Download as doc, pdf, or txt
You might also like
- Medical CertificateDocument2 pagesMedical Certificategcrajasekaran82% (11)
- Healthcare and Nursing Social Justice in Healthcare DistributionDocument3 pagesHealthcare and Nursing Social Justice in Healthcare DistributionNgọc QuỳnhNo ratings yet
- Anecdotal Records in NursingDocument5 pagesAnecdotal Records in NursingIndu KumariNo ratings yet
- University of San Francisco Student Health Insurance Plan For 2020 To 2021Document34 pagesUniversity of San Francisco Student Health Insurance Plan For 2020 To 2021The College FixNo ratings yet
- Dpa-E Bi 16 PDFDocument2 pagesDpa-E Bi 16 PDFJorgeHernanJaramilloNo ratings yet
- Physician Statement FormDocument2 pagesPhysician Statement Formmictesting123No ratings yet
- Mark Wesley Joseph SmithDocument2 pagesMark Wesley Joseph SmithMohammedNo ratings yet
- 2 Hipaa Front Notices-Page 1 2-13Document1 page2 Hipaa Front Notices-Page 1 2-13api-214017719No ratings yet
- Authorization Form For Researchers The Use and Disclosure of PHIDocument2 pagesAuthorization Form For Researchers The Use and Disclosure of PHImatiushynsNo ratings yet
- Authorization To Disclose Medical InformationDocument2 pagesAuthorization To Disclose Medical InformationFindLegalFormsNo ratings yet
- FORMS Informed Consent (For Procedures)Document1 pageFORMS Informed Consent (For Procedures)Jessa MaeNo ratings yet
- AMA WaiverDocument1 pageAMA WaiverTD BRNo ratings yet
- Consent To TreatDocument1 pageConsent To TreatfireflyimdNo ratings yet
- Consent FormsDocument2 pagesConsent FormsKristeline MedelNo ratings yet
- Sample Consent 2020 Update FinalDocument1 pageSample Consent 2020 Update FinalKevin G. DavisNo ratings yet
- Sample HIE Consent 2020 Update FinalDocument1 pageSample HIE Consent 2020 Update FinalKevin G. DavisNo ratings yet
- Privacy AcknowledgementDocument1 pagePrivacy Acknowledgementharrisk31No ratings yet
- Consent To CareDocument2 pagesConsent To CareJeanne Mari CostalesNo ratings yet
- Psycho Social AssessmentDocument10 pagesPsycho Social Assessmentaa985rocketmailNo ratings yet
- Surgery Consent FormDocument2 pagesSurgery Consent FormАлексей МалышкоNo ratings yet
- Hipaa Authorization For Use or Disclosure of Health InformationDocument3 pagesHipaa Authorization For Use or Disclosure of Health InformationSalsabilla NurfaniaNo ratings yet
- PHILPLANS Health Statement Form 1Document1 pagePHILPLANS Health Statement Form 1romelgregoriotorresNo ratings yet
- Clinical Referral FormDocument2 pagesClinical Referral FormJan Oneille Y. VallesNo ratings yet
- How To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormDocument3 pagesHow To Request Your Covid - 19 Lab Report: Complete The Consent To Disclose Phi FormAnithasree SrinivasanNo ratings yet
- Medical Record Authorization EnglishDocument1 pageMedical Record Authorization EnglishROBERTO BERLANGANo ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- Consent For Medications 2011Document1 pageConsent For Medications 2011maconjanice222No ratings yet
- Notification of Claim - Prudential GuaranteeDocument2 pagesNotification of Claim - Prudential GuaranteeZen Catolico ErumNo ratings yet
- CGH Release of InformationDocument2 pagesCGH Release of InformationEnoy LuNo ratings yet
- Roi Authorization Revision Final 08 27 13 PDFDocument1 pageRoi Authorization Revision Final 08 27 13 PDFHenry PannellNo ratings yet
- Mediclaim FormDocument1 pageMediclaim Formpicrush2pmNo ratings yet
- Adult Intake-1Document13 pagesAdult Intake-1Kimberly StanfordNo ratings yet
- HIPAADocument1 pageHIPAAwade_takenishiddsNo ratings yet
- CLAIMS 008 1022 7 Certificate of ClaimantDocument3 pagesCLAIMS 008 1022 7 Certificate of ClaimantEmsNo ratings yet
- Proposal Number / Nombor Cadangan: Soal Selidik Sakit BelakangDocument3 pagesProposal Number / Nombor Cadangan: Soal Selidik Sakit BelakangWan SaifulNo ratings yet
- Patient Information: X - Patient Signature or Legal Representative DateDocument1 pagePatient Information: X - Patient Signature or Legal Representative DateJohn FrinkNo ratings yet
- Records ReleaseDocument1 pageRecords ReleasechelseaNo ratings yet
- Attending Physicians Statement-Death ClaimDocument2 pagesAttending Physicians Statement-Death ClaimKen CelesteNo ratings yet
- SLMC-English-TELEHEALTH CONSENT FORMDocument3 pagesSLMC-English-TELEHEALTH CONSENT FORMyio16711No ratings yet
- HIPAA Privacy Authorization Form: 2835 20 Street Vero Beach, FL 32960 Telephone: (772) 299-3003 Fax: (772) 299-3005Document3 pagesHIPAA Privacy Authorization Form: 2835 20 Street Vero Beach, FL 32960 Telephone: (772) 299-3003 Fax: (772) 299-3005api-104636361No ratings yet
- Refusal To Treatment FormDocument1 pageRefusal To Treatment FormGlendaNo ratings yet
- Clinical Record Form: (May Be Completed by Patient)Document8 pagesClinical Record Form: (May Be Completed by Patient)Maria UlfahNo ratings yet
- Consent Form Pelvic ExaminationDocument2 pagesConsent Form Pelvic ExaminationGiullz EuguiNo ratings yet
- Health Care Proxy Form - EnglishDocument2 pagesHealth Care Proxy Form - EnglishTheFloatingHospitalNo ratings yet
- Patient Registration Form: General Information (Please Print Neatly)Document5 pagesPatient Registration Form: General Information (Please Print Neatly)Dan ThomasNo ratings yet
- MediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Document2 pagesMediHub Request For Letter of Guarantee Form 2021 v2 2 1 - 1Lhogeswaran RaviNo ratings yet
- Detailed Medical Records HippaDocument1 pageDetailed Medical Records HippaSergNo ratings yet
- Heritage Health - Pre Auth FormDocument6 pagesHeritage Health - Pre Auth FormBOOKREADER_NOWNo ratings yet
- Hipaa 1Document1 pageHipaa 1Gregory KnispelNo ratings yet
- Records ReleaseDocument1 pageRecords ReleaseChad MartinNo ratings yet
- TUE - WADA Version 2016-EnDocument4 pagesTUE - WADA Version 2016-EnYannick MOSSUSNo ratings yet
- Mental Health QuestionnaireDocument1 pageMental Health QuestionnaireNelly HNo ratings yet
- Certificate: (To Be Filled by The Hospital/ Nursing Home/ Clinic Authority)Document1 pageCertificate: (To Be Filled by The Hospital/ Nursing Home/ Clinic Authority)Darbha ShaliniNo ratings yet
- Physician Statement Form ETPDocument2 pagesPhysician Statement Form ETPKpi BrazilTwoNo ratings yet
- Hipaa Authorization For Use or Disclosure of Health InformationDocument3 pagesHipaa Authorization For Use or Disclosure of Health InformationNigil josephNo ratings yet
- AD Guide Entire Checklist v4Document37 pagesAD Guide Entire Checklist v4FAKESIGNUPACCOUNTNo ratings yet
- New Patient Package GodaddyDocument4 pagesNew Patient Package Godaddyapi-241814642No ratings yet
- JIT 2363 Authorization To Release Med RecordsDocument2 pagesJIT 2363 Authorization To Release Med Recordsalan benedettaNo ratings yet
- 451 Standard Authorization FormDocument3 pages451 Standard Authorization FormedzuckermanNo ratings yet
- COPC Authorization To Release InformationDocument1 pageCOPC Authorization To Release InformationLakee911No ratings yet
- APS FormDocument1 pageAPS Formviraj duaNo ratings yet
- CONSENT PROCEDURE - English - Oct2016Document2 pagesCONSENT PROCEDURE - English - Oct2016malaysiamadani01No ratings yet
- The Empowered Patient: Navigating the Healthcare System with ConfidenceFrom EverandThe Empowered Patient: Navigating the Healthcare System with ConfidenceNo ratings yet
- NCM 118Document7 pagesNCM 118Hazel MiraranNo ratings yet
- Chapter 12Document10 pagesChapter 12Mark Laurence GuillesNo ratings yet
- Brandi ADocument3 pagesBrandi Aapi-385247604No ratings yet
- Telepsychiatry Citations and Links by Jason CaferDocument25 pagesTelepsychiatry Citations and Links by Jason CaferJason Cafer100% (1)
- FY 2009 City Council Adopted Expense Budget Schedule CDocument246 pagesFY 2009 City Council Adopted Expense Budget Schedule CConnaissableNo ratings yet
- Hospital Services For Patients Residing in The Country For Year 2020 by EmiratesDocument2 pagesHospital Services For Patients Residing in The Country For Year 2020 by EmiratessherazalimemonNo ratings yet
- Dwnload Full Psychiatric Mental Health Nursing 5th Edition Fortinash Test Bank PDFDocument35 pagesDwnload Full Psychiatric Mental Health Nursing 5th Edition Fortinash Test Bank PDFchilyransei100% (13)
- Risk Management and Safety - EditedDocument9 pagesRisk Management and Safety - EditedViotry ChepkwonyNo ratings yet
- NCP AnxietyDocument3 pagesNCP AnxietyPaolo EspinosaNo ratings yet
- Reena Review1Document19 pagesReena Review1Yeshwanth SesettyNo ratings yet
- 10 Elements of A Just Patient Safety Culture WhitepaperDocument8 pages10 Elements of A Just Patient Safety Culture WhitepaperSema Sadullayeva02No ratings yet
- Medical Emergency Team (Met) - Adults: Warrnambool Campus OnlyDocument7 pagesMedical Emergency Team (Met) - Adults: Warrnambool Campus OnlytaqinosNo ratings yet
- American Well Case StudyDocument4 pagesAmerican Well Case StudyAnuj ChandaNo ratings yet
- Sample Report On Facilitating Change in Health and Social Care by Instant Essay WritingDocument17 pagesSample Report On Facilitating Change in Health and Social Care by Instant Essay WritingInstant Essay WritingNo ratings yet
- Building A Use Case For Community Based Peer Support in The Emergent Management of Opioid OverdoseDocument5 pagesBuilding A Use Case For Community Based Peer Support in The Emergent Management of Opioid OverdoseHerald Scholarly Open AccessNo ratings yet
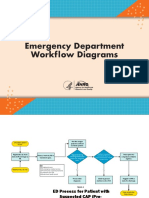
- Emergency Department Workflow DiagramsDocument5 pagesEmergency Department Workflow DiagramsMarwa El SayedNo ratings yet
- Angol - Nyelvvizsga B2 Listening (BME) 07-1 Female Doctors Are Better TextDocument1 pageAngol - Nyelvvizsga B2 Listening (BME) 07-1 Female Doctors Are Better TextCsaba GyörgyNo ratings yet
- Design Considerations For Hospitals and HotelsDocument18 pagesDesign Considerations For Hospitals and HotelsSaaviNo ratings yet
- Ella - (Effective Reporting and Record-Keeping in Health and Social Care Services)Document8 pagesElla - (Effective Reporting and Record-Keeping in Health and Social Care Services)Rajesh KumarNo ratings yet
- THE PROJECT HEALTH-Team BDocument33 pagesTHE PROJECT HEALTH-Team BNishtha RahejaNo ratings yet
- Shift Change ReportDocument30 pagesShift Change ReportAlfi Nur Hanifah100% (1)
- CV Janvi ThakkarDocument1 pageCV Janvi ThakkarJanki ThakkarNo ratings yet
- 1 Client Records 1Document15 pages1 Client Records 1Grape JuiceNo ratings yet
- Inspection Report: Windsor Dental PracticeDocument19 pagesInspection Report: Windsor Dental PracticeTeguh CaninusNo ratings yet
- Daisuke Tomita, Maki Sugimoto, Sachiko Kimizuka, Yumiko Tomita, Takuya Sueyoshi, Susumu OmuraDocument10 pagesDaisuke Tomita, Maki Sugimoto, Sachiko Kimizuka, Yumiko Tomita, Takuya Sueyoshi, Susumu OmurasalahoveNo ratings yet
- Emergency Departments and Crowding in United States Teaching HospitalsDocument7 pagesEmergency Departments and Crowding in United States Teaching HospitalsMaria CarlsonNo ratings yet
- Discharge Patient From The HospitalDocument4 pagesDischarge Patient From The HospitalEsamNo ratings yet