Download as pdf or txt
You might also like
- Abcde Bundle ICU DeleriumDocument1 pageAbcde Bundle ICU DeleriumKelly MartinNo ratings yet
- Folk Violin SongbookDocument19 pagesFolk Violin SongbookTyler Swinn100% (1)
- 1 Copyreading and Headline WritingDocument72 pages1 Copyreading and Headline WritingAdrian Yan Yan Delara100% (2)
- 3 Ijmpsoct20173Document6 pages3 Ijmpsoct20173TJPRC PublicationsNo ratings yet
- Preoperative Medical Evaluation of The Healthy Patient: Author Section Editor Deputy EditorDocument11 pagesPreoperative Medical Evaluation of The Healthy Patient: Author Section Editor Deputy EditorAdimas Sandhi PermadiNo ratings yet
- JC Frailty As A Risk Predictor in Cardiac SurgeryDocument30 pagesJC Frailty As A Risk Predictor in Cardiac SurgeryFaizan Ahmad AliNo ratings yet
- Schlitzkus 2015Document25 pagesSchlitzkus 2015rnvisNo ratings yet
- Jamasurgery Shah 2018 Oi 180008Document10 pagesJamasurgery Shah 2018 Oi 180008John SmithNo ratings yet
- Gait Speed, Grip Strength, and Clinical Outcomes in Older Patients With Hematologic MalignanciesDocument9 pagesGait Speed, Grip Strength, and Clinical Outcomes in Older Patients With Hematologic MalignanciesTícia RanessaNo ratings yet
- Fried Frailty Pred Surg Outcomes AmCSurg 10Document8 pagesFried Frailty Pred Surg Outcomes AmCSurg 10edos838No ratings yet
- MN Community Measurement Total Knee Replacement Impact and Recommendation Document June 2010Document5 pagesMN Community Measurement Total Knee Replacement Impact and Recommendation Document June 2010ronnyNo ratings yet
- Frailty and AnesthesiaDocument33 pagesFrailty and AnesthesiaRadmila KaranNo ratings yet
- Clinical Diagnosis of Uncomplicated, Acute Appendicitis Remains An Imperfect ScienceDocument3 pagesClinical Diagnosis of Uncomplicated, Acute Appendicitis Remains An Imperfect ScienceHector ReinozoNo ratings yet
- Diagnostic Errors - UpToDateDocument23 pagesDiagnostic Errors - UpToDateJoyce SumagaysayNo ratings yet
- DINAMIC RISK in Differentiated Thyroid Cancer 2023Document15 pagesDINAMIC RISK in Differentiated Thyroid Cancer 2023Olga GarciaNo ratings yet
- What's New in Perioperative Cardiac TestingDocument17 pagesWhat's New in Perioperative Cardiac TestingCamilo HernándezNo ratings yet
- Use of The SOFA Score To Assess The Incidence of Organ Dysfunction/failure in Intensive Care Units: Results of A Multicenter, Prospective StudyDocument8 pagesUse of The SOFA Score To Assess The Incidence of Organ Dysfunction/failure in Intensive Care Units: Results of A Multicenter, Prospective StudybayuaaNo ratings yet
- BMJ f7095Document9 pagesBMJ f7095Luis Gerardo Pérez CastroNo ratings yet
- Patient Risk Factors Best Practices SsiDocument9 pagesPatient Risk Factors Best Practices SsiAl MuzakkiNo ratings yet
- Jurnal ReadingDocument8 pagesJurnal ReadingHezar SalahudinNo ratings yet
- Reliability and Predictive Validity of Inlow's 60-Second Diabetic Foot Screen ToolDocument6 pagesReliability and Predictive Validity of Inlow's 60-Second Diabetic Foot Screen ToolburhanNo ratings yet
- Apgar LansiaDocument7 pagesApgar Lansiawispa handayaniNo ratings yet
- CC 11904Document8 pagesCC 11904ikjaya3110No ratings yet
- Paper - Guidelines - Surviving Sepsis Campaign 2021Document67 pagesPaper - Guidelines - Surviving Sepsis Campaign 2021Harold JeffersonNo ratings yet
- Evans2021 Article SurvivingSepsisCampaignInternaDocument67 pagesEvans2021 Article SurvivingSepsisCampaignInternaPablo Antonio Cruz VivasNo ratings yet
- Guía Manejo Del Shock 2023Document67 pagesGuía Manejo Del Shock 2023Alvaro ArriagadaNo ratings yet
- An Analysis of The Causes of Adverse Events From The Quality in Australian Health Care StudyDocument7 pagesAn Analysis of The Causes of Adverse Events From The Quality in Australian Health Care StudyaxramosNo ratings yet
- Articulo 2021 - EfectosDocument5 pagesArticulo 2021 - Efectosmilena cedeñoNo ratings yet
- Surviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock 2021Document67 pagesSurviving Sepsis Campaign: International Guidelines For Management of Sepsis and Septic Shock 2021Khanh Ha NguyenNo ratings yet
- Full Title: Accuracy of Clinical Breast Examination's AbnormalitiesDocument21 pagesFull Title: Accuracy of Clinical Breast Examination's AbnormalitiesMaria AyaNo ratings yet
- J Geriatr Cardiol 2020 17 7 441-6Document6 pagesJ Geriatr Cardiol 2020 17 7 441-6Fernando SousaNo ratings yet
- 1 S PSCDocument8 pages1 S PSCKen WonNo ratings yet
- Pillai2016 PDFDocument35 pagesPillai2016 PDFmehak malhotraNo ratings yet
- Acute Appendicitis in Adults: Diagnostic EvaluationDocument9 pagesAcute Appendicitis in Adults: Diagnostic EvaluationJamie LittleNo ratings yet
- The Alvarado Score For Predicting Acute Appendicitis: A Systematic ReviewDocument13 pagesThe Alvarado Score For Predicting Acute Appendicitis: A Systematic ReviewAndy Zevallos AraujoNo ratings yet
- Validation of The French Version of The Vulnerable Elders Survey-13 (VES-13)Document6 pagesValidation of The French Version of The Vulnerable Elders Survey-13 (VES-13)cheatingw995No ratings yet
- ENG - Epidemiology Biostatistics IMGDocument8 pagesENG - Epidemiology Biostatistics IMGManivanh AvalosNo ratings yet
- Thromboprohylaxis and DVT in Surgical PRDocument7 pagesThromboprohylaxis and DVT in Surgical PRAhmed MohammedNo ratings yet
- Frailty - UpToDateDocument30 pagesFrailty - UpToDateTomas Andres Bahamondes CordovezNo ratings yet
- Predicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Document14 pagesPredicting The Risk of Malignancy in Adnexal Masses Based On IOTA AJOG 2016Fernando Suarez ChumaceroNo ratings yet
- Table 1: The Alvarado ScoreDocument4 pagesTable 1: The Alvarado ScoreRyan ChambersNo ratings yet
- 2013 - Tamizaje de Cancer en Ancianos Con DiscapacidadDocument6 pages2013 - Tamizaje de Cancer en Ancianos Con DiscapacidadRodrigoMarinNo ratings yet
- Falls and Health Status in Elderly Women Following First Eye Cataract Surgery: A Randomised Controlled TrialDocument7 pagesFalls and Health Status in Elderly Women Following First Eye Cataract Surgery: A Randomised Controlled TrialDede Achmad BasofiNo ratings yet
- Journal Pre-Proof: Clinical Lymphoma, Myeloma and LeukemiaDocument20 pagesJournal Pre-Proof: Clinical Lymphoma, Myeloma and LeukemiaYakobus Antonius SobuberNo ratings yet
- Inpatient Falls: Defining The Problem and Identifying Possible Solutions. Part I: An Evidence-Based ReviewDocument9 pagesInpatient Falls: Defining The Problem and Identifying Possible Solutions. Part I: An Evidence-Based ReviewDedes SahpitraNo ratings yet
- Sun 等。 - 2018 - Age-dependent difference in impact of fertility pr的副本Document10 pagesSun 等。 - 2018 - Age-dependent difference in impact of fertility pr的副本Jing WangNo ratings yet
- Periop Risk ScoringDocument7 pagesPeriop Risk ScoringMabelis EstherNo ratings yet
- Critical CareDocument7 pagesCritical CareOanamikaela VaidaNo ratings yet
- 775 FullDocument9 pages775 FullidaNo ratings yet
- 77d8 PDFDocument7 pages77d8 PDFRosyid PrasetyoNo ratings yet
- 2021 BJMO Geriatric Syndromes in OncologyDocument8 pages2021 BJMO Geriatric Syndromes in OncologyTarafainy BasalamahNo ratings yet
- Preoperative Medical Evaluation of The Healthy Adult Patient - UpToDateDocument45 pagesPreoperative Medical Evaluation of The Healthy Adult Patient - UpToDateAdrieli PansaniNo ratings yet
- 9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEDocument12 pages9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEmiftakhul jannahNo ratings yet
- Summary of Article "Screening Tests: A Review With Examples"Document5 pagesSummary of Article "Screening Tests: A Review With Examples"Keshav ChaudharyNo ratings yet
- Make A NewSenin 26 Januari 2015 EBM GLOSARY Dr. Akhmad EdiDocument12 pagesMake A NewSenin 26 Januari 2015 EBM GLOSARY Dr. Akhmad EdinaotonaoiNo ratings yet
- Scoping Review of Pediatric Early Warning SystemsDocument29 pagesScoping Review of Pediatric Early Warning SystemsCantika SRNo ratings yet
- Receiver Operating Characteristic (ROC) Curve For Medical ResearchersDocument11 pagesReceiver Operating Characteristic (ROC) Curve For Medical ResearchersRaúl Ferrer PeñaNo ratings yet
- Search BMJ GroupDocument23 pagesSearch BMJ GroupCharles BrooksNo ratings yet
- Error Reduction and Prevention in Surgical PathologyFrom EverandError Reduction and Prevention in Surgical PathologyRaouf E. NakhlehNo ratings yet
- Preclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1No ratings yet
- Top 20 Tricky Question From MTPDocument22 pagesTop 20 Tricky Question From MTPsanjanarawal09No ratings yet
- Ritishree Offer EztruckDocument4 pagesRitishree Offer EztruckKali RathNo ratings yet
- Pharmanex®: Food Supplement With Green Tea ExtractDocument2 pagesPharmanex®: Food Supplement With Green Tea ExtractMiriam Hui KungNo ratings yet
- Jargeous - Product - Catalog Ver 1220 Compressed PDFDocument16 pagesJargeous - Product - Catalog Ver 1220 Compressed PDFFirdaus YahyaNo ratings yet
- HVAC Pump Handbook, Second Edition - Access Engineering From McGraw-HillDocument7 pagesHVAC Pump Handbook, Second Edition - Access Engineering From McGraw-HillamigdalNo ratings yet
- Digital Communications Project ReportDocument14 pagesDigital Communications Project ReportSonal Pinto0% (1)
- WVA Consulting Engineers PVT LTD: Analsyis and Design of Steel Watch TowerDocument23 pagesWVA Consulting Engineers PVT LTD: Analsyis and Design of Steel Watch TowerRomyMohanNo ratings yet
- 4ipnet Solution HotelDocument27 pages4ipnet Solution HotelAdrian Gamboa MarcellanaNo ratings yet
- Maya, Aztec, and Inca Civilizations PDFDocument116 pagesMaya, Aztec, and Inca Civilizations PDFGabriel Medina100% (2)
- New Jersey AG Questions Lakewood Schools' Lawyer's SalaryDocument2 pagesNew Jersey AG Questions Lakewood Schools' Lawyer's SalaryStaceyNo ratings yet
- KMA CVDocument5 pagesKMA CVKhandoker Mostak AhamedNo ratings yet
- Türkiye'deki Bazı Semi-Finish Grinding SistemleriDocument4 pagesTürkiye'deki Bazı Semi-Finish Grinding SistemleriTHAKARAR HARSHILNo ratings yet
- Coldplay - Higher Power (Uke Cifras)Document2 pagesColdplay - Higher Power (Uke Cifras)Jamille MesquitaNo ratings yet
- Evaporation of Different Liquids PDFDocument2 pagesEvaporation of Different Liquids PDFMandyNo ratings yet
- Filtrec F040 SeriesDocument8 pagesFiltrec F040 Serieshkhan10No ratings yet
- Depth of FocusDocument7 pagesDepth of FocusDr-Riya MondalNo ratings yet
- Installation and Maintenance Manual For The GP Poro-Stone Gas FilterDocument4 pagesInstallation and Maintenance Manual For The GP Poro-Stone Gas FilterMahmoud El-abdNo ratings yet
- Smietanka v. First Trust & Savings Bank: 257 U.S. 602 (1922) : Justia US Supreme Court CenterDocument1 pageSmietanka v. First Trust & Savings Bank: 257 U.S. 602 (1922) : Justia US Supreme Court CenterChou TakahiroNo ratings yet
- School - Guest Faculty Management SystemDocument1 pageSchool - Guest Faculty Management SystemSuraj BadholiyaNo ratings yet
- Expedition DiaryDocument23 pagesExpedition DiaryAnkur JhunjhunwalaNo ratings yet
- Knowledge, Creativity and Communication in Education: Multimodal DesignDocument11 pagesKnowledge, Creativity and Communication in Education: Multimodal DesignMartín VillagraNo ratings yet
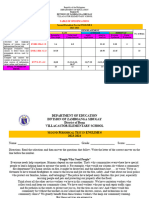
- PT English-6 Q2Document7 pagesPT English-6 Q2Elona Jane CapangpanganNo ratings yet
- Lab Work 1Document2 pagesLab Work 1Adly HakimNo ratings yet
- K-System Isolated Barriers: ManualDocument52 pagesK-System Isolated Barriers: ManualPaul Ramos CarcaustoNo ratings yet
- Deyu Cai: General Notes and SpecificationDocument1 pageDeyu Cai: General Notes and SpecificationSKYLERNo ratings yet
- Servicemanual Panasonic kv-s5046h 5076h s3Document17 pagesServicemanual Panasonic kv-s5046h 5076h s3Ralf KöhlerNo ratings yet
- Assessment For Learning A Practical GuideDocument108 pagesAssessment For Learning A Practical Guidesh1999100% (1)
- Mil M3 LearnersDocument2 pagesMil M3 Learnersfast6No ratings yet