Syndrome.Document10 pagesAssociation Between Polymorphisms of OCT1 and Metabolic Response To Metformin in Women With Polycystic Ovary Syndrome.Fahmi SidiqNo ratings yet
- Geofrey R. Watt - Calvin S Geneva Confronts Magic and Witchcraft The Evidence From The ConsistoryDocument31 pagesGeofrey R. Watt - Calvin S Geneva Confronts Magic and Witchcraft The Evidence From The ConsistoryMilica KovacevicNo ratings yet
- RESEARCH THESIS (IZAZ Khan)Document51 pagesRESEARCH THESIS (IZAZ Khan)Izaz KhanNo ratings yet
- Daftar Obat Floorstock RuanganDocument3 pagesDaftar Obat Floorstock Ruangandini mahdianiNo ratings yet
- 04-25-13 EditionDocument36 pages04-25-13 EditionSan Mateo Daily JournalNo ratings yet
- Medication Dialogue: Obs. in Loc de How Are You Feeling?", Putem Folosi How Do You Feel?", Fara Sa SchimbamDocument4 pagesMedication Dialogue: Obs. in Loc de How Are You Feeling?", Putem Folosi How Do You Feel?", Fara Sa SchimbamToma GeorgianaaNo ratings yet
- BOGNADocument198 pagesBOGNAjustingollosossuNo ratings yet
- Mobility, Stability and MovementDocument62 pagesMobility, Stability and MovementYuldashNo ratings yet
- Biotechnology Safety Law enDocument40 pagesBiotechnology Safety Law enSunnyNo ratings yet
- Exp 13N s18 Radioactivity FVDocument13 pagesExp 13N s18 Radioactivity FVAdnan SheraziNo ratings yet
- SUMMATIVE TEST QUARTER 3 Week 3Document2 pagesSUMMATIVE TEST QUARTER 3 Week 3Mary CrisNo ratings yet
- A Clinical Guide To Orthodontics - J. Sandy (2004) WW PDFDocument77 pagesA Clinical Guide To Orthodontics - J. Sandy (2004) WW PDFAntonela CeremușNo ratings yet
- Baaleman 2021 CHP - 10.1007 - 978 3 030 80068 0 - 21 Ver PDFDocument26 pagesBaaleman 2021 CHP - 10.1007 - 978 3 030 80068 0 - 21 Ver PDFcLAUDIANo ratings yet
- Motivational Interviewing: Engagement and AssessmentDocument31 pagesMotivational Interviewing: Engagement and AssessmenttakemebrickNo ratings yet
- Synopsis-Brain TumourDocument9 pagesSynopsis-Brain TumourKomalNo ratings yet
- Katkat File AP 10Document2 pagesKatkat File AP 10Cathlene TanNo ratings yet
- Lymphocytic LeukemiaDocument6 pagesLymphocytic Leukemiaル シリ100% (1)
- Gurley, Bill J, - Clinically Relevant Herb Mineral Vitamin IntrxnDocument9 pagesGurley, Bill J, - Clinically Relevant Herb Mineral Vitamin IntrxnMSKCNo ratings yet
- ოქსფორდის სახელმძღვანელო ფსიქიატრიაში 4Document9 pagesოქსფორდის სახელმძღვანელო ფსიქიატრიაში 4a.utiashviliNo ratings yet
- INTRO-TO-ANATOMY - PHYSIOLOGY LectureDocument30 pagesINTRO-TO-ANATOMY - PHYSIOLOGY LectureJulie anne De jesusNo ratings yet
- Brosur Jackson ReesDocument8 pagesBrosur Jackson ReesAnonymous tbJ24554No ratings yet
- 153 - 158 - 23 - PDF 2023 Jun 20 16 51 8Document17 pages153 - 158 - 23 - PDF 2023 Jun 20 16 51 8harshNo ratings yet
- Diagnosis and Management of Tremor.11Document16 pagesDiagnosis and Management of Tremor.11Stephanie Queiroz Dos SantosNo ratings yet
- UWORLD Notes by Subject Main Division Usmle GrassrootsDocument80 pagesUWORLD Notes by Subject Main Division Usmle Grassrootsnashra bukhariNo ratings yet
- Site Mobilzation PlanDocument18 pagesSite Mobilzation PlanRAMY ABOU AL DAHABNo ratings yet
- Vet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THEDocument7 pagesVet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THECésar Sa JimNo ratings yet