
4 Correlations Between Age, Pain Intensity, Disability, and Tactile Acuity in Patients With Chronic Low Back Pain
4 Correlations Between Age, Pain Intensity, Disability, and Tactile Acuity in Patients With Chronic Low Back Pain
You might also like
- Separation Process Engineering Includes Mass Transfer Analysis 4th Edition Wankat Solution ManualDocument54 pagesSeparation Process Engineering Includes Mass Transfer Analysis 4th Edition Wankat Solution Manualjacob100% (31)
- Hose Products and Tooling Guide 8th EditionDocument332 pagesHose Products and Tooling Guide 8th EditionKeron Trotz100% (4)
- #128 - Harvie - 2021 - Discrimination - Training - Neck - Pain - ProtocolDocument7 pages#128 - Harvie - 2021 - Discrimination - Training - Neck - Pain - ProtocolsoylahijadeunvampiroNo ratings yet
- Effects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialDocument14 pagesEffects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialLorena Rico ArtigasNo ratings yet
- The Relationship Between Rate of Algometer Application and Pain Pressure Threshold in TheDocument16 pagesThe Relationship Between Rate of Algometer Application and Pain Pressure Threshold in TheRafael BohnenbergerNo ratings yet
- RetrieveDocument9 pagesRetrieveSuttinont SurapuchongNo ratings yet
- Comparison of The Effects Between Lasers AppliedDocument29 pagesComparison of The Effects Between Lasers AppliedHelena GaribottiNo ratings yet
- 2015 - Article - 665eficacia EpicondilitiDocument13 pages2015 - Article - 665eficacia EpicondilitimorbreirNo ratings yet
- Bowen Back Pain WSN-93-2018-81-94Document14 pagesBowen Back Pain WSN-93-2018-81-94Saleha TariqNo ratings yet
- 2016 Article 653Document20 pages2016 Article 653CaioSelaimenNo ratings yet
- 904nm 0.6W - 12663 - 2013 - Article - 544Document7 pages904nm 0.6W - 12663 - 2013 - Article - 544Gino DammiuncrodinoNo ratings yet
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiNo ratings yet
- 2015 Sensorimotor Control in The Hand As An Outcome IndicatorDocument12 pages2015 Sensorimotor Control in The Hand As An Outcome IndicatorClaudia Chinchilla ZeceñaNo ratings yet
- Poster PapersDocument262 pagesPoster PapersLeonardo RodríguezNo ratings yet
- JCM 08 00051 v2Document7 pagesJCM 08 00051 v2joelruizmaNo ratings yet
- Efficacy of Repetitive Transcranial Magnetic StimuDocument28 pagesEfficacy of Repetitive Transcranial Magnetic Stimuluz elena guerraNo ratings yet
- 2 Ijpotdec20172Document10 pages2 Ijpotdec20172TJPRC PublicationsNo ratings yet
- Buyukturan 2018Document8 pagesBuyukturan 2018Eka BagaskaraNo ratings yet
- Comparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDocument29 pagesComparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDrPratibha SinghNo ratings yet
- Park 2014Document7 pagesPark 2014Nurfitrianti ArfahNo ratings yet
- Observational Pilot Study of Patients With Carpal Tunnel Syndrome Treated With Nucleo CMP ForteDocument8 pagesObservational Pilot Study of Patients With Carpal Tunnel Syndrome Treated With Nucleo CMP ForteRicardo BarcoNo ratings yet
- 16 Van Leerdam Et Al J Hand Surg Eur Vol. 2017 Jun 42 5 501 506 AAMDocument13 pages16 Van Leerdam Et Al J Hand Surg Eur Vol. 2017 Jun 42 5 501 506 AAMChristopher Freddy Bermeo RiveraNo ratings yet
- Effect of Positional Release Technique in Subjects With Subacute TrapezitisDocument9 pagesEffect of Positional Release Technique in Subjects With Subacute TrapezitisijphyNo ratings yet
- J Jpain 2012 01 047Document1 pageJ Jpain 2012 01 047adssaNo ratings yet
- Functional Outcome of Carpal Tunnel Syndrome After Exercise Versus Ultrasound DiathermyDocument8 pagesFunctional Outcome of Carpal Tunnel Syndrome After Exercise Versus Ultrasound DiathermyAdelia 102013330No ratings yet
- Research Paper 1Document14 pagesResearch Paper 1Ayesha HabibNo ratings yet
- Full TextDocument7 pagesFull TextJuan Pablo Casanova AnguloNo ratings yet
- Bmjopen 2021 051073Document12 pagesBmjopen 2021 051073Eugênio AraújoNo ratings yet
- Chen 2013Document5 pagesChen 2013RenaldiPrimaSaputraNo ratings yet
- Grossnickle Literature Review PaperDocument8 pagesGrossnickle Literature Review Paperapi-627301337No ratings yet
- Extracorporeal Shock Wave Therapy VersusDocument7 pagesExtracorporeal Shock Wave Therapy VersusGiannis SaramantosNo ratings yet
- Effect of Manual Therapy and Neurodynamic Techniques VsDocument10 pagesEffect of Manual Therapy and Neurodynamic Techniques VsTomBramboNo ratings yet
- 2408 2413Document6 pages2408 2413Anandhu GNo ratings yet
- Researcharticle Open Access: Philipp Wälti, Jan Kool and Hannu LuomajokiDocument11 pagesResearcharticle Open Access: Philipp Wälti, Jan Kool and Hannu LuomajokiRoaa MansourNo ratings yet
- Dunning James Et AlDocument10 pagesDunning James Et Alapi-290796947No ratings yet
- Randomizado-Us Pulsado e Fono em Tunel Do CarpoDocument9 pagesRandomizado-Us Pulsado e Fono em Tunel Do CarpoELONo ratings yet
- Medicina 58 01332Document27 pagesMedicina 58 01332Putu DeaNo ratings yet
- Lopez 2021Document9 pagesLopez 2021toaldoNo ratings yet
- MJCU - Volume 88 - Issue September - Pages 1601-1614Document9 pagesMJCU - Volume 88 - Issue September - Pages 1601-1614fomoNo ratings yet
- CBMT and NTDocument11 pagesCBMT and NTrizkiriasariNo ratings yet
- Chronic Ankle InstabilityDocument9 pagesChronic Ankle InstabilityJonathan Elias Barrientos OssesNo ratings yet
- 2015 LeeDocument3 pages2015 LeeJavier PelaezNo ratings yet
- 2019-Prolotherapy-Vs-Eswt-For-Lateral-Epicondylosis VS ONDAS DE CHOQUEDocument5 pages2019-Prolotherapy-Vs-Eswt-For-Lateral-Epicondylosis VS ONDAS DE CHOQUEDuilio GuzzardoNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- Cognitive Impairment 3 Months After Moderate and Severe Traumatic Brain Injury: A Prospective Follow-Up StudyDocument10 pagesCognitive Impairment 3 Months After Moderate and Severe Traumatic Brain Injury: A Prospective Follow-Up StudyIngrid Nayibe Díaz EspinosaNo ratings yet
- 1 s2.0 S0020138320310548 MainDocument7 pages1 s2.0 S0020138320310548 MainAURORA BADIALINo ratings yet
- FFT®: Functional Fascial Taping®Document5 pagesFFT®: Functional Fascial Taping®BwizerNo ratings yet
- Hypoesthesia Associated With Mandibular Movement After Sagittal Split Ramus OsteotomyDocument7 pagesHypoesthesia Associated With Mandibular Movement After Sagittal Split Ramus OsteotomyBruno ManNo ratings yet
- SSRN Id3705177Document222 pagesSSRN Id3705177Paula Heline NisanshaNo ratings yet
- Reduction of Spontaneous Electrical Activity and Pain Perception of Trigger Points in The Upper Trapezius Muscle Through Trigger Point Compression and Passive StretchingDocument13 pagesReduction of Spontaneous Electrical Activity and Pain Perception of Trigger Points in The Upper Trapezius Muscle Through Trigger Point Compression and Passive StretchingKapil SharmaNo ratings yet
- Articulo BrasileroDocument8 pagesArticulo BrasileroLuis GalvanNo ratings yet
- A Deep Neural Network-Based Pain Classifier Using A Photoplethysmography SignalDocument16 pagesA Deep Neural Network-Based Pain Classifier Using A Photoplethysmography SignalPING KWAN MANNo ratings yet
- ScientificDocument4 pagesScientificKiran AbidNo ratings yet
- 410 4225 PDFDocument5 pages410 4225 PDFmilhimNo ratings yet
- Comparing The Effects of Manual Therapy Versus Electrophysical Agents in The Management of Knee OsteoarthritisDocument4 pagesComparing The Effects of Manual Therapy Versus Electrophysical Agents in The Management of Knee OsteoarthritisNurul MuslihahNo ratings yet
- Tendon 2Document10 pagesTendon 2Verónica Téllez ArriagaNo ratings yet
- Paper 4Document13 pagesPaper 4Pablo Cuevas SaldivarNo ratings yet
- Osteopathic Manipulation Treatment Versus Therapeutic Exercises in Patients With Chronic Nonspecific Low Back PainDocument11 pagesOsteopathic Manipulation Treatment Versus Therapeutic Exercises in Patients With Chronic Nonspecific Low Back PainBruno AssunçaoNo ratings yet
- Temporomandibular DisordersDocument8 pagesTemporomandibular DisordersItzel VargasNo ratings yet
- Palpation of The Lateral Pterygoid Area in The Myofascial Pain DiagnosisDocument6 pagesPalpation of The Lateral Pterygoid Area in The Myofascial Pain Diagnosisdavidcosmin186832No ratings yet
- Clinical Gait Assessment in The Neurologically ImpairedDocument6 pagesClinical Gait Assessment in The Neurologically Impairedvamat63No ratings yet
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- Mt4gui CheatsheetDocument2 pagesMt4gui Cheatsheetbinosp2No ratings yet
- Us0ab 21023133 21023133Document1 pageUs0ab 21023133 21023133krish.gkavarapuNo ratings yet
- Fintech Adoption and Its Impact On Sustainability: Risk Benefit Analysis of An Emerging EconomyDocument32 pagesFintech Adoption and Its Impact On Sustainability: Risk Benefit Analysis of An Emerging EconomyAudit and Accounting ReviewNo ratings yet
- DC Circuit Breakers:: An Important Role in The Continuity and Quality of ServiceDocument3 pagesDC Circuit Breakers:: An Important Role in The Continuity and Quality of ServiceSagar GadhiaNo ratings yet
- GogugugDocument2 pagesGogugugvipin kumarNo ratings yet
- Senior HighschoolDocument3 pagesSenior HighschoolAngelica MathewNo ratings yet
- TimkooDocument1 pageTimkooAli HabibNo ratings yet
- Philippine LiteratureDocument26 pagesPhilippine LiteratureCierly Mae TantanNo ratings yet
- Advancements in Weft Knitting TechnologyDocument28 pagesAdvancements in Weft Knitting TechnologyAbhi Sheikh100% (1)
- 1246 SP 4 Emm 24003 B2Document132 pages1246 SP 4 Emm 24003 B2Arash Aghagol100% (1)
- Suzuki Ertiga p1-26Document26 pagesSuzuki Ertiga p1-26bonruiz100% (2)
- CEM130 Construction Safety Management - SYLLABUS RevisedDocument5 pagesCEM130 Construction Safety Management - SYLLABUS Reviseddel rosarioNo ratings yet
- CH 19 Cash and Liquidity Management Appendix Class WorkDocument4 pagesCH 19 Cash and Liquidity Management Appendix Class WorkMhmd KaramNo ratings yet
- Introduction To Copulas: Mark S. Tenney Mathematical Finance Company July 18, 2003Document9 pagesIntroduction To Copulas: Mark S. Tenney Mathematical Finance Company July 18, 2003Mario CruzNo ratings yet
- Variable Valve Timing & Acoustic Control Induction Systems: Section 8Document19 pagesVariable Valve Timing & Acoustic Control Induction Systems: Section 8sungjoo75No ratings yet
- Us 1 NUM 10xx Series CNC Backup/ Restore Procedures Using NUMBackUp 14 10xx NUMBackupDocument3 pagesUs 1 NUM 10xx Series CNC Backup/ Restore Procedures Using NUMBackUp 14 10xx NUMBackupHa Pro50% (2)
- DCRM 6 Channel NewDocument9 pagesDCRM 6 Channel NewSayan ChatterjeeNo ratings yet
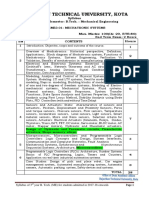
- Rajasthan Technical University, Kota: Syllabus 3 Year - V Semester: B.Tech.: Mechanical EngineeringDocument1 pageRajasthan Technical University, Kota: Syllabus 3 Year - V Semester: B.Tech.: Mechanical Engineeringsharad pareekNo ratings yet
- Ui22 Lab1Document5 pagesUi22 Lab1dattpatel2020No ratings yet
- Anfis (Adaptive Network Fuzzy Inference System) : G.AnuradhaDocument25 pagesAnfis (Adaptive Network Fuzzy Inference System) : G.Anuradhamodis777No ratings yet
- Inquiries, Investigation, and ImmersionDocument6 pagesInquiries, Investigation, and ImmersioniNo ratings yet
- English TestDocument5 pagesEnglish TestfabiolaNo ratings yet
- Gha Ba Ags531441-01 enDocument68 pagesGha Ba Ags531441-01 enRagab TolbaNo ratings yet
- The Department of Ethnography: Reading Passage 1Document13 pagesThe Department of Ethnography: Reading Passage 1mujeebNo ratings yet
- Bilirubin BR2 DatasheetDocument4 pagesBilirubin BR2 DatasheetCao Minh TríNo ratings yet
- Tips On UpcatDocument5 pagesTips On UpcatAira Mae AloverosNo ratings yet
- CHAPTER 6 - HOMEWORK - With KeyDocument8 pagesCHAPTER 6 - HOMEWORK - With KeyVõ Ngọc HânNo ratings yet
- Iit Hybrid ScheduleDocument3 pagesIit Hybrid ScheduleAdithyan CANo ratings yet

























































































Download as pdf or txt
You might also like
- Separation Process Engineering Includes Mass Transfer Analysis 4th Edition Wankat Solution ManualDocument54 pagesSeparation Process Engineering Includes Mass Transfer Analysis 4th Edition Wankat Solution Manualjacob100% (31)
- Hose Products and Tooling Guide 8th EditionDocument332 pagesHose Products and Tooling Guide 8th EditionKeron Trotz100% (4)
- #128 - Harvie - 2021 - Discrimination - Training - Neck - Pain - ProtocolDocument7 pages#128 - Harvie - 2021 - Discrimination - Training - Neck - Pain - ProtocolsoylahijadeunvampiroNo ratings yet
- Effects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialDocument14 pagesEffects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialLorena Rico ArtigasNo ratings yet
- The Relationship Between Rate of Algometer Application and Pain Pressure Threshold in TheDocument16 pagesThe Relationship Between Rate of Algometer Application and Pain Pressure Threshold in TheRafael BohnenbergerNo ratings yet
- RetrieveDocument9 pagesRetrieveSuttinont SurapuchongNo ratings yet
- Comparison of The Effects Between Lasers AppliedDocument29 pagesComparison of The Effects Between Lasers AppliedHelena GaribottiNo ratings yet
- 2015 - Article - 665eficacia EpicondilitiDocument13 pages2015 - Article - 665eficacia EpicondilitimorbreirNo ratings yet
- Bowen Back Pain WSN-93-2018-81-94Document14 pagesBowen Back Pain WSN-93-2018-81-94Saleha TariqNo ratings yet
- 2016 Article 653Document20 pages2016 Article 653CaioSelaimenNo ratings yet
- 904nm 0.6W - 12663 - 2013 - Article - 544Document7 pages904nm 0.6W - 12663 - 2013 - Article - 544Gino DammiuncrodinoNo ratings yet
- Disability and Related Factors in Patients With Chronic Cervical Myofascial PainDocument8 pagesDisability and Related Factors in Patients With Chronic Cervical Myofascial Painaria tristayanthiNo ratings yet
- 2015 Sensorimotor Control in The Hand As An Outcome IndicatorDocument12 pages2015 Sensorimotor Control in The Hand As An Outcome IndicatorClaudia Chinchilla ZeceñaNo ratings yet
- Poster PapersDocument262 pagesPoster PapersLeonardo RodríguezNo ratings yet
- JCM 08 00051 v2Document7 pagesJCM 08 00051 v2joelruizmaNo ratings yet
- Efficacy of Repetitive Transcranial Magnetic StimuDocument28 pagesEfficacy of Repetitive Transcranial Magnetic Stimuluz elena guerraNo ratings yet
- 2 Ijpotdec20172Document10 pages2 Ijpotdec20172TJPRC PublicationsNo ratings yet
- Buyukturan 2018Document8 pagesBuyukturan 2018Eka BagaskaraNo ratings yet
- Comparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDocument29 pagesComparison Between Outcomes of Dry Needling With Conventional Protocol and Rood's Approach With Conventional Protocol On Pain, Strength and Balance in Knee OsteoarthritisDrPratibha SinghNo ratings yet
- Park 2014Document7 pagesPark 2014Nurfitrianti ArfahNo ratings yet
- Observational Pilot Study of Patients With Carpal Tunnel Syndrome Treated With Nucleo CMP ForteDocument8 pagesObservational Pilot Study of Patients With Carpal Tunnel Syndrome Treated With Nucleo CMP ForteRicardo BarcoNo ratings yet
- 16 Van Leerdam Et Al J Hand Surg Eur Vol. 2017 Jun 42 5 501 506 AAMDocument13 pages16 Van Leerdam Et Al J Hand Surg Eur Vol. 2017 Jun 42 5 501 506 AAMChristopher Freddy Bermeo RiveraNo ratings yet
- Effect of Positional Release Technique in Subjects With Subacute TrapezitisDocument9 pagesEffect of Positional Release Technique in Subjects With Subacute TrapezitisijphyNo ratings yet
- J Jpain 2012 01 047Document1 pageJ Jpain 2012 01 047adssaNo ratings yet
- Functional Outcome of Carpal Tunnel Syndrome After Exercise Versus Ultrasound DiathermyDocument8 pagesFunctional Outcome of Carpal Tunnel Syndrome After Exercise Versus Ultrasound DiathermyAdelia 102013330No ratings yet
- Research Paper 1Document14 pagesResearch Paper 1Ayesha HabibNo ratings yet
- Full TextDocument7 pagesFull TextJuan Pablo Casanova AnguloNo ratings yet
- Bmjopen 2021 051073Document12 pagesBmjopen 2021 051073Eugênio AraújoNo ratings yet
- Chen 2013Document5 pagesChen 2013RenaldiPrimaSaputraNo ratings yet
- Grossnickle Literature Review PaperDocument8 pagesGrossnickle Literature Review Paperapi-627301337No ratings yet
- Extracorporeal Shock Wave Therapy VersusDocument7 pagesExtracorporeal Shock Wave Therapy VersusGiannis SaramantosNo ratings yet
- Effect of Manual Therapy and Neurodynamic Techniques VsDocument10 pagesEffect of Manual Therapy and Neurodynamic Techniques VsTomBramboNo ratings yet
- 2408 2413Document6 pages2408 2413Anandhu GNo ratings yet
- Researcharticle Open Access: Philipp Wälti, Jan Kool and Hannu LuomajokiDocument11 pagesResearcharticle Open Access: Philipp Wälti, Jan Kool and Hannu LuomajokiRoaa MansourNo ratings yet
- Dunning James Et AlDocument10 pagesDunning James Et Alapi-290796947No ratings yet
- Randomizado-Us Pulsado e Fono em Tunel Do CarpoDocument9 pagesRandomizado-Us Pulsado e Fono em Tunel Do CarpoELONo ratings yet
- Medicina 58 01332Document27 pagesMedicina 58 01332Putu DeaNo ratings yet
- Lopez 2021Document9 pagesLopez 2021toaldoNo ratings yet
- MJCU - Volume 88 - Issue September - Pages 1601-1614Document9 pagesMJCU - Volume 88 - Issue September - Pages 1601-1614fomoNo ratings yet
- CBMT and NTDocument11 pagesCBMT and NTrizkiriasariNo ratings yet
- Chronic Ankle InstabilityDocument9 pagesChronic Ankle InstabilityJonathan Elias Barrientos OssesNo ratings yet
- 2015 LeeDocument3 pages2015 LeeJavier PelaezNo ratings yet
- 2019-Prolotherapy-Vs-Eswt-For-Lateral-Epicondylosis VS ONDAS DE CHOQUEDocument5 pages2019-Prolotherapy-Vs-Eswt-For-Lateral-Epicondylosis VS ONDAS DE CHOQUEDuilio GuzzardoNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- Cognitive Impairment 3 Months After Moderate and Severe Traumatic Brain Injury: A Prospective Follow-Up StudyDocument10 pagesCognitive Impairment 3 Months After Moderate and Severe Traumatic Brain Injury: A Prospective Follow-Up StudyIngrid Nayibe Díaz EspinosaNo ratings yet
- 1 s2.0 S0020138320310548 MainDocument7 pages1 s2.0 S0020138320310548 MainAURORA BADIALINo ratings yet
- FFT®: Functional Fascial Taping®Document5 pagesFFT®: Functional Fascial Taping®BwizerNo ratings yet
- Hypoesthesia Associated With Mandibular Movement After Sagittal Split Ramus OsteotomyDocument7 pagesHypoesthesia Associated With Mandibular Movement After Sagittal Split Ramus OsteotomyBruno ManNo ratings yet
- SSRN Id3705177Document222 pagesSSRN Id3705177Paula Heline NisanshaNo ratings yet
- Reduction of Spontaneous Electrical Activity and Pain Perception of Trigger Points in The Upper Trapezius Muscle Through Trigger Point Compression and Passive StretchingDocument13 pagesReduction of Spontaneous Electrical Activity and Pain Perception of Trigger Points in The Upper Trapezius Muscle Through Trigger Point Compression and Passive StretchingKapil SharmaNo ratings yet
- Articulo BrasileroDocument8 pagesArticulo BrasileroLuis GalvanNo ratings yet
- A Deep Neural Network-Based Pain Classifier Using A Photoplethysmography SignalDocument16 pagesA Deep Neural Network-Based Pain Classifier Using A Photoplethysmography SignalPING KWAN MANNo ratings yet
- ScientificDocument4 pagesScientificKiran AbidNo ratings yet
- 410 4225 PDFDocument5 pages410 4225 PDFmilhimNo ratings yet
- Comparing The Effects of Manual Therapy Versus Electrophysical Agents in The Management of Knee OsteoarthritisDocument4 pagesComparing The Effects of Manual Therapy Versus Electrophysical Agents in The Management of Knee OsteoarthritisNurul MuslihahNo ratings yet
- Tendon 2Document10 pagesTendon 2Verónica Téllez ArriagaNo ratings yet
- Paper 4Document13 pagesPaper 4Pablo Cuevas SaldivarNo ratings yet
- Osteopathic Manipulation Treatment Versus Therapeutic Exercises in Patients With Chronic Nonspecific Low Back PainDocument11 pagesOsteopathic Manipulation Treatment Versus Therapeutic Exercises in Patients With Chronic Nonspecific Low Back PainBruno AssunçaoNo ratings yet
- Temporomandibular DisordersDocument8 pagesTemporomandibular DisordersItzel VargasNo ratings yet
- Palpation of The Lateral Pterygoid Area in The Myofascial Pain DiagnosisDocument6 pagesPalpation of The Lateral Pterygoid Area in The Myofascial Pain Diagnosisdavidcosmin186832No ratings yet
- Clinical Gait Assessment in The Neurologically ImpairedDocument6 pagesClinical Gait Assessment in The Neurologically Impairedvamat63No ratings yet
- Neuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodFrom EverandNeuroscientific based therapy of dysfunctional cognitive overgeneralizations caused by stimulus overload with an "emotionSync" methodNo ratings yet
- Mt4gui CheatsheetDocument2 pagesMt4gui Cheatsheetbinosp2No ratings yet
- Us0ab 21023133 21023133Document1 pageUs0ab 21023133 21023133krish.gkavarapuNo ratings yet
- Fintech Adoption and Its Impact On Sustainability: Risk Benefit Analysis of An Emerging EconomyDocument32 pagesFintech Adoption and Its Impact On Sustainability: Risk Benefit Analysis of An Emerging EconomyAudit and Accounting ReviewNo ratings yet
- DC Circuit Breakers:: An Important Role in The Continuity and Quality of ServiceDocument3 pagesDC Circuit Breakers:: An Important Role in The Continuity and Quality of ServiceSagar GadhiaNo ratings yet
- GogugugDocument2 pagesGogugugvipin kumarNo ratings yet
- Senior HighschoolDocument3 pagesSenior HighschoolAngelica MathewNo ratings yet
- TimkooDocument1 pageTimkooAli HabibNo ratings yet
- Philippine LiteratureDocument26 pagesPhilippine LiteratureCierly Mae TantanNo ratings yet
- Advancements in Weft Knitting TechnologyDocument28 pagesAdvancements in Weft Knitting TechnologyAbhi Sheikh100% (1)
- 1246 SP 4 Emm 24003 B2Document132 pages1246 SP 4 Emm 24003 B2Arash Aghagol100% (1)
- Suzuki Ertiga p1-26Document26 pagesSuzuki Ertiga p1-26bonruiz100% (2)
- CEM130 Construction Safety Management - SYLLABUS RevisedDocument5 pagesCEM130 Construction Safety Management - SYLLABUS Reviseddel rosarioNo ratings yet
- CH 19 Cash and Liquidity Management Appendix Class WorkDocument4 pagesCH 19 Cash and Liquidity Management Appendix Class WorkMhmd KaramNo ratings yet
- Introduction To Copulas: Mark S. Tenney Mathematical Finance Company July 18, 2003Document9 pagesIntroduction To Copulas: Mark S. Tenney Mathematical Finance Company July 18, 2003Mario CruzNo ratings yet
- Variable Valve Timing & Acoustic Control Induction Systems: Section 8Document19 pagesVariable Valve Timing & Acoustic Control Induction Systems: Section 8sungjoo75No ratings yet
- Us 1 NUM 10xx Series CNC Backup/ Restore Procedures Using NUMBackUp 14 10xx NUMBackupDocument3 pagesUs 1 NUM 10xx Series CNC Backup/ Restore Procedures Using NUMBackUp 14 10xx NUMBackupHa Pro50% (2)
- DCRM 6 Channel NewDocument9 pagesDCRM 6 Channel NewSayan ChatterjeeNo ratings yet
- Rajasthan Technical University, Kota: Syllabus 3 Year - V Semester: B.Tech.: Mechanical EngineeringDocument1 pageRajasthan Technical University, Kota: Syllabus 3 Year - V Semester: B.Tech.: Mechanical Engineeringsharad pareekNo ratings yet
- Ui22 Lab1Document5 pagesUi22 Lab1dattpatel2020No ratings yet
- Anfis (Adaptive Network Fuzzy Inference System) : G.AnuradhaDocument25 pagesAnfis (Adaptive Network Fuzzy Inference System) : G.Anuradhamodis777No ratings yet
- Inquiries, Investigation, and ImmersionDocument6 pagesInquiries, Investigation, and ImmersioniNo ratings yet
- English TestDocument5 pagesEnglish TestfabiolaNo ratings yet
- Gha Ba Ags531441-01 enDocument68 pagesGha Ba Ags531441-01 enRagab TolbaNo ratings yet
- The Department of Ethnography: Reading Passage 1Document13 pagesThe Department of Ethnography: Reading Passage 1mujeebNo ratings yet
- Bilirubin BR2 DatasheetDocument4 pagesBilirubin BR2 DatasheetCao Minh TríNo ratings yet
- Tips On UpcatDocument5 pagesTips On UpcatAira Mae AloverosNo ratings yet
- CHAPTER 6 - HOMEWORK - With KeyDocument8 pagesCHAPTER 6 - HOMEWORK - With KeyVõ Ngọc HânNo ratings yet
- Iit Hybrid ScheduleDocument3 pagesIit Hybrid ScheduleAdithyan CANo ratings yet