Download as docx, pdf, or txt
You might also like
- Heart Failure Nursing Care Management - A Study GuideDocument16 pagesHeart Failure Nursing Care Management - A Study GuideJOSHUA DICHOSONo ratings yet
- Heart Failure 2011 SVDocument74 pagesHeart Failure 2011 SVtoobstudyingNo ratings yet
- A 07 IccDocument17 pagesA 07 IccJorge CotrinaNo ratings yet
- CHF Left SidedDocument21 pagesCHF Left SidedSandie Daniel GabalunosNo ratings yet
- Cardiovascular Diseases Management Amp Nursing CareDocument76 pagesCardiovascular Diseases Management Amp Nursing CareAlberto MeroNo ratings yet
- Congestive Heart Failure OverviewDocument12 pagesCongestive Heart Failure OverviewkazelleNo ratings yet
- Cad - Coronary Artery Disease & Myocardial InfarctionDocument6 pagesCad - Coronary Artery Disease & Myocardial Infarctionmaulikmd21No ratings yet
- Case Presentation For ClassDocument59 pagesCase Presentation For ClassMuhammad HarisNo ratings yet
- Clinical Symptoms Due To Fluid CongestionDocument6 pagesClinical Symptoms Due To Fluid CongestionedenpearlcastilloNo ratings yet
- Kurmabekov Ilim: The Heart: Anatomy, Physiology, and Functi OnDocument16 pagesKurmabekov Ilim: The Heart: Anatomy, Physiology, and Functi OnILIM KURMANBEKOVNo ratings yet
- Cardio Vascular DiseasesDocument34 pagesCardio Vascular DiseasesSam ParkNo ratings yet
- Case 27 (LC Fix)Document14 pagesCase 27 (LC Fix)galih suharno0% (1)
- Congestive Heart Failure - Left Vs Right Side Uncategorized: DoublesDocument8 pagesCongestive Heart Failure - Left Vs Right Side Uncategorized: DoublesWeng Ramojal0% (1)
- Nursing Care Plan For Acyanotic Heart DiseaseDocument55 pagesNursing Care Plan For Acyanotic Heart DiseaseDeepikaxena John79% (14)
- Non-St Segment Elevation Myocardial Infarction (Nstemi)Document24 pagesNon-St Segment Elevation Myocardial Infarction (Nstemi)MHIEMHOINo ratings yet
- HCVD KoDocument10 pagesHCVD KoMarianne BaquilalaNo ratings yet
- Case Presentation On "Congestive Heart Failure" General ObjectiveDocument7 pagesCase Presentation On "Congestive Heart Failure" General ObjectiveLorlaine Quilitano PeñarandaNo ratings yet
- CHF ReportDocument16 pagesCHF ReportCristina L. JaysonNo ratings yet
- Case StudyDocument4 pagesCase StudyDaniel Angelo ArangoNo ratings yet
- 0 No Musc. Contrac'n, 1-Visible Musc. Con W/no or Trace Movement, 2-Limb Movmnt But Not AgaistDocument7 pages0 No Musc. Contrac'n, 1-Visible Musc. Con W/no or Trace Movement, 2-Limb Movmnt But Not AgaistGirlie TeruelNo ratings yet
- The Heart-1Document30 pagesThe Heart-1Ebuka AniNo ratings yet
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- Psychology PsychopathologyDocument15 pagesPsychology Psychopathologykunalpandey704921No ratings yet
- Materi TM 1Document3 pagesMateri TM 1leny cahyani putriNo ratings yet
- Heart FailureDocument13 pagesHeart Failuremildred alidon100% (2)
- Heart Failure inDocument11 pagesHeart Failure inastro1211No ratings yet
- Congestive Heart FailureDocument64 pagesCongestive Heart FailureBentoys StreetNo ratings yet
- Acute Heart FailureDocument13 pagesAcute Heart FailureffuNo ratings yet
- MM M M MDocument20 pagesMM M M MAshok KumarNo ratings yet
- Congestive Heart Failure FinalxxxxDocument12 pagesCongestive Heart Failure FinalxxxxDoneva Lyn MedinaNo ratings yet
- Coronary Heart Disease High Blood Pressure DiabetesDocument2 pagesCoronary Heart Disease High Blood Pressure DiabetesrichardiaNo ratings yet
- OXY-Cardio Care ManagementDocument114 pagesOXY-Cardio Care Managementlalaine22daleNo ratings yet
- Heart FailureDocument16 pagesHeart FailureLillabinNo ratings yet
- Cardiovascular DiseasesDocument52 pagesCardiovascular DiseasesAMAN KUMAR JHANo ratings yet
- Congestive Heart FailureDocument13 pagesCongestive Heart FailureryanmoreNo ratings yet
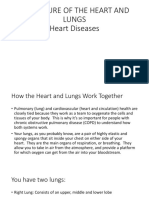
- Procedure of The Heart and Lungs Heart DiseasesDocument19 pagesProcedure of The Heart and Lungs Heart DiseasesKristin ArgosinoNo ratings yet
- Heart Failure: Lungu Adelina Anul II BDocument10 pagesHeart Failure: Lungu Adelina Anul II BLungu AdelinaNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart FailureBella Trix PagdangananNo ratings yet
- Heart Failure: A Case AnalysisDocument14 pagesHeart Failure: A Case AnalysisBrix ValdrizNo ratings yet
- CHFDocument61 pagesCHFAngeline Lareza-Reyna VillasorNo ratings yet
- Prevention: Blood Pressure Body Weight Here BMIDocument8 pagesPrevention: Blood Pressure Body Weight Here BMILuthfi Rama MaulanaNo ratings yet
- H FDocument23 pagesH FSaihmingliani SailoNo ratings yet
- Heart Failure ?Document4 pagesHeart Failure ?kilodan16No ratings yet
- A Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and MidwiferyDocument13 pagesA Case Study of Hypertensive Cardiovascular Disease (HCVD) : School of Nursing and Midwiferyhsiria100% (2)
- 07 - 01 - Assessment of Cardiovascular SystemDocument55 pages07 - 01 - Assessment of Cardiovascular SystemSalman Habeeb50% (2)
- Cardiovascular Disease Case StudyDocument8 pagesCardiovascular Disease Case StudyAbigail BascoNo ratings yet
- Congestive Heart Failure: Jeffrey Navarro Rojas, R.N., R.M., M.N. Clinical Instructor University of HailDocument12 pagesCongestive Heart Failure: Jeffrey Navarro Rojas, R.N., R.M., M.N. Clinical Instructor University of Hailjeffrey_rojasNo ratings yet
- Case Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDocument7 pagesCase Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDaniel Angelo ArangoNo ratings yet
- Heart PresentationDocument20 pagesHeart PresentationAni KvaratskheliaNo ratings yet
- Congenital Heart Disease Is One or More Problems With The Heart's Structure ThatDocument37 pagesCongenital Heart Disease Is One or More Problems With The Heart's Structure Thatneelimawanker chinnariNo ratings yet
- Congestive Heart Failure (CHF) : BY Miss. S. D. Ajetrao Assistant Professor ADCDP, AshtaDocument16 pagesCongestive Heart Failure (CHF) : BY Miss. S. D. Ajetrao Assistant Professor ADCDP, AshtaChandraprakash JadhavNo ratings yet
- Case Study PPT Patho NLNGDocument36 pagesCase Study PPT Patho NLNGKate ChavezNo ratings yet
- Natural Treatments for Heart Diseases: Through Medicinal Alkaline Herbs, Diets, & Aerobic Physiotherapy that Boost Natural Immunity; Detoxification & Prevent Infections, Inflammation & Cardiac ArrestFrom EverandNatural Treatments for Heart Diseases: Through Medicinal Alkaline Herbs, Diets, & Aerobic Physiotherapy that Boost Natural Immunity; Detoxification & Prevent Infections, Inflammation & Cardiac ArrestNo ratings yet
- As SNAB Revision NotesDocument49 pagesAs SNAB Revision NotesawinterqueenNo ratings yet
- CCF and Dementia Complete-1Document24 pagesCCF and Dementia Complete-1Agboola SeyiNo ratings yet
- Case Study (Assessing Heart and Neck Vessels)Document3 pagesCase Study (Assessing Heart and Neck Vessels)Claire LibatNo ratings yet
- Infas Ci Cardio Vasculary Syst 2022Document7 pagesInfas Ci Cardio Vasculary Syst 2022YAO CESAR KOFFINo ratings yet
- The Circulatory SystemDocument25 pagesThe Circulatory SystemEduardson PHNo ratings yet
- Cardiovascular System: Presented byDocument76 pagesCardiovascular System: Presented bySoma Al-mutairiNo ratings yet
- Reverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)From EverandReverse and Prevent Heart Disease: Natural Ways to Stop and Prevent Heart Disease, Using Plant-Based Oil-Free Diets (Cure Congestive Heart Failure)No ratings yet
- Electronic Health RecordsDocument13 pagesElectronic Health RecordsZechariah NicholasNo ratings yet
- CATHETERIZATIONDocument18 pagesCATHETERIZATIONZechariah NicholasNo ratings yet
- Midbm3106 Complex Midwifery PracticeDocument4 pagesMidbm3106 Complex Midwifery PracticeZechariah NicholasNo ratings yet
- Mal PresentationDocument19 pagesMal PresentationZechariah NicholasNo ratings yet
- Guidelines For Management of Leprosy - PRINT VeersionDocument53 pagesGuidelines For Management of Leprosy - PRINT VeersionZechariah NicholasNo ratings yet
- Fore ArmDocument3 pagesFore ArmZechariah NicholasNo ratings yet
- Drug AddictionDocument7 pagesDrug AddictionZechariah NicholasNo ratings yet
- Case Study of Patient With Tuberculosis EditedDocument14 pagesCase Study of Patient With Tuberculosis EditedZechariah NicholasNo ratings yet
- Muscle TissueDocument2 pagesMuscle TissueZechariah NicholasNo ratings yet
- Cell MembraneDocument7 pagesCell MembraneZechariah NicholasNo ratings yet
- Breast EngorgementDocument15 pagesBreast EngorgementZechariah NicholasNo ratings yet
- 2012 MitraClip For The Treatment of Mitral RegurgitationDocument11 pages2012 MitraClip For The Treatment of Mitral RegurgitationThanh BinhNo ratings yet
- Cor PulmonaleDocument21 pagesCor Pulmonalemaibejose100% (1)
- Clinical Application of Pulsatility Index: Review ArticleDocument10 pagesClinical Application of Pulsatility Index: Review ArticleMayNo ratings yet
- Hemodynamic response to β-blockers in severe sepsis and septic shock: A review of current literatureDocument6 pagesHemodynamic response to β-blockers in severe sepsis and septic shock: A review of current literatureIris AszalosNo ratings yet
- Human Body DR MellaliDocument20 pagesHuman Body DR MellaliSarah MellaliNo ratings yet
- Sentance ArrangementDocument43 pagesSentance ArrangementRabendraSharmaNo ratings yet
- Nursing CVDocument6 pagesNursing CVanil kumarNo ratings yet
- Pacemaker Invasive Cardiac PacingDocument57 pagesPacemaker Invasive Cardiac PacingAhmad Khalil Ahmad Al-SadiNo ratings yet
- Homeopathy in Intensive Care and Emergency Medicine: July 2015Document11 pagesHomeopathy in Intensive Care and Emergency Medicine: July 2015BABLU ROYNo ratings yet
- ANOM Lapsus PresentationDocument36 pagesANOM Lapsus PresentationPetrus TjiangNo ratings yet
- KARDIOGRAFIDocument86 pagesKARDIOGRAFIYusuf KamaruddinNo ratings yet
- Cambridge International General Certificate of Secondary EducationDocument20 pagesCambridge International General Certificate of Secondary Educationsalma RamadanNo ratings yet
- Case StudyDocument7 pagesCase StudyBiway RegalaNo ratings yet
- Vascular System 1 Anatomy and PhysiologyDocument5 pagesVascular System 1 Anatomy and PhysiologyLyssa KateNo ratings yet
- Class Test 3Document4 pagesClass Test 3shreyas DongreNo ratings yet
- Percutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookDocument15 pagesPercutaneous Interventional Cardiovascular Medicine - The PCR-EAPCI TextbookRanda TabbahNo ratings yet
- Aortic Stenosis Differential DiagnosisDocument12 pagesAortic Stenosis Differential DiagnosisCristina PorfireNo ratings yet
- Cryotherapy: DR - Farah Mir Bugti (PT) 3/3/2021Document12 pagesCryotherapy: DR - Farah Mir Bugti (PT) 3/3/2021aza bellaNo ratings yet
- Anatomy of The KidneyDocument5 pagesAnatomy of The Kidneycatherine kate gulengNo ratings yet
- Scientech 2357: Scope of LearningDocument1 pageScientech 2357: Scope of LearningSudip KunduNo ratings yet
- Hemodynamic DisordersDocument16 pagesHemodynamic DisordersHussein Al SaediNo ratings yet
- Acut Heart FailureDocument20 pagesAcut Heart FailureCatherine MorrisNo ratings yet
- Pathophysiology of Hydrops FetalisDocument10 pagesPathophysiology of Hydrops FetalisdrsunilpawarNo ratings yet
- II. Blood Vessels Physiology By: Dr. Abdulrahman Aqra MD MSCDocument12 pagesII. Blood Vessels Physiology By: Dr. Abdulrahman Aqra MD MSCapi-290338101No ratings yet
- Cardiovascular System ExaminationDocument67 pagesCardiovascular System ExaminationJaaydev100% (1)
- RN Expert Guides Cardiovascular Care PDFDocument512 pagesRN Expert Guides Cardiovascular Care PDFSteven Berschaminski100% (1)
- Finals Cardiovascular SystemDocument20 pagesFinals Cardiovascular SystemgabbypeigNo ratings yet
- M80637.04-Nicolet Elite BrochureDocument4 pagesM80637.04-Nicolet Elite BrochureRama Tenis CopecNo ratings yet
- Unit 2 ReviewDocument5 pagesUnit 2 Reviewduonghi3lpsNo ratings yet
- Drug StudyDocument6 pagesDrug StudyGeraldine Gallaron - CasipongNo ratings yet