Download as pdf or txt
You might also like
- Complication of TPNDocument1 pageComplication of TPNNURSES' PAD100% (4)
- Nursing Care Plan Diabetes 2Document3 pagesNursing Care Plan Diabetes 2inagasi83% (12)
- Chapter 032Document22 pagesChapter 032dtheart2821100% (1)
- Respiratory Term 2Document13 pagesRespiratory Term 2Abegail QuintoNo ratings yet
- Altered Level of Consciousness (Ms Mark)Document5 pagesAltered Level of Consciousness (Ms Mark)Cristelle Joy RebocaNo ratings yet
- NCM116j Reviewer Endocrine UPDATEDDocument14 pagesNCM116j Reviewer Endocrine UPDATEDAliza Abn bklNo ratings yet
- Dengue Spectrum FinalDocument43 pagesDengue Spectrum Finalshyam kumar MishraNo ratings yet
- Blood Transfusion: 42 Days. Five DaysDocument5 pagesBlood Transfusion: 42 Days. Five DayskatsukagemaruNo ratings yet
- Abc Case 5Document19 pagesAbc Case 5Christian Dave EndinoNo ratings yet
- Tutorial Liver FailureDocument59 pagesTutorial Liver FailureNadhrah zulkifliNo ratings yet
- Midterm PRT 2aDocument24 pagesMidterm PRT 2aReysel MonteroNo ratings yet
- Ineffective Tissue Perfusion Nursing Care PlanDocument1 pageIneffective Tissue Perfusion Nursing Care PlankimmybapkiddingNo ratings yet
- NCP HemothoraxDocument3 pagesNCP Hemothoraxroseonabreeze0% (2)
- ATI Fluids, AcidBase, DietsDocument9 pagesATI Fluids, AcidBase, DietsBernardo AntonioNo ratings yet
- Acute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CDocument29 pagesAcute Glomerulonep Hritis: By: Edelrose D. Lapitan BSN Iii-CEdelrose Lapitan100% (1)
- NCM 118 - CCN - THEORY - MidtermsDocument19 pagesNCM 118 - CCN - THEORY - MidtermsSTEFFANIE VALE BORJANo ratings yet
- ShockDocument26 pagesShockdaisy100% (1)
- Serum Plasma Minus Fibrinogen Albumin Provides Osmotic PressureDocument13 pagesSerum Plasma Minus Fibrinogen Albumin Provides Osmotic PressureFreeNursingNotesNo ratings yet
- Treatment/ Infusion d5lrDocument1 pageTreatment/ Infusion d5lrjbespirituNo ratings yet
- Shock NotesDocument4 pagesShock NotesKenneth UbaldeNo ratings yet
- FE Enrichment 2024Document4 pagesFE Enrichment 2024tarahggggNo ratings yet
- Cirrhosis of LiverDocument1 pageCirrhosis of LiverShaini ChristianNo ratings yet
- CKD Presentation GroupDocument49 pagesCKD Presentation GroupAhmad BaolayyanNo ratings yet
- Shock and Its Management: Presented byDocument72 pagesShock and Its Management: Presented bysheme171150% (2)
- Shock PPT NewDocument21 pagesShock PPT NewcjimkarlNo ratings yet
- Dengue Management in Primary CareDocument61 pagesDengue Management in Primary CareDaniel RajNo ratings yet
- Hematological Alterations: Disseminated Intravascular Coagulation (DIC)Document16 pagesHematological Alterations: Disseminated Intravascular Coagulation (DIC)jhommmmmNo ratings yet
- Liver Biopsy: Mary Raina Angeli Fujiyoshi, MDDocument10 pagesLiver Biopsy: Mary Raina Angeli Fujiyoshi, MDRaina FujiyoshiNo ratings yet
- Pediatric Genitourinary DisordersDocument40 pagesPediatric Genitourinary DisordersGelsey Gelsinator JianNo ratings yet
- Med Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Document7 pagesMed Surg 2 - 7 Malabsorption Syndromes and Nursing Care of Clients With Hepatic Disorders 2Maxinne RoseñoNo ratings yet
- What Is Colonoscopy?Document4 pagesWhat Is Colonoscopy?Angel DamoNo ratings yet
- 1 Coagulation Disorderin PregnancyDocument21 pages1 Coagulation Disorderin PregnancyIntan Nursiani AgnurNo ratings yet
- Acute Tubular NecrosisDocument2 pagesAcute Tubular NecrosischoobiNo ratings yet
- Renal DisordersSDocument29 pagesRenal DisordersSpastrokateNo ratings yet
- Nursing Care of Patient On Dialysis 10Document17 pagesNursing Care of Patient On Dialysis 10Suji MerlineNo ratings yet
- Endo Session 3Document30 pagesEndo Session 3series recapNo ratings yet
- Nursing Care Plan NephritisDocument2 pagesNursing Care Plan Nephritisderic82% (17)
- Hematology: - What Are The Functions of The Blood?Document23 pagesHematology: - What Are The Functions of The Blood?Ricardo SimõesNo ratings yet
- DVT in PregDocument2 pagesDVT in Pregkhadzx100% (2)
- Pharmd - 4Y & 1Y (PB) - 4.3 - Clinical PharmacyDocument24 pagesPharmd - 4Y & 1Y (PB) - 4.3 - Clinical PharmacyDebasish SanyalNo ratings yet
- Renal EmergenciesDocument8 pagesRenal EmergenciesRENEROSE TORRESNo ratings yet
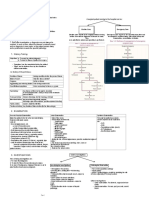
- Glomerular Disease: Nephrotic vs. NephriticDocument26 pagesGlomerular Disease: Nephrotic vs. NephriticMarcel DocNo ratings yet
- Midterm PRT 2 A qq9Document33 pagesMidterm PRT 2 A qq9Reysel MonteroNo ratings yet
- Nursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleDocument8 pagesNursing Care Plan 1: Diagnosis Goal Nursing Interventions RationaleTrysna Ayu SukardiNo ratings yet
- NORCETDocument101 pagesNORCETDiksha DhillonNo ratings yet
- Wardclasspptbt 120819085632 Phpapp01Document26 pagesWardclasspptbt 120819085632 Phpapp01Ryan-Jay AbolenciaNo ratings yet
- Abortion and Its Complications 2Document17 pagesAbortion and Its Complications 2api-3705046100% (2)
- Sepsis and MODS 2Document12 pagesSepsis and MODS 2Alex ChiuNo ratings yet
- Microsoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1Document23 pagesMicrosoft Word Oxygenation Handouts 2007 Nclex 1232010737844931 1api-19824701100% (1)
- NCP For Delivery RoomDocument4 pagesNCP For Delivery RoomGiselle EstoquiaNo ratings yet
- DialysisDocument19 pagesDialysisPatricia Mag-akatNo ratings yet
- BOX 17.4 NCP Postpartum HemorrhageDocument4 pagesBOX 17.4 NCP Postpartum HemorrhageJam AliNo ratings yet
- Fluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Document41 pagesFluid & Electrolyte, Acid-Base Imbalance (MS REPORT)Jane BelvisNo ratings yet
- Blood TransfusionDocument52 pagesBlood TransfusionCeljie OmresoNo ratings yet
- Management of A Cerebro-Vascular Accident (CVA) PTDocument45 pagesManagement of A Cerebro-Vascular Accident (CVA) PTmorati.lepNo ratings yet
- General Surgery IntroductionDocument1 pageGeneral Surgery IntroductionAndrew BonusNo ratings yet
- Hematologic DisorderDocument16 pagesHematologic DisorderZoe DorothyNo ratings yet
- Drugstudy BangkalDocument16 pagesDrugstudy BangkalClaire MachicaNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Ascites, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAscites, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- FormsDocument5 pagesFormsMatth N. ErejerNo ratings yet
- Changing and Discontinuing of IVFDocument1 pageChanging and Discontinuing of IVFMatth N. ErejerNo ratings yet
- Biological MoleculesDocument5 pagesBiological MoleculesMatth N. ErejerNo ratings yet
- Application of TravelbeeDocument1 pageApplication of TravelbeeMatth N. ErejerNo ratings yet
- Daliton-Uts4 AnswersDocument3 pagesDaliton-Uts4 AnswersMatth N. ErejerNo ratings yet
- Cell TheoryDocument3 pagesCell TheoryMatth N. ErejerNo ratings yet
- Intro MicroandParanotesDocument3 pagesIntro MicroandParanotesMatth N. ErejerNo ratings yet
- Dic PihDocument82 pagesDic PihMatth N. ErejerNo ratings yet
- Cellular RespirationDocument6 pagesCellular RespirationMatth N. ErejerNo ratings yet
- Slide 5 Cystic Fibrosis Mental IllnessDocument40 pagesSlide 5 Cystic Fibrosis Mental IllnessMatth N. ErejerNo ratings yet
- Clarithromycin DrugDocument1 pageClarithromycin DrugMatth N. ErejerNo ratings yet
- Metronidazole DrugDocument1 pageMetronidazole DrugMatth N. ErejerNo ratings yet
- Facilitating of Learning JunDocument12 pagesFacilitating of Learning JunMatth N. ErejerNo ratings yet
- Caber Human Environmental Factors Affecting MotivationDocument6 pagesCaber Human Environmental Factors Affecting MotivationMatth N. ErejerNo ratings yet
- Ischemic Stroke: Tarlac State University College of Science Department of NursingDocument21 pagesIschemic Stroke: Tarlac State University College of Science Department of NursingKrisianne Mae Lorenzo FranciscoNo ratings yet
- An Update Management of Acute Ischemic Stroke: SurotoDocument36 pagesAn Update Management of Acute Ischemic Stroke: SurotoShinta DianNo ratings yet
- Shock IndexDocument6 pagesShock IndexWILBERTH YOHEL PINEDO CALDASNo ratings yet
- Sally Scott CVDocument2 pagesSally Scott CVSally Jane ScottNo ratings yet
- Assessing Blood PressureDocument4 pagesAssessing Blood PressureCraigyyNo ratings yet
- ASCIA HP Guidelines Acute Management Anaphylaxis 2020Document8 pagesASCIA HP Guidelines Acute Management Anaphylaxis 2020Munshi KamrulNo ratings yet
- FWD PR2 PDFDocument58 pagesFWD PR2 PDFbernadineyamat19No ratings yet
- Nursing Care Plan 1 - DiarrheaDocument7 pagesNursing Care Plan 1 - DiarrheakirbyroohNo ratings yet
- t12 Manuale Bene Mobile - Manuale Service Eng Full - Monitor Parametri Vitali - Biomedicale - Fukuda - Ds 8100Document247 pagest12 Manuale Bene Mobile - Manuale Service Eng Full - Monitor Parametri Vitali - Biomedicale - Fukuda - Ds 8100mauro100% (1)
- Percentiles & Normal Distr (2-3) BiostatisticsDocument12 pagesPercentiles & Normal Distr (2-3) BiostatisticsBlackstarNo ratings yet
- Urden Chapter - 018 Cardio Diagnostic ProceduresDocument29 pagesUrden Chapter - 018 Cardio Diagnostic ProceduresTara McNeillNo ratings yet
- Non-Invasive Blood Pressure Monitoring: TutorialDocument6 pagesNon-Invasive Blood Pressure Monitoring: TutorialandymulyonoNo ratings yet
- Resit-1 Prelium XI BIOLOGY AKUEB Paper 2021Document29 pagesResit-1 Prelium XI BIOLOGY AKUEB Paper 2021Nusrat AbbasNo ratings yet
- Core Program (All Residents) : Saudi Board Anesthesia CurriculumDocument4 pagesCore Program (All Residents) : Saudi Board Anesthesia CurriculumHany ElbarougyNo ratings yet
- Infliximab ProtDocument5 pagesInfliximab ProtQusay AbdohNo ratings yet
- Case Presentation - HypertensionDocument24 pagesCase Presentation - HypertensionMazhabul AbirNo ratings yet
- Guias Hipertension 2023 Esc AnalisisDocument12 pagesGuias Hipertension 2023 Esc Analisismiguel contrerasNo ratings yet
- Acute Stroke PathwayDocument2 pagesAcute Stroke PathwayAnonymous eBmPrPNo ratings yet
- H. Pathophysiology I. Definition of Diagnosis A) Pregnancy Induced HypertensionDocument9 pagesH. Pathophysiology I. Definition of Diagnosis A) Pregnancy Induced HypertensionEmmy Flor ValmoriaNo ratings yet
- Pts 3a Mock Sba Series 2021 - Paper 1 - V3 - QuestionsDocument26 pagesPts 3a Mock Sba Series 2021 - Paper 1 - V3 - QuestionsmaiNo ratings yet
- Life Process Part 2 2Document32 pagesLife Process Part 2 2Anin BertNo ratings yet
- Federal Employee Program Incentive For Using CPT Category Ii CodesDocument2 pagesFederal Employee Program Incentive For Using CPT Category Ii CodesngNo ratings yet
- Assessment of The Frail Elderly Client: A. Skin, Hair, and NailsDocument11 pagesAssessment of The Frail Elderly Client: A. Skin, Hair, and Nailsshannon c. lewisNo ratings yet
- Equipment Used in Exercise Physiology and Its UsesDocument55 pagesEquipment Used in Exercise Physiology and Its UsesAkshayNo ratings yet
- 100 Item Exam On Fundamentals of Nursing KeysDocument14 pages100 Item Exam On Fundamentals of Nursing KeysMar BleNo ratings yet
- Strategies in Answering Reading Comprehension: Vocabulary Questions. The First Type Asks You To Answer QuestionsDocument9 pagesStrategies in Answering Reading Comprehension: Vocabulary Questions. The First Type Asks You To Answer QuestionsDuvi Ahmad Duvi DekanNo ratings yet
- Siwes ReportDocument27 pagesSiwes Reportkesiah700No ratings yet
- Clinical Procedures For Medical AssistantDocument40 pagesClinical Procedures For Medical AssistantStudent1010No ratings yet
- Intraocular Pressure: Harry Murgatroyd BSC MB CHB (Hons) Jane Bembridge MB CHB (Hons) FrcaDocument4 pagesIntraocular Pressure: Harry Murgatroyd BSC MB CHB (Hons) Jane Bembridge MB CHB (Hons) FrcaArmitha Putri NapitupuluNo ratings yet