Download as pdf or txt
You might also like
- Infection ControlDocument23 pagesInfection ControlUdaya Sree67% (3)
- Management of Infectious Discitis. Outcome in One Hundred and Eight Patients in A University HospitalDocument6 pagesManagement of Infectious Discitis. Outcome in One Hundred and Eight Patients in A University HospitalKarina PortilloNo ratings yet
- Ajayan 2013Document3 pagesAjayan 2013Dung TranNo ratings yet
- CKD PDFDocument7 pagesCKD PDFniaNo ratings yet
- Streptococcus Suis Infection: Overview of Case Reports: in ThailandDocument6 pagesStreptococcus Suis Infection: Overview of Case Reports: in ThailandAram Dumnoen-ngamNo ratings yet
- Chronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With SepsisDocument8 pagesChronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With Sepsisida ayu agung WijayantiNo ratings yet
- Lander 2016Document2 pagesLander 2016Jocilene Dantas Torres NascimentoNo ratings yet
- 149 FullDocument10 pages149 Fullসোমনাথ মহাপাত্রNo ratings yet
- Epidemiology and Clinical Manifestations of Mucormycosis CMIDocument9 pagesEpidemiology and Clinical Manifestations of Mucormycosis CMIDINESH VENKATESANNo ratings yet
- Ye 2014Document8 pagesYe 2014dickypranataNo ratings yet
- Ioi80197 463 473Document11 pagesIoi80197 463 473Phạm LinhNo ratings yet
- 1 s2.0 S1201971209003063 MainDocument4 pages1 s2.0 S1201971209003063 Mainlee zaraNo ratings yet
- Founier GangrenDocument5 pagesFounier GangrenJohannes MarpaungNo ratings yet
- Jamadermatology Kridin 2021 Oi 210045 1634154542.6481Document9 pagesJamadermatology Kridin 2021 Oi 210045 1634154542.6481Nandha KumarNo ratings yet
- Saini 2016 Calci NoseDocument5 pagesSaini 2016 Calci NoseRym MesfarNo ratings yet
- 3 - Tuberculous Meningitis in Adults - Review of 48 Cases 1996 (Modelo para o Trabalho)Document7 pages3 - Tuberculous Meningitis in Adults - Review of 48 Cases 1996 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Deep Neck Infections: Continuing Burden in Developing World: Original ArticleDocument4 pagesDeep Neck Infections: Continuing Burden in Developing World: Original ArticlevaNo ratings yet
- Bulatovic HEPARIN INDUCED THROMBOCYTOPENIA AND Hemodialysis Single Center ExperienceDocument1 pageBulatovic HEPARIN INDUCED THROMBOCYTOPENIA AND Hemodialysis Single Center ExperienceJobertNo ratings yet
- JurnalDocument5 pagesJurnalgustina mariantiNo ratings yet
- 10 1016@j Jaad 2019 05 096Document8 pages10 1016@j Jaad 2019 05 096JohnNo ratings yet
- Clinical Microbiology and InfectionDocument9 pagesClinical Microbiology and InfectionAguilarKrystell'No ratings yet
- mdw557 2Document7 pagesmdw557 2mfaddhilNo ratings yet
- Neutropenic Colitis in Children 2011Document4 pagesNeutropenic Colitis in Children 2011IRINA SULEY TIRADO PEREZNo ratings yet
- SaudiJKidneyDisTranspl302470-5143025 141710Document8 pagesSaudiJKidneyDisTranspl302470-5143025 141710AmatystNo ratings yet
- Brain Abscess: Clinical Analysis of 53 CasesDocument8 pagesBrain Abscess: Clinical Analysis of 53 CasesIqbal AbdillahNo ratings yet
- Systemic - Sclerosis Nature Review 2014Document22 pagesSystemic - Sclerosis Nature Review 2014CT TANNo ratings yet
- Predictors of Septic Metastatic Infection and Mortality Among Patients With KlebsiellaDocument9 pagesPredictors of Septic Metastatic Infection and Mortality Among Patients With KlebsiellaJeanetteNo ratings yet
- Hydatid Disease of Central Nervous System, A Clinicopathological Study of 33 CasesDocument5 pagesHydatid Disease of Central Nervous System, A Clinicopathological Study of 33 CasesIvory Arévalo ManríquezNo ratings yet
- Mucormycosis in Children: A Study of 22 Cases in A Mexican HospitalDocument6 pagesMucormycosis in Children: A Study of 22 Cases in A Mexican Hospitalandrianiputri916No ratings yet
- Idsa GuidelinesDocument34 pagesIdsa GuidelinesROSEN NNo ratings yet
- Risk Factor TaiwanDocument5 pagesRisk Factor TaiwanMira ApriliaNo ratings yet
- 1gorgan BrainAbcessesDocument8 pages1gorgan BrainAbcessesHaryono HaryNo ratings yet
- Prognostic Factors For Progression Free and Overall Survival in Malignant PleuralDocument9 pagesPrognostic Factors For Progression Free and Overall Survival in Malignant PleuralAlanNo ratings yet
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiNo ratings yet
- Thwaites 2004Document11 pagesThwaites 2004Navisa HaifaNo ratings yet
- (RCT) Cardiovascular Injuries After Covid-19 InfectionDocument7 pages(RCT) Cardiovascular Injuries After Covid-19 InfectionPatrick NunsioNo ratings yet
- Bou Quill Ard 2009Document3 pagesBou Quill Ard 2009Rohit RajeevanNo ratings yet
- Otogenic Complications of Otitis Media Experience at Tertiary Care HospitalDocument5 pagesOtogenic Complications of Otitis Media Experience at Tertiary Care HospitalAjeng Ratna HaryantiNo ratings yet
- J Clin Tuberc Other Mycobact Dis: SciencedirectDocument7 pagesJ Clin Tuberc Other Mycobact Dis: SciencedirectNidya PutriNo ratings yet
- Systemic Sclerosis - 2015Document21 pagesSystemic Sclerosis - 2015XRobert17No ratings yet
- Warley 2017Document1 pageWarley 2017cecibroedersNo ratings yet
- Clinical Presentation of Scrub Typhus During A Major Outbreak in Central NepalDocument5 pagesClinical Presentation of Scrub Typhus During A Major Outbreak in Central NepalArun SedhainNo ratings yet
- 10 11648 J Ijidt 20200501 12Document5 pages10 11648 J Ijidt 20200501 12hern andesNo ratings yet
- TBM MedscapeDocument5 pagesTBM MedscapeAsnan Azis FatoniNo ratings yet
- 1 s2.0 S0268960X22000182 MainDocument10 pages1 s2.0 S0268960X22000182 Mainafg_19No ratings yet
- Neurologia MeningiteDocument10 pagesNeurologia MeningitesuzanaNo ratings yet
- 220 FullDocument4 pages220 FullOttofianus Alvedo Hewick KalangiNo ratings yet
- JIAO - 20210313 - A Different Era For Malignant Otitis Externa The Non-Diabetic and Non-Immunocompromised PatientsDocument5 pagesJIAO - 20210313 - A Different Era For Malignant Otitis Externa The Non-Diabetic and Non-Immunocompromised PatientsJohn LatzonisNo ratings yet
- Silent NightDocument6 pagesSilent NightApril Rae Obregon GarcesNo ratings yet
- Jurnal PatogenesisDocument6 pagesJurnal PatogenesisErmiati EmhyNo ratings yet
- DR Julian-MYOCARDITISDocument83 pagesDR Julian-MYOCARDITISArmando Esteban Coa SandovalNo ratings yet
- 1 s2.0 S1201971205001839 MainDocument6 pages1 s2.0 S1201971205001839 MainsivanthiNo ratings yet
- Original Article: Clinical and Histopathological Correlation of Cutaneous TuberculosisDocument6 pagesOriginal Article: Clinical and Histopathological Correlation of Cutaneous Tuberculosisderil ridwanNo ratings yet
- 100220080112Document8 pages100220080112Nabil MrhiliNo ratings yet
- Takayasu Arteritis Challenges in DiagnosisDocument9 pagesTakayasu Arteritis Challenges in DiagnosisYesenia HuertaNo ratings yet
- Primer: Systemic SclerosisDocument21 pagesPrimer: Systemic Sclerosishumberto_620No ratings yet
- Diagnostics 11 02008 v2Document12 pagesDiagnostics 11 02008 v2Fatoş TekelioğluNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- American J Hematol - 2007 - Mistry - Consequences of Diagnostic Delays in Type 1 Gaucher Disease The Need For GreaterDocument6 pagesAmerican J Hematol - 2007 - Mistry - Consequences of Diagnostic Delays in Type 1 Gaucher Disease The Need For GreatererenNo ratings yet
- Epidemiology and Outcome ofDocument20 pagesEpidemiology and Outcome ofrgumralNo ratings yet
- Encyclopedia of Infectious Diseases: Modern MethodologiesFrom EverandEncyclopedia of Infectious Diseases: Modern MethodologiesMichel TibayrencNo ratings yet
- Nocardia (2019) GuidelineDocument12 pagesNocardia (2019) Guidelinephuong mai leNo ratings yet
- Clinical Microbiology 2Document20 pagesClinical Microbiology 2phuong mai leNo ratings yet
- ExaminationDocument271 pagesExaminationphuong mai leNo ratings yet
- Asm Beta Lactamase Cmr.00047 19Document37 pagesAsm Beta Lactamase Cmr.00047 19phuong mai leNo ratings yet
- Diagnostic Challenges in Musculoskeletal Radiology PDFDocument182 pagesDiagnostic Challenges in Musculoskeletal Radiology PDFphuong mai leNo ratings yet
- Keertan Dheda (3) TB Test PDFDocument48 pagesKeertan Dheda (3) TB Test PDFphuong mai leNo ratings yet
- What Is Global Health and Why Is It ImportantDocument7 pagesWhat Is Global Health and Why Is It ImportantSanty ManuelNo ratings yet
- Vaccination Programs in Poultry - Poultry - Veterinary ManualDocument2 pagesVaccination Programs in Poultry - Poultry - Veterinary ManualAbd Al-Rhman SalminNo ratings yet
- Occupational Health QuestionnaireDocument2 pagesOccupational Health QuestionnaireRuby MooreNo ratings yet
- Components of EpidemiologyDocument13 pagesComponents of EpidemiologyGAURAV KUMARNo ratings yet
- Bed BathDocument10 pagesBed BathjokazelNo ratings yet
- Approach To PCM CasesDocument310 pagesApproach To PCM CasesgjdbfiuvaNo ratings yet
- 363713v1 FullDocument27 pages363713v1 FullALI MAKRINo ratings yet
- CorynebacteriumDocument14 pagesCorynebacteriumGerrard Angelo CastillaNo ratings yet
- A.respiratory HistoryDocument3 pagesA.respiratory HistoryEl SpinnerNo ratings yet
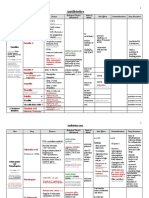
- Antimicrobial Drugs TableDocument19 pagesAntimicrobial Drugs TableLaylee ClareNo ratings yet
- Assessment of Bacterial Contamination in Cellular PhonesDocument8 pagesAssessment of Bacterial Contamination in Cellular PhonesMedrechEditorialNo ratings yet
- Chocolate AgarDocument5 pagesChocolate AgarBramita Beta ArnandaNo ratings yet
- PPK IB Lap Rekapitulasi 10 Besar Penyakit MeiDocument3 pagesPPK IB Lap Rekapitulasi 10 Besar Penyakit MeiwahyumozabillaNo ratings yet
- Infective Endocarditis-2023Document40 pagesInfective Endocarditis-2023يزن الحارثيNo ratings yet
- 3 Streptococcus: 3.2.1 The Direct Bacteriological Diagnosis in Streptococcal PharyngitisDocument5 pages3 Streptococcus: 3.2.1 The Direct Bacteriological Diagnosis in Streptococcal PharyngitisMahmoud IdlbiNo ratings yet
- Ao 2007-0036 Pidsr PDFDocument16 pagesAo 2007-0036 Pidsr PDFRey San Luis III100% (2)
- EFA Pembahasan Strategi 3 ReadingDocument29 pagesEFA Pembahasan Strategi 3 ReadingFitria AndrinaNo ratings yet
- Sharp Injury PreventionDocument12 pagesSharp Injury Preventionsimmi2768No ratings yet
- Schreibman - Radiology of Joint Disease - My Practical ApproachDocument16 pagesSchreibman - Radiology of Joint Disease - My Practical ApproachborstNo ratings yet
- PSM Workbook (Empty)Document50 pagesPSM Workbook (Empty)Srishti PrasadNo ratings yet
- VDRL Test and Its InterpretationDocument8 pagesVDRL Test and Its InterpretationThyago SilvaNo ratings yet
- ObatDocument1 pageObatLiezna MusyarofaNo ratings yet
- Calcified Ranke ComplexDocument2 pagesCalcified Ranke ComplexRomel BarrientosNo ratings yet
- Periodontal AbcessDocument52 pagesPeriodontal Abcessperiodontics07100% (1)
- Communicable Disease Paper Hepatits BDocument2 pagesCommunicable Disease Paper Hepatits BMandy MartinNo ratings yet
- Listado Microorganismos MALDIDocument51 pagesListado Microorganismos MALDIElias ENo ratings yet
- COVID-19 in ChildrenDocument9 pagesCOVID-19 in ChildrenFarahdina UmarellaNo ratings yet
- Febra La Pacientul Imunodeprimat (Romana)Document59 pagesFebra La Pacientul Imunodeprimat (Romana)ialomitaNo ratings yet
- Luna Apple Fungicide - 2012 Product GuideDocument2 pagesLuna Apple Fungicide - 2012 Product GuideLunaFungicidesNo ratings yet