Download as pdf or txt
You might also like
- Sample Community Pharmacy Intern Training PlanDocument20 pagesSample Community Pharmacy Intern Training PlanAmatou ASSAMII EL HADRAOUINo ratings yet
- NNF 2ndDocument235 pagesNNF 2ndRuDy RaviNo ratings yet
- Depot Antipsychotic Medication Guidelines - PHA04 - February 2020 - 0Document29 pagesDepot Antipsychotic Medication Guidelines - PHA04 - February 2020 - 0Obinna AnozieNo ratings yet
- Patient Controlled Analgesia (PCA) : Pat/Mm 7Document15 pagesPatient Controlled Analgesia (PCA) : Pat/Mm 7kaiyeung0818No ratings yet
- Benzodiazepine and Hypnotic Guidelines (V1.0 July 2010)Document18 pagesBenzodiazepine and Hypnotic Guidelines (V1.0 July 2010)Deza IngridNo ratings yet
- Final Approved Guidelines For The Drug Treatment of Pain in Primary Care Version 50 1494493393Document15 pagesFinal Approved Guidelines For The Drug Treatment of Pain in Primary Care Version 50 1494493393zebun nahar BushraNo ratings yet
- Rapid TranquillisationDocument42 pagesRapid TranquillisationAnubhav NaikNo ratings yet
- Final Benzodiazepine Guidelines Version 23 1495194854Document18 pagesFinal Benzodiazepine Guidelines Version 23 1495194854Kru PrimeNo ratings yet
- Prescribing Psychotropics: Perspective From Telepsychiatry Operational Guidelines 2020Document5 pagesPrescribing Psychotropics: Perspective From Telepsychiatry Operational Guidelines 2020ika nurul shofiyahNo ratings yet
- Anxiety Disorder Prescribing Guidelines - PHA49 - May 2022Document28 pagesAnxiety Disorder Prescribing Guidelines - PHA49 - May 2022Iza D.No ratings yet
- Administration of Medicines SOP v3.0Document13 pagesAdministration of Medicines SOP v3.0Ani RahimNo ratings yet
- Pro Re Nata (PRN) Medication: PurposeDocument4 pagesPro Re Nata (PRN) Medication: PurposeF̳̿a̳̿l̳̿a̳̿h̳̿ Opcional S̳̿u̳̿d̳̿i̳̿r̳̿a̳̿d̳̿i̳̿r̳̿e̳̿j̳̿a̳̿No ratings yet
- NHS Rapid Tranquillisation PolicyDocument49 pagesNHS Rapid Tranquillisation PolicyUrgencias HorwitzNo ratings yet
- PSI and Medical Council Joint GuidanceDocument22 pagesPSI and Medical Council Joint GuidanceIrina FloreaNo ratings yet
- 1.1.1.4 Sedation PolicyDocument34 pages1.1.1.4 Sedation PolicyNguyen Duy ThanhNo ratings yet
- 1.4 CNS Drugs - Sedatives and Hypnotics - Dr. Rani Qasem 2014-2015Document23 pages1.4 CNS Drugs - Sedatives and Hypnotics - Dr. Rani Qasem 2014-2015Faisal FahadNo ratings yet
- Pharmacologic Management of Neuropathic Pain ENGverDocument138 pagesPharmacologic Management of Neuropathic Pain ENGvermagreaNo ratings yet
- nhsgvancDocument17 pagesnhsgvanchisonamikaze2No ratings yet
- Antipsychotic Guidelines Version 3.2 - Oct 15 - With New Hdat Form Added - Dec 16 0 PDFDocument61 pagesAntipsychotic Guidelines Version 3.2 - Oct 15 - With New Hdat Form Added - Dec 16 0 PDFIoana IoanaNo ratings yet
- An Off-Label Guide To Gabapentin 2022-01-31 CARLAT PUBLISHINGDocument1 pageAn Off-Label Guide To Gabapentin 2022-01-31 CARLAT PUBLISHINGLee ThompsonNo ratings yet
- Inada, 2015Document8 pagesInada, 2015Khumaira SantaNo ratings yet
- Esketamine PSD July 2022Document54 pagesEsketamine PSD July 2022aarons1012000No ratings yet
- Laai Guidelines - v5 - 0118 0 PDFDocument27 pagesLaai Guidelines - v5 - 0118 0 PDFadam lawrence100% (1)
- Pharmacologic Management of Chronic Neuropathic Pain: Clinical ReviewDocument9 pagesPharmacologic Management of Chronic Neuropathic Pain: Clinical ReviewOdi P JayaNo ratings yet
- Diazepam Understanding The Pharmacokinetics of Anxiolytic DrugsDocument19 pagesDiazepam Understanding The Pharmacokinetics of Anxiolytic DrugsFarros ibrahimNo ratings yet
- Prescription Trends of Antidepressants. What Are We Doing & What Else Is Required?Document8 pagesPrescription Trends of Antidepressants. What Are We Doing & What Else Is Required?happy_atworkNo ratings yet
- Naloxone in AdultsDocument8 pagesNaloxone in AdultsRoboschi StefaniaNo ratings yet
- Pharmacology BookDocument332 pagesPharmacology BookKenneth DayritNo ratings yet
- Hypnotic and Anxiolytic Reduction or Withdrawal ResourcesDocument28 pagesHypnotic and Anxiolytic Reduction or Withdrawal ResourcesbarakaNo ratings yet
- Antipsychotic Polypharmacy in Psychotic DisorderDocument10 pagesAntipsychotic Polypharmacy in Psychotic DisorderFiarry FikarisNo ratings yet
- GBSDocument50 pagesGBSDanik Mahfirotul HayatiNo ratings yet
- Benzodiazepine and Z Hypnotic Prescribing GuidanceDocument11 pagesBenzodiazepine and Z Hypnotic Prescribing GuidanceKru PrimeNo ratings yet
- Psychotherapy: DepressionDocument8 pagesPsychotherapy: DepressionkerfunkerNo ratings yet
- ECDD 37th Report FINAL PrelayoutDocument45 pagesECDD 37th Report FINAL PrelayoutsppNo ratings yet
- 4462MC Rev HSS-Q5401 Pharmacy-Assistant 25-07-2017 PDFDocument27 pages4462MC Rev HSS-Q5401 Pharmacy-Assistant 25-07-2017 PDFSauraj GautamNo ratings yet
- FARM Notes: A Systematic Review: Pharma Times July 2019Document3 pagesFARM Notes: A Systematic Review: Pharma Times July 2019Syed Qasim MehmoodNo ratings yet
- Treating Panic DisordersDocument16 pagesTreating Panic DisorderspatriaindraNo ratings yet
- Neuropharmacology: Danielle Larson, Tanya SimuniDocument6 pagesNeuropharmacology: Danielle Larson, Tanya SimunigustavoNo ratings yet
- Trombopenie Polycythemie expertReviewsHemat2014Document11 pagesTrombopenie Polycythemie expertReviewsHemat2014salamredNo ratings yet
- Clinical Skills For Pharmacists-APatient-FocusedApproach3rdeditionDocument13 pagesClinical Skills For Pharmacists-APatient-FocusedApproach3rdeditionNADYA FEBRIYANTINo ratings yet
- Medi-100-E27653Document7 pagesMedi-100-E27653Rika TriwardianiNo ratings yet
- Antipsychotic Prescribing GuidelineDocument26 pagesAntipsychotic Prescribing GuidelineAshraf MullaNo ratings yet
- Farmaco AnsiDocument10 pagesFarmaco AnsiYakelin VillanuevaNo ratings yet
- Document ControlDocument20 pagesDocument Controldoctor uroosaNo ratings yet
- Psychotherapy Plus Antidepressant For Panic Disorder With or Without Agoraphobia Systematic ReviewDocument8 pagesPsychotherapy Plus Antidepressant For Panic Disorder With or Without Agoraphobia Systematic ReviewRizky AmNo ratings yet
- Introduction, Medicines Classification and Standard Operating ProceduresDocument14 pagesIntroduction, Medicines Classification and Standard Operating ProceduresAnkur SinghNo ratings yet
- 1047-PPP66 Policy Guide SROMDocument13 pages1047-PPP66 Policy Guide SROMWael BebawyNo ratings yet
- Uritsky 2018Document7 pagesUritsky 2018Sheena Mae MansinadesNo ratings yet
- Comment: Lancet Neurol 2020Document2 pagesComment: Lancet Neurol 2020dhea nadhiaNo ratings yet
- 2021 1.0 Medicines Procedure 28 LAI ProcedureDocument33 pages2021 1.0 Medicines Procedure 28 LAI ProcedureFazal ShahNo ratings yet
- Rational Drug Use (Rdu) - Clin Pharma - IDocument3 pagesRational Drug Use (Rdu) - Clin Pharma - IKandysse de OcampoNo ratings yet
- The Pharmacopeia Internationalis or International Pharmacopeia (Ip)Document2 pagesThe Pharmacopeia Internationalis or International Pharmacopeia (Ip)Farhana DalandasNo ratings yet
- MOH CPG - Prescribing of BenzodiazepinesDocument67 pagesMOH CPG - Prescribing of BenzodiazepinesthefrankoneNo ratings yet
- Parmar Et Al 2023 National List of Essential Medicines 2022 of India Perspectives From PsychiatristsDocument4 pagesParmar Et Al 2023 National List of Essential Medicines 2022 of India Perspectives From PsychiatristsonamreNo ratings yet
- Glutamato My Gaba en AnsuedadDocument17 pagesGlutamato My Gaba en AnsuedadGerardo TellezNo ratings yet
- Jurnal Jiwa 2Document18 pagesJurnal Jiwa 2Yolanda Karoline PasaribuNo ratings yet
- A Practical Guide To Pain Management IV ChildrenDocument13 pagesA Practical Guide To Pain Management IV Childrenfuka priesleyNo ratings yet
- Use of Antipsychotic Depot and Long Acting Injections Lai Dec 2021Document25 pagesUse of Antipsychotic Depot and Long Acting Injections Lai Dec 2021Diego HormacheaNo ratings yet
- Triptans and Migraine: Advances in Use, Administration, Formulation, and DevelopmentDocument35 pagesTriptans and Migraine: Advances in Use, Administration, Formulation, and DevelopmentMartin GiraudoNo ratings yet
- Principles of CNS Drug Development: From Test Tube to Clinic and BeyondFrom EverandPrinciples of CNS Drug Development: From Test Tube to Clinic and BeyondNo ratings yet
- Agrirobot PDFDocument103 pagesAgrirobot PDFMuhamad Azlan ShahNo ratings yet
- Marketing Plan: GoldilocksDocument18 pagesMarketing Plan: GoldilocksAkhia Visitacion100% (1)
- RC Depron F 35Document25 pagesRC Depron F 35pccdtkNo ratings yet
- Voslp /F 38: Overcenter ValvesDocument2 pagesVoslp /F 38: Overcenter ValvesSachin RamadasanNo ratings yet
- Wizard - School of DiabolismDocument1 pageWizard - School of DiabolismHope LaneNo ratings yet
- User ConsentDocument3 pagesUser ConsentvikuvishnuvikuNo ratings yet
- Price ScheduleDocument10 pagesPrice ScheduleRen SalazarNo ratings yet
- Advanced Baking 1Document61 pagesAdvanced Baking 1Judelmae SisonNo ratings yet
- 6º Ano Ingles Unit4 Test3Document3 pages6º Ano Ingles Unit4 Test3Paula Lopes100% (1)
- NI-Predictive Maintenance and Machine Health MonitoringDocument34 pagesNI-Predictive Maintenance and Machine Health Monitoringtườngt_14No ratings yet
- Full Download Elementary Statistics A Step by Step Approach Bluman 9Th Edition Solutions Manual PDFDocument49 pagesFull Download Elementary Statistics A Step by Step Approach Bluman 9Th Edition Solutions Manual PDFsteven.engelke246100% (21)
- Section 2 Digital OutputDocument1 pageSection 2 Digital Outputsamim_khNo ratings yet
- 03 - Rise of The Allies 1Document41 pages03 - Rise of The Allies 1evanpate0No ratings yet
- PS2 VGA Diagram Rev by GillBert - Rev2 PDFDocument6 pagesPS2 VGA Diagram Rev by GillBert - Rev2 PDFwuemuraNo ratings yet
- HBS Assessment Feedback Form IndividualDocument1 pageHBS Assessment Feedback Form IndividualsarithaNo ratings yet
- Solar Power PlantDocument23 pagesSolar Power Plantmadhu_bedi12No ratings yet
- GMP Checklist Sanitary Facilities and ControlsDocument1 pageGMP Checklist Sanitary Facilities and ControlsATSEDENo ratings yet
- Principles of Electricity PDFDocument371 pagesPrinciples of Electricity PDFJohn C. Stephens100% (5)
- CA Empanelment-Application FormatDocument5 pagesCA Empanelment-Application FormatPV REDDY AssociatesNo ratings yet
- Lewis Dot Structures #1Document3 pagesLewis Dot Structures #1Dustin MoenchNo ratings yet
- The Outlaw (1871)Document21 pagesThe Outlaw (1871)ViannisoNo ratings yet
- 1700 N Manhattan Ave - Royal Towers - Notice of CondemnationDocument14 pages1700 N Manhattan Ave - Royal Towers - Notice of CondemnationMatthew SelfNo ratings yet
- Spa Music 10 SLM3 q1Document21 pagesSpa Music 10 SLM3 q1Noldan King FranciscoNo ratings yet
- Serial AcquirersDocument54 pagesSerial AcquirersArturo OrtegaNo ratings yet
- Bullock Cart: Aarushree KhobragadeDocument13 pagesBullock Cart: Aarushree KhobragadeAzure MidoriyaNo ratings yet
- 65018-1A - Rev 0 - QSF 75 65018-1A Parts ManualDocument52 pages65018-1A - Rev 0 - QSF 75 65018-1A Parts Manualandrei20041No ratings yet
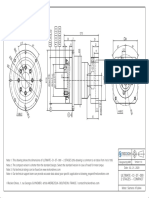
- ULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Document1 pageULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Francesco SchioppaNo ratings yet
- Christopher MontoyaDocument1 pageChristopher MontoyaUF Student GovernmentNo ratings yet
- Sales and Purchases 2021-22Document15 pagesSales and Purchases 2021-22Vamsi ShettyNo ratings yet
- Erco Complete Catalogue 2019 en PDFDocument1,280 pagesErco Complete Catalogue 2019 en PDFarmadityaNo ratings yet