Download as docx, pdf, or txt
You might also like
- Medical-Surgical Drug ListDocument3 pagesMedical-Surgical Drug Listbarbara100% (1)
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- Physical Therapy AssessmentDocument38 pagesPhysical Therapy Assessmentnikki98% (56)
- Extra Exam Practice 2: Read The Text and Answer The Questions That FollowDocument2 pagesExtra Exam Practice 2: Read The Text and Answer The Questions That Follow.100% (1)
- Group Termination Shapiro2002Document19 pagesGroup Termination Shapiro2002bertie_bertolucciNo ratings yet
- 3 Transport GuideDocument13 pages3 Transport GuideИван МельникNo ratings yet
- Advanced Hypnotherapy Steve G Jones EbookDocument148 pagesAdvanced Hypnotherapy Steve G Jones EbookLeonardo Do Carmo82% (22)
- RBI-Vital-Signs-Wellness MassageDocument36 pagesRBI-Vital-Signs-Wellness Massagema.fatima ravalo rabulanNo ratings yet
- Vital SignsDocument47 pagesVital SignsSchneider JovellanoNo ratings yet
- Basic Health Care Skills: How To Measure Vital Signs Vital SignsDocument8 pagesBasic Health Care Skills: How To Measure Vital Signs Vital SignsJoan BarcenasNo ratings yet
- NCM 101 Health Assessment IiiDocument21 pagesNCM 101 Health Assessment IiiArrianne AbdonNo ratings yet
- Vital Sign Na (1) by ZWBDocument52 pagesVital Sign Na (1) by ZWBAshraf Ali100% (1)
- NSTP12 FinalDocument16 pagesNSTP12 FinalJhonny pingolNo ratings yet
- Vital Signs LectureDocument67 pagesVital Signs LectureJayrelle D. SafranNo ratings yet
- Group 5 Vital SignsDocument27 pagesGroup 5 Vital SignsGelique AnterolaNo ratings yet
- Health Assessment LectureDocument42 pagesHealth Assessment Lecturekc bpNo ratings yet
- NTILS GuideDocument11 pagesNTILS GuideNeil ThomasNo ratings yet
- Vital Signs: St. Scholastica's College Tacloban Maharlika Highway, Brgy. Campetic, Palo, Leyte College of NursingDocument33 pagesVital Signs: St. Scholastica's College Tacloban Maharlika Highway, Brgy. Campetic, Palo, Leyte College of NursingEVRMC ICSNo ratings yet
- Assesing A Casualty Vital SignsDocument19 pagesAssesing A Casualty Vital SignsCiedelle Honey Lou DimaligNo ratings yet
- AOP AdultDocument93 pagesAOP AdultKvothe EdemaRuhNo ratings yet
- Vitalsigns PDFDocument36 pagesVitalsigns PDFSuneel Kumar PrajapatiNo ratings yet
- Vital Signs LatestDocument56 pagesVital Signs LatestCriselda PabuaNo ratings yet
- Vital SignsDocument31 pagesVital Signstom10carandangNo ratings yet
- Vital SignsDocument5 pagesVital SignsSandara Delas PenasNo ratings yet
- Outline Vital SignsDocument4 pagesOutline Vital SignsDino MicaNo ratings yet
- 2) Vital SignsDocument7 pages2) Vital SignsJudy JalbunaNo ratings yet
- Vital SignsDocument24 pagesVital Signsma.fatima ravalo rabulanNo ratings yet
- Clinical Procedures For Medical AssistantDocument40 pagesClinical Procedures For Medical AssistantStudent1010No ratings yet
- Blood PressureDocument18 pagesBlood PressureChelsea BorgoniaNo ratings yet
- Pemeriksaan Tanda Vital-Kuliah PengantarDocument22 pagesPemeriksaan Tanda Vital-Kuliah PengantartrisiaNo ratings yet
- HA-RLE-WS # 5 Assessing General Status and Vital SignsDocument5 pagesHA-RLE-WS # 5 Assessing General Status and Vital SignsJULIE ANNE CORTEZ100% (1)
- Bicol University College of NursingDocument71 pagesBicol University College of NursingDanekka TanNo ratings yet
- CSI 101 Skills Lab 3 NotesDocument4 pagesCSI 101 Skills Lab 3 Notescampbellbritney8811856No ratings yet
- Vital-Signs 042951Document37 pagesVital-Signs 042951alyssaburgos02No ratings yet
- Radtech Vital SignsDocument49 pagesRadtech Vital SignsGEORGIE JANE LORENANo ratings yet
- NSTP1 Vital SignsDocument31 pagesNSTP1 Vital SignsCarmie CasañasNo ratings yet
- Module 2 Full SlidesDocument69 pagesModule 2 Full SlidesMaria Du-PastoralNo ratings yet
- Vital Sign PresentationDocument44 pagesVital Sign PresentationannabelleNo ratings yet
- Vital Signs NotesDocument7 pagesVital Signs NotesJustine Martinez AmoresNo ratings yet
- Vital Signs (BHW Training) 2Document31 pagesVital Signs (BHW Training) 2Yathziel Meow100% (4)
- Module 7 Taking Vital SignsDocument7 pagesModule 7 Taking Vital SignsMary Joy CejalboNo ratings yet
- Vital Signs and TestingDocument47 pagesVital Signs and TestingRegina Garrard100% (1)
- Physical ExaminationDocument32 pagesPhysical ExaminationCaroline AgathaNo ratings yet
- Course: Emergency Procedures and Patient Care Lecture-4Document27 pagesCourse: Emergency Procedures and Patient Care Lecture-4saba ramzanNo ratings yet
- 3 - Vital SignDocument27 pages3 - Vital SignBav VAansoqnuaetzNo ratings yet
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyNo ratings yet
- Newborn AssessmentDocument17 pagesNewborn Assessmentmarycris100% (3)
- VITAL SIGNS and Patient AssessmentDocument8 pagesVITAL SIGNS and Patient AssessmentHANNAH ANIVERSARIONo ratings yet
- RLE 2 - Lecture On Vital SignsDocument59 pagesRLE 2 - Lecture On Vital SignsIrah Joy MarianoNo ratings yet
- Vital SignsDocument5 pagesVital SignsFrances Kaye Sta. CruzNo ratings yet
- The Precise Neurological ExamDocument30 pagesThe Precise Neurological ExamZīshān FārūqNo ratings yet
- Vital SignsDocument2 pagesVital SignsAfril CadagNo ratings yet
- Vital Signs Final PDFDocument8 pagesVital Signs Final PDFJeanne IrishNo ratings yet
- MECA HandoutsDocument118 pagesMECA HandoutsJun JavierNo ratings yet
- Vital Signs 19Document26 pagesVital Signs 19LisetteNo ratings yet
- Vital SignsDocument55 pagesVital SignsArunesh 456No ratings yet
- Resume Vital Sign ExaminationDocument6 pagesResume Vital Sign ExaminationRedmy LasmanaNo ratings yet
- Vital Signs SabansiDocument116 pagesVital Signs SabansiTariku olanaNo ratings yet
- Lesson 2 NCM 101 Assessing Vital Signs and General StatusDocument5 pagesLesson 2 NCM 101 Assessing Vital Signs and General StatusbelgicasalveNo ratings yet
- Vital SignsDocument63 pagesVital SignsAlvin JavierNo ratings yet
- Blood Pressure: Step By Step Guide And Proven Recipes To Lower Your Blood Pressure Without Any MedicationFrom EverandBlood Pressure: Step By Step Guide And Proven Recipes To Lower Your Blood Pressure Without Any MedicationNo ratings yet
- Blood Pressure Monitoring Journal: A Hypertension Diary and LogFrom EverandBlood Pressure Monitoring Journal: A Hypertension Diary and LogNo ratings yet
- Ben ResumeDocument2 pagesBen ResumeJohana Pinagayao AngkadNo ratings yet
- EO BCPC No. 4,2019Document2 pagesEO BCPC No. 4,2019Johana Pinagayao AngkadNo ratings yet
- CP111 Module 2 (Whole)Document35 pagesCP111 Module 2 (Whole)Johana Pinagayao AngkadNo ratings yet
- Module-In-In-Foundation-Of-Special-And-Inclusive-Education - Pdf-FreeDocument13 pagesModule-In-In-Foundation-Of-Special-And-Inclusive-Education - Pdf-FreeJohana Pinagayao AngkadNo ratings yet
- CP111 Module WS1 (Whole)Document20 pagesCP111 Module WS1 (Whole)Johana Pinagayao AngkadNo ratings yet
- Deparment of EducationDocument13 pagesDeparment of EducationJohana Pinagayao AngkadNo ratings yet
- CP111 Module PP1 (Whole)Document36 pagesCP111 Module PP1 (Whole)Johana Pinagayao AngkadNo ratings yet
- Application LetterDocument1 pageApplication LetterJohana Pinagayao AngkadNo ratings yet
- CROPROTDocument5 pagesCROPROTJohana Pinagayao AngkadNo ratings yet
- Blank ML CERTIFICATIONDocument1 pageBlank ML CERTIFICATIONJohana Pinagayao AngkadNo ratings yet
- Affidavit of AbandonmentDocument1 pageAffidavit of AbandonmentJohana Pinagayao AngkadNo ratings yet
- Affidavit of AbandonmentDocument2 pagesAffidavit of AbandonmentJohana Pinagayao AngkadNo ratings yet
- Distribution PayrollDocument9 pagesDistribution PayrollJohana Pinagayao AngkadNo ratings yet
- Sample Cbjip Book of Barangay Kauswagan 1Document38 pagesSample Cbjip Book of Barangay Kauswagan 1Johana Pinagayao AngkadNo ratings yet
- EO No. 5 BCPCDocument2 pagesEO No. 5 BCPCJohana Pinagayao AngkadNo ratings yet
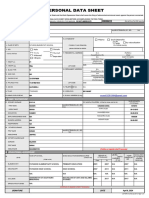
- Samsia PDSDocument4 pagesSamsia PDSJohana Pinagayao AngkadNo ratings yet
- Chapter 4 5Document13 pagesChapter 4 5Johana Pinagayao AngkadNo ratings yet
- Funda ReviewerDocument3 pagesFunda ReviewerJohana Pinagayao AngkadNo ratings yet
- Michael Sanday AboDocument1 pageMichael Sanday AboJohana Pinagayao AngkadNo ratings yet
- Black and White Minimalist High School English Teacher ResumeDocument1 pageBlack and White Minimalist High School English Teacher ResumeJohana Pinagayao AngkadNo ratings yet
- Entomology FinalDocument224 pagesEntomology FinalJohana Pinagayao AngkadNo ratings yet
- PapangDocument1 pagePapangJohana Pinagayao AngkadNo ratings yet
- EO No. 13 BHRACTDocument2 pagesEO No. 13 BHRACTJohana Pinagayao AngkadNo ratings yet
- Intro-2-1-1-3-1-3 KabacanDocument1 pageIntro-2-1-1-3-1-3 KabacanJohana Pinagayao AngkadNo ratings yet
- Final Week 17 18Document13 pagesFinal Week 17 18Johana Pinagayao AngkadNo ratings yet
- BCPC Over PictureDocument1 pageBCPC Over PictureJohana Pinagayao AngkadNo ratings yet
- Final Week 15 16Document13 pagesFinal Week 15 16Johana Pinagayao AngkadNo ratings yet
- Prefinal Week 11Document9 pagesPrefinal Week 11Johana Pinagayao AngkadNo ratings yet
- Nutrition Management CancerDocument5 pagesNutrition Management CancerkitsilcNo ratings yet
- Caduet (Dr. Ismahun Maret 2009)Document41 pagesCaduet (Dr. Ismahun Maret 2009)Yulia SumarnaNo ratings yet
- PCC EasamcDocument22 pagesPCC EasamchusnaNo ratings yet
- Re Education of MusclesDocument41 pagesRe Education of MusclesMohamed Magdy El Meligie0% (3)
- Accuracy Thessaly TestDocument52 pagesAccuracy Thessaly TestC Martin Traumato100% (2)
- Escvs Full Program For Vacular SessionDocument7 pagesEscvs Full Program For Vacular SessionJelenaJadzicNo ratings yet
- Long-Term Efficacy of Percutaneous Steroid Injection For Treating Benign Vocal Fold Lesions: A Prospective StudyDocument5 pagesLong-Term Efficacy of Percutaneous Steroid Injection For Treating Benign Vocal Fold Lesions: A Prospective StudyWahyu JuliandaNo ratings yet
- Clinical AutopsyDocument20 pagesClinical AutopsyKim_b_Serac_6246No ratings yet
- HCC Computation ManualDocument195 pagesHCC Computation Manualykbhaumik123No ratings yet
- Post Partum Hemorrhage Nursing Care Plan PDFDocument2 pagesPost Partum Hemorrhage Nursing Care Plan PDFA sison100% (1)
- Lip LesionsDocument59 pagesLip Lesionspasser by100% (1)
- Simon Nuari Sitorus: ProfileDocument1 pageSimon Nuari Sitorus: ProfilehanaNo ratings yet
- Anemia in Older AdultsDocument8 pagesAnemia in Older AdultsStalin ViswanathanNo ratings yet
- Slide Fraktur FemurDocument26 pagesSlide Fraktur FemurMarhama FitrianiNo ratings yet
- Directions:: Read The Following Passage Carefully and Answer TheDocument22 pagesDirections:: Read The Following Passage Carefully and Answer Thepavankumar1313No ratings yet
- Post in GlycoDocument4 pagesPost in GlycoSA SHNo ratings yet
- Judicial Affidavit Preliminary StatementDocument5 pagesJudicial Affidavit Preliminary StatementVanessa GerodiasNo ratings yet
- Waiver/Blood Donor'S Consent: National Service Training Program (NSTP) OfficeDocument4 pagesWaiver/Blood Donor'S Consent: National Service Training Program (NSTP) OfficeMayra MerczNo ratings yet
- Apa Itu MengikDocument2 pagesApa Itu MengikAmy Tryabto ArifinNo ratings yet
- NCP CKD From CaneDocument74 pagesNCP CKD From CaneSheela Khrystyn LeeNo ratings yet
- Chap 20 LeadershipDocument4 pagesChap 20 LeadershipklossmaddyNo ratings yet
- Arrhythmias: Terminology, Definitions, and MechanismsDocument16 pagesArrhythmias: Terminology, Definitions, and MechanismshazelelNo ratings yet
- Gram Staining Guest Lecture JIPMER PondcherryDocument75 pagesGram Staining Guest Lecture JIPMER Pondcherrytummalapalli venkateswara raoNo ratings yet
- Apnea of PrematurityDocument8 pagesApnea of PrematuritypatriaindraNo ratings yet
- Community Acquired Pneumonia, Lancet, 12-03Document11 pagesCommunity Acquired Pneumonia, Lancet, 12-03Maya ramadaniNo ratings yet