
Critical CHD
Critical CHD
You might also like
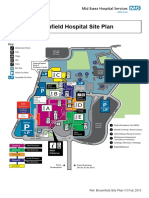
- Broomfield Hospital Site Plan: Café Shops Lifts Information PointsDocument1 pageBroomfield Hospital Site Plan: Café Shops Lifts Information Pointsady trader0% (2)
- Project Proposal On Dairy FarmDocument26 pagesProject Proposal On Dairy Farmvector dairy88% (8)
- 557-Assign 2-Action Plan For Culturally-Diverse School ClimateDocument10 pages557-Assign 2-Action Plan For Culturally-Diverse School Climateapi-566276833No ratings yet
- Cardiovascular DisorderDocument88 pagesCardiovascular DisorderSandeepNo ratings yet
- Pedia Cardiology 2Document5 pagesPedia Cardiology 2Medisina101No ratings yet
- Congenital Heart Disease: Education and Practice GapsDocument18 pagesCongenital Heart Disease: Education and Practice GapsAlvaro Ignacio Lagos SuilNo ratings yet
- Anesthesia For Noncardiac Surgery in Adults With Congenital Heart DiseaseDocument9 pagesAnesthesia For Noncardiac Surgery in Adults With Congenital Heart DiseaseIda Bagus MahendraNo ratings yet
- Congenital Heart Disease (2011)Document17 pagesCongenital Heart Disease (2011)drheay100% (1)
- Neonatal Cardiac EmergenciesDocument4 pagesNeonatal Cardiac EmergenciesEstellaNo ratings yet
- Tamizaje Enfermedades CardiacasDocument16 pagesTamizaje Enfermedades CardiacasDanna GonzálezNo ratings yet
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- Shunt Card Clin 2015Document8 pagesShunt Card Clin 2015cardiologiaimss34No ratings yet
- Approach To A Child With Congenital Heart DiseaseDocument31 pagesApproach To A Child With Congenital Heart DiseaseMUHAMMAD DANIAL BIN HASAN FPSKNo ratings yet
- 16 Syndr Cardiovas SystDocument11 pages16 Syndr Cardiovas Systjqpwzcg8xrNo ratings yet
- Rossano2014 PDFDocument6 pagesRossano2014 PDFAditya SanjayaNo ratings yet
- Aruna Ramesh-Emergency...Document6 pagesAruna Ramesh-Emergency...Aishu BNo ratings yet
- Duct Dependent Heart Lesions by DR Parashuram Waddar (Pediatrician, MBBS, DCH DNB)Document63 pagesDuct Dependent Heart Lesions by DR Parashuram Waddar (Pediatrician, MBBS, DCH DNB)parasuram waddarNo ratings yet
- Acyanotic and Cyanotic Congenital Heart DiseasesDocument7 pagesAcyanotic and Cyanotic Congenital Heart DiseasesAndrewNo ratings yet
- Congenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementDocument87 pagesCongenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementJZNo ratings yet
- FINAL Slides EKA Webinar 2021, STPDocument49 pagesFINAL Slides EKA Webinar 2021, STPKevin GilbertNo ratings yet
- Cardiac Disease in NeonatesDocument5 pagesCardiac Disease in NeonatesVera PetkovskaNo ratings yet
- Cardiovascular Diseases in PregnancyDocument27 pagesCardiovascular Diseases in PregnancyAlphine DalgoNo ratings yet
- K17. Conginetal Heart Disease (Dr. Yanti)Document107 pagesK17. Conginetal Heart Disease (Dr. Yanti)amaliyamataul100% (1)
- Background: EmbryologyDocument25 pagesBackground: EmbryologydonisaputraNo ratings yet
- Case Report CHF PedsDocument36 pagesCase Report CHF PedsKanagavalli VijayakumarNo ratings yet
- Congestive Heart Failure in Children: Education GapsDocument13 pagesCongestive Heart Failure in Children: Education GapsMida RidayantiNo ratings yet
- Atrioventricular Septal DefectDocument4 pagesAtrioventricular Septal DefectAti Rahmi PurwandariNo ratings yet
- MKR 049Document6 pagesMKR 049venkatesh chowdaryNo ratings yet
- Cardiac Evaluation of ThenewbornDocument19 pagesCardiac Evaluation of ThenewbornChristian MartínezNo ratings yet
- Nursing Care Plan For Acyanotic Heart DiseaseDocument55 pagesNursing Care Plan For Acyanotic Heart DiseaseDeepikaxena John79% (14)
- Tetralogy of FallotDocument31 pagesTetralogy of FallotAnditha Namira RS100% (1)
- Identifying Newborns With Critical Congenital Heart DiseaseDocument32 pagesIdentifying Newborns With Critical Congenital Heart DiseaseHardian RakhmawardanaNo ratings yet
- Heart Disease JaninDocument7 pagesHeart Disease JaninTiara Anggun NurartoNo ratings yet
- Congenital Heart Diseases.Document86 pagesCongenital Heart Diseases.Salman KhanNo ratings yet
- 11 History Growth Nutrition PE and Lab TestsDocument16 pages11 History Growth Nutrition PE and Lab TestsVictor PazNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- PericarditisDocument11 pagesPericarditisjosefamdNo ratings yet
- MedsciDocument12 pagesMedscikathNo ratings yet
- Mitral Stenosis For Non-Cardiac Surgery Case FileDocument4 pagesMitral Stenosis For Non-Cardiac Surgery Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Clasificacion Cardioaptias Ductus DependientesDocument7 pagesClasificacion Cardioaptias Ductus DependientesdavidNo ratings yet
- 10 Cardiology LectureDocument64 pages10 Cardiology Lectureaemy13266No ratings yet
- Cardio Vascular DiseasesDocument34 pagesCardio Vascular DiseasesSam ParkNo ratings yet
- Critical Congenital Heart Disease: Early Detection and ManagementDocument29 pagesCritical Congenital Heart Disease: Early Detection and ManagementtyesNo ratings yet
- Midterms Group 5Document25 pagesMidterms Group 5Karina MadriagaNo ratings yet
- Enfermedad Cardiovascular MaternaDocument12 pagesEnfermedad Cardiovascular MaternaWalter Huacani HuamaniNo ratings yet
- Congenital Acyanotic Heart DiseaseDocument46 pagesCongenital Acyanotic Heart DiseaseChaman AraNo ratings yet
- 1 s2.0 S2666668520300525 MainDocument7 pages1 s2.0 S2666668520300525 MainNura Eky VNo ratings yet
- Acynotic DiseaseDocument55 pagesAcynotic DiseaseTesfamichael AbathunNo ratings yet
- Molecular Mechanism of Peripartum Cardiomyopathy A Vaskular or Hormonal HypothesisDocument11 pagesMolecular Mechanism of Peripartum Cardiomyopathy A Vaskular or Hormonal HypothesisAnggi saputriNo ratings yet
- Management of Persistent Ductus ArteriosusDocument79 pagesManagement of Persistent Ductus Arteriosushashim adekunleNo ratings yet
- Congenital Heart DiseaseDocument20 pagesCongenital Heart DiseaseMogtaba M HilalNo ratings yet
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseMarisa PetersonNo ratings yet
- Cardiovascular DisordersDocument14 pagesCardiovascular DisordersRayan AhmedNo ratings yet
- Congenital Heart Disease - SeminarDocument35 pagesCongenital Heart Disease - SeminarAsha jilu100% (2)
- Narrative Review: Pulmonary Hypertension in CKDDocument11 pagesNarrative Review: Pulmonary Hypertension in CKDDr. Jatin GargNo ratings yet
- Low Cardiac Output ChildrenDocument11 pagesLow Cardiac Output ChildrenXavier AbrilNo ratings yet
- Congenital Heart Disease (CHD) : by Alireza PourtalebiDocument69 pagesCongenital Heart Disease (CHD) : by Alireza PourtalebiAswathy AswathyNo ratings yet
- The Pediatric Electrocardiogram Part III: Congenital Heart Disease and Other Cardiac SyndromesDocument7 pagesThe Pediatric Electrocardiogram Part III: Congenital Heart Disease and Other Cardiac SyndromesBijesh DasNo ratings yet
- Hypoplastic Left Heart Syndrome Diagnosis and ManagementDocument10 pagesHypoplastic Left Heart Syndrome Diagnosis and ManagementMore InterestingNo ratings yet
- Fetal Cardiac Intervention Rational, Risk and BenefitDocument4 pagesFetal Cardiac Intervention Rational, Risk and BenefitThomson AffendyNo ratings yet
- Heart Disease in PregnancyDocument14 pagesHeart Disease in PregnancyManisha ThakurNo ratings yet
- Cardiovascular DysfunctionDocument15 pagesCardiovascular DysfunctionJhasseryne Orias SanchezNo ratings yet
- Navigating Acute Heart Failure: Comprehensive Insights and Holistic ApproachesFrom EverandNavigating Acute Heart Failure: Comprehensive Insights and Holistic ApproachesNo ratings yet
- Cmas 508Document1 pageCmas 508Naman KhalidNo ratings yet
- Kikai Pencitraan 19 Oct 2022Document53 pagesKikai Pencitraan 19 Oct 2022Naman KhalidNo ratings yet
- Early Detection SLEDocument12 pagesEarly Detection SLENaman KhalidNo ratings yet
- HHS Public AccessDocument12 pagesHHS Public AccessNaman KhalidNo ratings yet
- J Coll Physicians Surg Pak 2018 28 3 206 209Document4 pagesJ Coll Physicians Surg Pak 2018 28 3 206 209Naman KhalidNo ratings yet
- Determinants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyDocument8 pagesDeterminants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyNaman KhalidNo ratings yet
- 2018 Article 1130Document9 pages2018 Article 1130Naman KhalidNo ratings yet
- Hubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaDocument7 pagesHubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaNaman KhalidNo ratings yet
- Turner Syndrome: New Insights From Prenatal Genomics and TranscriptomicsDocument5 pagesTurner Syndrome: New Insights From Prenatal Genomics and TranscriptomicsNaman KhalidNo ratings yet
- Cui 2018Document6 pagesCui 2018Naman KhalidNo ratings yet
- Critical AppraisalDocument47 pagesCritical AppraisalNaman KhalidNo ratings yet
- Bucerzan 2017Document10 pagesBucerzan 2017Naman KhalidNo ratings yet
- Daftar Singkatan Nama ObatDocument3 pagesDaftar Singkatan Nama ObatNaman KhalidNo ratings yet
- Jurnal RdsDocument6 pagesJurnal RdsNaman KhalidNo ratings yet
- Journal Article PowerpointDocument2 pagesJournal Article PowerpointNaman KhalidNo ratings yet
- IJP Volume 7 Issue 1 Pages 8815-8820-1Document6 pagesIJP Volume 7 Issue 1 Pages 8815-8820-1Naman KhalidNo ratings yet
- Research & Innovation: The EuDocument42 pagesResearch & Innovation: The EurubenpeNo ratings yet
- Anthropometrics ErgonomicsDocument78 pagesAnthropometrics ErgonomicsashokdinoNo ratings yet
- Layug V IACDocument1 pageLayug V IACYasser MambuayNo ratings yet
- Data Collection MethodsDocument18 pagesData Collection MethodsachsurajNo ratings yet
- Fraction - Improper Fraction To Mixed FractionDocument8 pagesFraction - Improper Fraction To Mixed FractionRisaNo ratings yet
- TAB Installation Instruction v1.1Document15 pagesTAB Installation Instruction v1.1vignesh. viswanathanNo ratings yet
- Niir Mumbai Companies Directory Database XLSX Excel Format 5th EditionDocument2 pagesNiir Mumbai Companies Directory Database XLSX Excel Format 5th Editionphone25hire phone25hireNo ratings yet
- George The SlugDocument4 pagesGeorge The SlugAndrewBayangNo ratings yet
- Wed Sept 6 GeographyDocument17 pagesWed Sept 6 Geographyapi-367886489No ratings yet
- C161 Occupational Health Services ConventionDocument7 pagesC161 Occupational Health Services ConventionKeith RhodesNo ratings yet
- Frac Pack Offshore Sand ControlDocument15 pagesFrac Pack Offshore Sand ControlRamanamurthy PalliNo ratings yet
- ENGLISH - 2006 Read The Following Poem Carefully and Answer The Questions That Follow: (8 Marks) Forest FiresDocument6 pagesENGLISH - 2006 Read The Following Poem Carefully and Answer The Questions That Follow: (8 Marks) Forest FiresSanjay KumarNo ratings yet
- Complete Guide For Growing Plants Hydroponically by J Benton Jones JR B00hznqitmDocument5 pagesComplete Guide For Growing Plants Hydroponically by J Benton Jones JR B00hznqitmnagesh dolasNo ratings yet
- Case CX TrainingDocument20 pagesCase CX Traininghoward100% (27)
- Math 8 Q3 Module 5 With Answer KeyDocument13 pagesMath 8 Q3 Module 5 With Answer KeyJimcris villamorNo ratings yet
- Emflon PFRW Filter Cartridges: For Sterile Filtration of GasesDocument3 pagesEmflon PFRW Filter Cartridges: For Sterile Filtration of GasesRichard BakerNo ratings yet
- Nami Solar Company Profile Aug 2020 ENGDocument13 pagesNami Solar Company Profile Aug 2020 ENGKien Trung Nguyen100% (1)
- Hdat2en 4 52Document156 pagesHdat2en 4 52blahh12345689No ratings yet
- 08 - Chapter 3 PDFDocument36 pages08 - Chapter 3 PDF1921 Vishwanath PakhareNo ratings yet
- Anderson Distribution of The Correlation CoefficientDocument14 pagesAnderson Distribution of The Correlation Coefficientdauren_pcNo ratings yet
- Mac25 Maintenance Section 2Document27 pagesMac25 Maintenance Section 2Wahyu SriharjaNo ratings yet
- Technical Paper (Al Sharq Tower)Document17 pagesTechnical Paper (Al Sharq Tower)ကိုနေဝင်းNo ratings yet
- Coordinte GeometryDocument72 pagesCoordinte GeometrySukhamrit PalNo ratings yet
- Fundamentals of Thermal Sensors: Thu HuynhDocument39 pagesFundamentals of Thermal Sensors: Thu HuynhsamcaridoNo ratings yet
- Lacerte Jennifer ResumeDocument1 pageLacerte Jennifer Resumejennifer_lacerteNo ratings yet
- 1575517183688JlPSe5QaAila2orp PDFDocument15 pages1575517183688JlPSe5QaAila2orp PDFPr Satish BethaNo ratings yet
- Final Report: Simulation Using Star CCM+ Theory and Practice in Marine CFD BenaoeDocument10 pagesFinal Report: Simulation Using Star CCM+ Theory and Practice in Marine CFD BenaoeRaviindra singhNo ratings yet








































































































Download as pdf or txt
You might also like
- Broomfield Hospital Site Plan: Café Shops Lifts Information PointsDocument1 pageBroomfield Hospital Site Plan: Café Shops Lifts Information Pointsady trader0% (2)
- Project Proposal On Dairy FarmDocument26 pagesProject Proposal On Dairy Farmvector dairy88% (8)
- 557-Assign 2-Action Plan For Culturally-Diverse School ClimateDocument10 pages557-Assign 2-Action Plan For Culturally-Diverse School Climateapi-566276833No ratings yet
- Cardiovascular DisorderDocument88 pagesCardiovascular DisorderSandeepNo ratings yet
- Pedia Cardiology 2Document5 pagesPedia Cardiology 2Medisina101No ratings yet
- Congenital Heart Disease: Education and Practice GapsDocument18 pagesCongenital Heart Disease: Education and Practice GapsAlvaro Ignacio Lagos SuilNo ratings yet
- Anesthesia For Noncardiac Surgery in Adults With Congenital Heart DiseaseDocument9 pagesAnesthesia For Noncardiac Surgery in Adults With Congenital Heart DiseaseIda Bagus MahendraNo ratings yet
- Congenital Heart Disease (2011)Document17 pagesCongenital Heart Disease (2011)drheay100% (1)
- Neonatal Cardiac EmergenciesDocument4 pagesNeonatal Cardiac EmergenciesEstellaNo ratings yet
- Tamizaje Enfermedades CardiacasDocument16 pagesTamizaje Enfermedades CardiacasDanna GonzálezNo ratings yet
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- Shunt Card Clin 2015Document8 pagesShunt Card Clin 2015cardiologiaimss34No ratings yet
- Approach To A Child With Congenital Heart DiseaseDocument31 pagesApproach To A Child With Congenital Heart DiseaseMUHAMMAD DANIAL BIN HASAN FPSKNo ratings yet
- 16 Syndr Cardiovas SystDocument11 pages16 Syndr Cardiovas Systjqpwzcg8xrNo ratings yet
- Rossano2014 PDFDocument6 pagesRossano2014 PDFAditya SanjayaNo ratings yet
- Aruna Ramesh-Emergency...Document6 pagesAruna Ramesh-Emergency...Aishu BNo ratings yet
- Duct Dependent Heart Lesions by DR Parashuram Waddar (Pediatrician, MBBS, DCH DNB)Document63 pagesDuct Dependent Heart Lesions by DR Parashuram Waddar (Pediatrician, MBBS, DCH DNB)parasuram waddarNo ratings yet
- Acyanotic and Cyanotic Congenital Heart DiseasesDocument7 pagesAcyanotic and Cyanotic Congenital Heart DiseasesAndrewNo ratings yet
- Congenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementDocument87 pagesCongenital Cardiac Disease: A Guide To Evaluation, Treatment and Anesthetic ManagementJZNo ratings yet
- FINAL Slides EKA Webinar 2021, STPDocument49 pagesFINAL Slides EKA Webinar 2021, STPKevin GilbertNo ratings yet
- Cardiac Disease in NeonatesDocument5 pagesCardiac Disease in NeonatesVera PetkovskaNo ratings yet
- Cardiovascular Diseases in PregnancyDocument27 pagesCardiovascular Diseases in PregnancyAlphine DalgoNo ratings yet
- K17. Conginetal Heart Disease (Dr. Yanti)Document107 pagesK17. Conginetal Heart Disease (Dr. Yanti)amaliyamataul100% (1)
- Background: EmbryologyDocument25 pagesBackground: EmbryologydonisaputraNo ratings yet
- Case Report CHF PedsDocument36 pagesCase Report CHF PedsKanagavalli VijayakumarNo ratings yet
- Congestive Heart Failure in Children: Education GapsDocument13 pagesCongestive Heart Failure in Children: Education GapsMida RidayantiNo ratings yet
- Atrioventricular Septal DefectDocument4 pagesAtrioventricular Septal DefectAti Rahmi PurwandariNo ratings yet
- MKR 049Document6 pagesMKR 049venkatesh chowdaryNo ratings yet
- Cardiac Evaluation of ThenewbornDocument19 pagesCardiac Evaluation of ThenewbornChristian MartínezNo ratings yet
- Nursing Care Plan For Acyanotic Heart DiseaseDocument55 pagesNursing Care Plan For Acyanotic Heart DiseaseDeepikaxena John79% (14)
- Tetralogy of FallotDocument31 pagesTetralogy of FallotAnditha Namira RS100% (1)
- Identifying Newborns With Critical Congenital Heart DiseaseDocument32 pagesIdentifying Newborns With Critical Congenital Heart DiseaseHardian RakhmawardanaNo ratings yet
- Heart Disease JaninDocument7 pagesHeart Disease JaninTiara Anggun NurartoNo ratings yet
- Congenital Heart Diseases.Document86 pagesCongenital Heart Diseases.Salman KhanNo ratings yet
- 11 History Growth Nutrition PE and Lab TestsDocument16 pages11 History Growth Nutrition PE and Lab TestsVictor PazNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- PericarditisDocument11 pagesPericarditisjosefamdNo ratings yet
- MedsciDocument12 pagesMedscikathNo ratings yet
- Mitral Stenosis For Non-Cardiac Surgery Case FileDocument4 pagesMitral Stenosis For Non-Cardiac Surgery Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Clasificacion Cardioaptias Ductus DependientesDocument7 pagesClasificacion Cardioaptias Ductus DependientesdavidNo ratings yet
- 10 Cardiology LectureDocument64 pages10 Cardiology Lectureaemy13266No ratings yet
- Cardio Vascular DiseasesDocument34 pagesCardio Vascular DiseasesSam ParkNo ratings yet
- Critical Congenital Heart Disease: Early Detection and ManagementDocument29 pagesCritical Congenital Heart Disease: Early Detection and ManagementtyesNo ratings yet
- Midterms Group 5Document25 pagesMidterms Group 5Karina MadriagaNo ratings yet
- Enfermedad Cardiovascular MaternaDocument12 pagesEnfermedad Cardiovascular MaternaWalter Huacani HuamaniNo ratings yet
- Congenital Acyanotic Heart DiseaseDocument46 pagesCongenital Acyanotic Heart DiseaseChaman AraNo ratings yet
- 1 s2.0 S2666668520300525 MainDocument7 pages1 s2.0 S2666668520300525 MainNura Eky VNo ratings yet
- Acynotic DiseaseDocument55 pagesAcynotic DiseaseTesfamichael AbathunNo ratings yet
- Molecular Mechanism of Peripartum Cardiomyopathy A Vaskular or Hormonal HypothesisDocument11 pagesMolecular Mechanism of Peripartum Cardiomyopathy A Vaskular or Hormonal HypothesisAnggi saputriNo ratings yet
- Management of Persistent Ductus ArteriosusDocument79 pagesManagement of Persistent Ductus Arteriosushashim adekunleNo ratings yet
- Congenital Heart DiseaseDocument20 pagesCongenital Heart DiseaseMogtaba M HilalNo ratings yet
- Congenital Heart DiseaseDocument10 pagesCongenital Heart DiseaseMarisa PetersonNo ratings yet
- Cardiovascular DisordersDocument14 pagesCardiovascular DisordersRayan AhmedNo ratings yet
- Congenital Heart Disease - SeminarDocument35 pagesCongenital Heart Disease - SeminarAsha jilu100% (2)
- Narrative Review: Pulmonary Hypertension in CKDDocument11 pagesNarrative Review: Pulmonary Hypertension in CKDDr. Jatin GargNo ratings yet
- Low Cardiac Output ChildrenDocument11 pagesLow Cardiac Output ChildrenXavier AbrilNo ratings yet
- Congenital Heart Disease (CHD) : by Alireza PourtalebiDocument69 pagesCongenital Heart Disease (CHD) : by Alireza PourtalebiAswathy AswathyNo ratings yet
- The Pediatric Electrocardiogram Part III: Congenital Heart Disease and Other Cardiac SyndromesDocument7 pagesThe Pediatric Electrocardiogram Part III: Congenital Heart Disease and Other Cardiac SyndromesBijesh DasNo ratings yet
- Hypoplastic Left Heart Syndrome Diagnosis and ManagementDocument10 pagesHypoplastic Left Heart Syndrome Diagnosis and ManagementMore InterestingNo ratings yet
- Fetal Cardiac Intervention Rational, Risk and BenefitDocument4 pagesFetal Cardiac Intervention Rational, Risk and BenefitThomson AffendyNo ratings yet
- Heart Disease in PregnancyDocument14 pagesHeart Disease in PregnancyManisha ThakurNo ratings yet
- Cardiovascular DysfunctionDocument15 pagesCardiovascular DysfunctionJhasseryne Orias SanchezNo ratings yet
- Navigating Acute Heart Failure: Comprehensive Insights and Holistic ApproachesFrom EverandNavigating Acute Heart Failure: Comprehensive Insights and Holistic ApproachesNo ratings yet
- Cmas 508Document1 pageCmas 508Naman KhalidNo ratings yet
- Kikai Pencitraan 19 Oct 2022Document53 pagesKikai Pencitraan 19 Oct 2022Naman KhalidNo ratings yet
- Early Detection SLEDocument12 pagesEarly Detection SLENaman KhalidNo ratings yet
- HHS Public AccessDocument12 pagesHHS Public AccessNaman KhalidNo ratings yet
- J Coll Physicians Surg Pak 2018 28 3 206 209Document4 pagesJ Coll Physicians Surg Pak 2018 28 3 206 209Naman KhalidNo ratings yet
- Determinants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyDocument8 pagesDeterminants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyNaman KhalidNo ratings yet
- 2018 Article 1130Document9 pages2018 Article 1130Naman KhalidNo ratings yet
- Hubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaDocument7 pagesHubungan Asfiksia Neonatorum Dan BBLR Dengan Kejadian Sepsis Neonatorum Di Rsud Abdul Wahab Sjahranie SamarindaNaman KhalidNo ratings yet
- Turner Syndrome: New Insights From Prenatal Genomics and TranscriptomicsDocument5 pagesTurner Syndrome: New Insights From Prenatal Genomics and TranscriptomicsNaman KhalidNo ratings yet
- Cui 2018Document6 pagesCui 2018Naman KhalidNo ratings yet
- Critical AppraisalDocument47 pagesCritical AppraisalNaman KhalidNo ratings yet
- Bucerzan 2017Document10 pagesBucerzan 2017Naman KhalidNo ratings yet
- Daftar Singkatan Nama ObatDocument3 pagesDaftar Singkatan Nama ObatNaman KhalidNo ratings yet
- Jurnal RdsDocument6 pagesJurnal RdsNaman KhalidNo ratings yet
- Journal Article PowerpointDocument2 pagesJournal Article PowerpointNaman KhalidNo ratings yet
- IJP Volume 7 Issue 1 Pages 8815-8820-1Document6 pagesIJP Volume 7 Issue 1 Pages 8815-8820-1Naman KhalidNo ratings yet
- Research & Innovation: The EuDocument42 pagesResearch & Innovation: The EurubenpeNo ratings yet
- Anthropometrics ErgonomicsDocument78 pagesAnthropometrics ErgonomicsashokdinoNo ratings yet
- Layug V IACDocument1 pageLayug V IACYasser MambuayNo ratings yet
- Data Collection MethodsDocument18 pagesData Collection MethodsachsurajNo ratings yet
- Fraction - Improper Fraction To Mixed FractionDocument8 pagesFraction - Improper Fraction To Mixed FractionRisaNo ratings yet
- TAB Installation Instruction v1.1Document15 pagesTAB Installation Instruction v1.1vignesh. viswanathanNo ratings yet
- Niir Mumbai Companies Directory Database XLSX Excel Format 5th EditionDocument2 pagesNiir Mumbai Companies Directory Database XLSX Excel Format 5th Editionphone25hire phone25hireNo ratings yet
- George The SlugDocument4 pagesGeorge The SlugAndrewBayangNo ratings yet
- Wed Sept 6 GeographyDocument17 pagesWed Sept 6 Geographyapi-367886489No ratings yet
- C161 Occupational Health Services ConventionDocument7 pagesC161 Occupational Health Services ConventionKeith RhodesNo ratings yet
- Frac Pack Offshore Sand ControlDocument15 pagesFrac Pack Offshore Sand ControlRamanamurthy PalliNo ratings yet
- ENGLISH - 2006 Read The Following Poem Carefully and Answer The Questions That Follow: (8 Marks) Forest FiresDocument6 pagesENGLISH - 2006 Read The Following Poem Carefully and Answer The Questions That Follow: (8 Marks) Forest FiresSanjay KumarNo ratings yet
- Complete Guide For Growing Plants Hydroponically by J Benton Jones JR B00hznqitmDocument5 pagesComplete Guide For Growing Plants Hydroponically by J Benton Jones JR B00hznqitmnagesh dolasNo ratings yet
- Case CX TrainingDocument20 pagesCase CX Traininghoward100% (27)
- Math 8 Q3 Module 5 With Answer KeyDocument13 pagesMath 8 Q3 Module 5 With Answer KeyJimcris villamorNo ratings yet
- Emflon PFRW Filter Cartridges: For Sterile Filtration of GasesDocument3 pagesEmflon PFRW Filter Cartridges: For Sterile Filtration of GasesRichard BakerNo ratings yet
- Nami Solar Company Profile Aug 2020 ENGDocument13 pagesNami Solar Company Profile Aug 2020 ENGKien Trung Nguyen100% (1)
- Hdat2en 4 52Document156 pagesHdat2en 4 52blahh12345689No ratings yet
- 08 - Chapter 3 PDFDocument36 pages08 - Chapter 3 PDF1921 Vishwanath PakhareNo ratings yet
- Anderson Distribution of The Correlation CoefficientDocument14 pagesAnderson Distribution of The Correlation Coefficientdauren_pcNo ratings yet
- Mac25 Maintenance Section 2Document27 pagesMac25 Maintenance Section 2Wahyu SriharjaNo ratings yet
- Technical Paper (Al Sharq Tower)Document17 pagesTechnical Paper (Al Sharq Tower)ကိုနေဝင်းNo ratings yet
- Coordinte GeometryDocument72 pagesCoordinte GeometrySukhamrit PalNo ratings yet
- Fundamentals of Thermal Sensors: Thu HuynhDocument39 pagesFundamentals of Thermal Sensors: Thu HuynhsamcaridoNo ratings yet
- Lacerte Jennifer ResumeDocument1 pageLacerte Jennifer Resumejennifer_lacerteNo ratings yet
- 1575517183688JlPSe5QaAila2orp PDFDocument15 pages1575517183688JlPSe5QaAila2orp PDFPr Satish BethaNo ratings yet
- Final Report: Simulation Using Star CCM+ Theory and Practice in Marine CFD BenaoeDocument10 pagesFinal Report: Simulation Using Star CCM+ Theory and Practice in Marine CFD BenaoeRaviindra singhNo ratings yet