Download as pdf or txt
You might also like
- Massive MIMO Detection Algorithm and VLSI Architecture 2019 PDFDocument348 pagesMassive MIMO Detection Algorithm and VLSI Architecture 2019 PDFdupipiNo ratings yet
- Bapineuzumab For Mild To Moderate Alzheimer 'S Disease in Two Global, Randomized, Phase 3 TrialsDocument13 pagesBapineuzumab For Mild To Moderate Alzheimer 'S Disease in Two Global, Randomized, Phase 3 TrialsRoza EtlaboraNo ratings yet
- 1 s2.0 S2352873716300166 Main PDFDocument8 pages1 s2.0 S2352873716300166 Main PDFChalisa ThamdamrongNo ratings yet
- 81635793Document13 pages81635793Brock TernovNo ratings yet
- Lecanemab SubmDocument21 pagesLecanemab SubmHenrique OliveiraNo ratings yet
- Jca 38 45Document10 pagesJca 38 45filianalefaanNo ratings yet
- Anti Amyloid Monoclonal Antibodies For The Treatment of Alzheimer's DiseaseDocument18 pagesAnti Amyloid Monoclonal Antibodies For The Treatment of Alzheimer's DiseasegunarodeoliveiraNo ratings yet
- Amyloid Vaccine For Alzheimer's Disease - Is It Feasible by Supreet Khare, Deeksha Seth, Shrayash KhareDocument4 pagesAmyloid Vaccine For Alzheimer's Disease - Is It Feasible by Supreet Khare, Deeksha Seth, Shrayash Khareijr_journalNo ratings yet
- Jpad 2022 30Document14 pagesJpad 2022 30lujiexu94No ratings yet
- IVIgG AmiloidDocument4 pagesIVIgG AmiloidyinvilllNo ratings yet
- OPERA OcrelizumabDocument14 pagesOPERA OcrelizumabalmarazneurologiaNo ratings yet
- Utilizing Targeted Gene Therapy With Nano Particles Binding Alpha V Beta 3 For Imaging and Treating Choroidal NeovascularizationDocument9 pagesUtilizing Targeted Gene Therapy With Nano Particles Binding Alpha V Beta 3 For Imaging and Treating Choroidal Neovascularizationtennisboy92No ratings yet
- Proceedings of The Anaesthetic Research Society Meeting: AbstractsDocument13 pagesProceedings of The Anaesthetic Research Society Meeting: AbstractsrYanDYNo ratings yet
- 1 s2.0 S2666990024000181 MainDocument9 pages1 s2.0 S2666990024000181 MaintrendyternaitesNo ratings yet
- Advocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Document2 pagesAdvocating For Demonstration of Disease Modification - Have We Been Approaching Clinical Trials in Early Alzheimer Disease Incorrectly?Lorrane NevesNo ratings yet
- Nejmoa 2211023Document10 pagesNejmoa 2211023EvelynNo ratings yet
- Van Dyck 2017 - Anti-AB Monoclonar Antibodies For ADDocument9 pagesVan Dyck 2017 - Anti-AB Monoclonar Antibodies For ADljdNo ratings yet
- Fourth International Conference On Alzheimer'S Disease s137Document2 pagesFourth International Conference On Alzheimer'S Disease s137Sergiy Prokofiy MontanoNo ratings yet
- Clinical Characteristics and PDocument10 pagesClinical Characteristics and Pmiss betawiNo ratings yet
- Beta Blockers and AsthmaDocument8 pagesBeta Blockers and AsthmaAzmachamberAzmacareNo ratings yet
- Biodistribution of Drug/ADA Complexes: The Impact of Immune Complex Formation On Antibody DistributionDocument12 pagesBiodistribution of Drug/ADA Complexes: The Impact of Immune Complex Formation On Antibody Distributiongskcl429No ratings yet
- Bittner 2016 AlzDemDocument10 pagesBittner 2016 AlzDemnour abdallaNo ratings yet
- Biologics in Chronic UrticariaDocument18 pagesBiologics in Chronic UrticariaRohit GuptaNo ratings yet
- Impact of Anti-Amyloid-b Monoclonal Antibodies On The Pathology and Clinical Profile of Alzheimer's Disease - A Focus On Aducanumab and LecanemabDocument11 pagesImpact of Anti-Amyloid-b Monoclonal Antibodies On The Pathology and Clinical Profile of Alzheimer's Disease - A Focus On Aducanumab and LecanemabPau Fer Mujica CNo ratings yet
- Articulo Nanomedicina AlzheimerDocument15 pagesArticulo Nanomedicina AlzheimerAdriana LópezNo ratings yet
- Articol McsDocument14 pagesArticol McsMari NiculaeNo ratings yet
- Human Loiasis in A Cameroonian Village A Double-Blind, Placebo-Controlled, Crossover Clinical Trial of Athree-Day Albendazole RegimenDocument5 pagesHuman Loiasis in A Cameroonian Village A Double-Blind, Placebo-Controlled, Crossover Clinical Trial of Athree-Day Albendazole RegimenLucchéri Ndong AkomezogheNo ratings yet
- Journal Club EdavaroneDocument5 pagesJournal Club EdavaroneJohn Christopher RuizNo ratings yet
- Gold Nanoparticles Enhance Antibody Effect Through Direct Cancer Cell Cytotoxicity by Differential Regulation of PhagocytosisDocument13 pagesGold Nanoparticles Enhance Antibody Effect Through Direct Cancer Cell Cytotoxicity by Differential Regulation of PhagocytosistobyNo ratings yet
- Perspective Is Therapeutic Plasma Exchange A Viable Option For TreatingDocument11 pagesPerspective Is Therapeutic Plasma Exchange A Viable Option For TreatingRaul Rios RitterNo ratings yet
- FPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseDocument2 pagesFPTP - Amoxicillin - Clavulanic Acid in Cats With & Without Chronic Kidney DiseaseMabe AguirreNo ratings yet
- AlzheimerDocument19 pagesAlzheimerNET-AVÓNo ratings yet
- Daftar PustakaDocument16 pagesDaftar PustakaDestrie CindyNo ratings yet
- NIH Public Access: Two Phase 3 Trials of Bapineuzumab in Mild-to-Moderate Alzheimer's DiseaseDocument18 pagesNIH Public Access: Two Phase 3 Trials of Bapineuzumab in Mild-to-Moderate Alzheimer's DiseaseNaufal NanditaNo ratings yet
- RCT Simvastatin AlzheimerDocument8 pagesRCT Simvastatin AlzheimerGabriel Septiana CitraNo ratings yet
- Cyclosporine For Moderate-To-Severe Alopecia Areata: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial of Efficacy and SafetyDocument8 pagesCyclosporine For Moderate-To-Severe Alopecia Areata: A Double-Blind, Randomized, Placebo-Controlled Clinical Trial of Efficacy and Safetysupaidi97No ratings yet
- 10.1016@S1575 09220970841 1Document5 pages10.1016@S1575 09220970841 1ririsNo ratings yet
- 2014 WangDocument10 pages2014 WangJosé Messias PerdigãoNo ratings yet
- 15 Sheline YI West TDocument9 pages15 Sheline YI West Tihsan fadhilahNo ratings yet
- J 1468-1331 2010 03092 XDocument10 pagesJ 1468-1331 2010 03092 XLauri VergaraNo ratings yet
- Autoantibodies Alzheimer Disease.1Document9 pagesAutoantibodies Alzheimer Disease.1MARIA DE FATIMA TEIXEIRA GORDILLONo ratings yet
- Liu 2020Document6 pagesLiu 2020Andra CismaruNo ratings yet
- 2019 - High-Resolution Metabolomic Profiling of Alzheimer's PDFDocument10 pages2019 - High-Resolution Metabolomic Profiling of Alzheimer's PDFEva Sánchez YébenesNo ratings yet
- 5 - 2016 LpADocument10 pages5 - 2016 LpAjef5525No ratings yet
- Ac Anti AdaDocument7 pagesAc Anti AdaAndreea RacovitaNo ratings yet
- Biomedicines 05 00017Document13 pagesBiomedicines 05 00017Nilton MafraNo ratings yet
- 1 s2.0 S0168827804905533 MainDocument1 page1 s2.0 S0168827804905533 Maindjafer maryaNo ratings yet
- 2020 Boada A Randomized Controlled Clinical Trial of Plasma Exchange With Albumin ReplacementDocument14 pages2020 Boada A Randomized Controlled Clinical Trial of Plasma Exchange With Albumin ReplacementFranc DechiaNo ratings yet
- Dkab 413Document9 pagesDkab 413wiwiNo ratings yet
- Donanemab in Early Alzheimer's Disease: Original ArticleDocument14 pagesDonanemab in Early Alzheimer's Disease: Original ArticleBalla ElkhiderNo ratings yet
- 66 68 PBDocument89 pages66 68 PBAyesha FatimaNo ratings yet
- Repurposing of Kinase Inhibitors To Target C-Abl As PotentialDocument10 pagesRepurposing of Kinase Inhibitors To Target C-Abl As PotentialShreeya BhatNo ratings yet
- Mechanism of Amyloid Removal in Patients With Gantenerumab (Roche Mab) - Oct 2011Document10 pagesMechanism of Amyloid Removal in Patients With Gantenerumab (Roche Mab) - Oct 2011sckeddyNo ratings yet
- 1 - Ascorbate X Cancer PaperDocument5 pages1 - Ascorbate X Cancer PaperFazisvaldo PimentãoNo ratings yet
- Cardiovascular Safety of Naltrexone and Bupropion Therapy Systematic Review and Meta-AnalysesDocument9 pagesCardiovascular Safety of Naltrexone and Bupropion Therapy Systematic Review and Meta-AnalysesPlinio ReisNo ratings yet
- The Amyloid-β Pathway in Alzheimer's Disease. Molecular PsychiatryDocument23 pagesThe Amyloid-β Pathway in Alzheimer's Disease. Molecular Psychiatryanggi abNo ratings yet
- Shin - 2019 - AB Oligomers Promote Uptake TauDocument13 pagesShin - 2019 - AB Oligomers Promote Uptake TauTibor SzénásiNo ratings yet
- Baclofen For Alcohol Withdrawal.: Liu J Wang LNDocument5 pagesBaclofen For Alcohol Withdrawal.: Liu J Wang LNVivekNo ratings yet
- Small Interfering RNA To ReduceDocument10 pagesSmall Interfering RNA To ReduceMahmoud Abu MayalehNo ratings yet
- Comparing Low Vs High Dose CFDocument12 pagesComparing Low Vs High Dose CFLarissa RodNo ratings yet
- MWM Post Treatment 18mo APP: WT Veh WT PBN TG Veh TG PBNDocument1 pageMWM Post Treatment 18mo APP: WT Veh WT PBN TG Veh TG PBNPau Fer Mujica CNo ratings yet
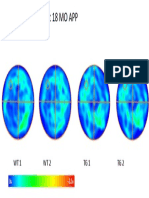
- MWM Pre Treatment 18 MO APP: WT1 WT2 TG1 TG2Document1 pageMWM Pre Treatment 18 MO APP: WT1 WT2 TG1 TG2Pau Fer Mujica CNo ratings yet
- MWM Post Treatment 3mo APP: WT Veh WT PBN TG Veh TG PBNDocument1 pageMWM Post Treatment 3mo APP: WT Veh WT PBN TG Veh TG PBNPau Fer Mujica CNo ratings yet
- NOR Post Treatment 18mo APP: WT Veh TG Veh TG PBN WT PBNDocument1 pageNOR Post Treatment 18mo APP: WT Veh TG Veh TG PBN WT PBNPau Fer Mujica CNo ratings yet
- MWM Pre Treatment 12mo APP: WT Veh TG VehDocument1 pageMWM Pre Treatment 12mo APP: WT Veh TG VehPau Fer Mujica CNo ratings yet
- 15.2.1. A, P, B R: Nesthesia Erfusion AND Rain EmovalDocument6 pages15.2.1. A, P, B R: Nesthesia Erfusion AND Rain EmovalPau Fer Mujica CNo ratings yet
- Proyecto de Tesis - Nicole SanguinettiDocument26 pagesProyecto de Tesis - Nicole SanguinettiPau Fer Mujica CNo ratings yet
- The Impact On Synaptic Transmission by Removal of Endocannabinoid Signaling in Specific NeuronsDocument6 pagesThe Impact On Synaptic Transmission by Removal of Endocannabinoid Signaling in Specific NeuronsPau Fer Mujica CNo ratings yet
- Hand Out MEOW PHYF111Document3 pagesHand Out MEOW PHYF111Shreya GuptaNo ratings yet
- Manda FreqDocument539 pagesManda FreqTom StNo ratings yet
- DCEM-21xx BrochureDocument4 pagesDCEM-21xx BrochureApply Softtech100% (1)
- L-s20 Specification For Road Lighting InstallationDocument82 pagesL-s20 Specification For Road Lighting Installationzamanhuri junidNo ratings yet
- Research Report - Aakanksha MistryDocument19 pagesResearch Report - Aakanksha MistryAakanksha MistryNo ratings yet
- Hazardous Areas - Explosionproof Solenoids: Some HistoryDocument5 pagesHazardous Areas - Explosionproof Solenoids: Some HistoryShahram GhassemiNo ratings yet
- Physics 158 Final Exam Review Package: UBC Engineering Undergraduate SocietyDocument22 pagesPhysics 158 Final Exam Review Package: UBC Engineering Undergraduate SocietySpam MailNo ratings yet
- Dopamine D23 Receptor Antagonism Reduces Activity-Based AnorexiaDocument10 pagesDopamine D23 Receptor Antagonism Reduces Activity-Based AnorexiaJeffery TaylorNo ratings yet
- The Summer Internship at Limited: Hindustan AeronauticsDocument59 pagesThe Summer Internship at Limited: Hindustan AeronauticsAbhishek StarkNo ratings yet
- Basic Troubleshooting CLARKDocument21 pagesBasic Troubleshooting CLARKRaul E. SoliNo ratings yet
- Siskyou Bombing RangeDocument114 pagesSiskyou Bombing RangeCAP History LibraryNo ratings yet
- Reinforcement PADDocument13 pagesReinforcement PADamr al yacoubNo ratings yet
- 3F4 Error Control Coding: Dr. I. J. WassellDocument70 pages3F4 Error Control Coding: Dr. I. J. WassellgpaswathyNo ratings yet
- ISO 00426-1-1983 ScanDocument5 pagesISO 00426-1-1983 ScanthangNo ratings yet
- Dampak Bencana Alam Bagi Sektor Pariwisata Di Bali Ni Ketut Sutrisnawati AKPAR DenpasarDocument10 pagesDampak Bencana Alam Bagi Sektor Pariwisata Di Bali Ni Ketut Sutrisnawati AKPAR DenpasarRihar KoharNo ratings yet
- CitoVac EnglishDocument32 pagesCitoVac EnglishJulio C. Sierra PalominoNo ratings yet
- Edubba A Composite Text Ver3Document7 pagesEdubba A Composite Text Ver3RicardoNo ratings yet
- Budget of Work in Mathematics IIIDocument7 pagesBudget of Work in Mathematics IIIWehn LustreNo ratings yet
- Biological Bases of BehaviorDocument7 pagesBiological Bases of BehaviorSANTHOSH KUMAR T MNo ratings yet
- Variables On Both Sides of EquationsDocument17 pagesVariables On Both Sides of EquationsShatakshi DixitNo ratings yet
- CASE REPORT On OsteomyelitisDocument30 pagesCASE REPORT On OsteomyelitisNirbhay KatiyarNo ratings yet
- Composite EbookDocument285 pagesComposite Ebooksunilas218408100% (1)
- Catalytic Properties of Silver Nanoparticles Supported On Silica SpheresDocument6 pagesCatalytic Properties of Silver Nanoparticles Supported On Silica SpheresEduarddo Ravelo NietoNo ratings yet
- Biology Q & A Booklet: (English Medium)Document76 pagesBiology Q & A Booklet: (English Medium)La EscenaNo ratings yet
- Perform-3d-V5 0 0Document15 pagesPerform-3d-V5 0 0Darley MauricioNo ratings yet
- Dwaraka Nadh K: Mobile:8504080654,8500353334Document3 pagesDwaraka Nadh K: Mobile:8504080654,8500353334anon_396084846No ratings yet
- Ácido Sulfurico Ligas CompatíveisDocument2 pagesÁcido Sulfurico Ligas CompatíveisGuilherme Augusto de OliveiraNo ratings yet
- B-Housing and Living - 1Document2 pagesB-Housing and Living - 1Štěpánka OndrůškováNo ratings yet
- The Stall Chart - Varying Flow Secondary - Constant Inlet Temperature - Constant Outlet TemperatureDocument8 pagesThe Stall Chart - Varying Flow Secondary - Constant Inlet Temperature - Constant Outlet TemperatureSandra FerrellNo ratings yet