Download as pdf or txt
You might also like
- Nurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsDocument10 pagesNurse-Directed Interventions To Reduce Catheter-Associated Urinary Tract InfectionsAngernani Trias WulandariNo ratings yet
- Adorno - A Guide For The Perplexed - Alex ThomsonDocument183 pagesAdorno - A Guide For The Perplexed - Alex ThomsonAline100% (1)
- CAUTI Barriers For Nurse DrivenDocument19 pagesCAUTI Barriers For Nurse Drivenayngn13No ratings yet
- Jurnal Uro 2Document8 pagesJurnal Uro 2Lisa HikmawanNo ratings yet
- 440 Leadership Strategic AnalysisDocument7 pages440 Leadership Strategic Analysisapi-212894173No ratings yet
- Journal Pdig 0000017Document38 pagesJournal Pdig 0000017Emmanuel SandovalNo ratings yet
- The Ann Arbor Criteria For Appropriate Urinary Catheter Use in Hospitalized Medical Patients: Results Obtained by Using The RAND/UCLA Appropriateness MethodDocument34 pagesThe Ann Arbor Criteria For Appropriate Urinary Catheter Use in Hospitalized Medical Patients: Results Obtained by Using The RAND/UCLA Appropriateness MethodCarissa SulaimanNo ratings yet
- External Quality Assessment in Resource-Limited CoDocument14 pagesExternal Quality Assessment in Resource-Limited CoEben Leonel Albano MaiopueNo ratings yet
- Utilization Management in A Large Urban Academic Medical CenterDocument11 pagesUtilization Management in A Large Urban Academic Medical CenterMELYANo ratings yet
- Preventing Ventilator-Associated ICHEDocument8 pagesPreventing Ventilator-Associated ICHEFelix Brian FelixNo ratings yet
- Ebp FormativeDocument12 pagesEbp Formativeapi-288858560No ratings yet
- Adherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaDocument9 pagesAdherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaIJAR JOURNALNo ratings yet
- Adherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaDocument9 pagesAdherence of Physicians Practice Tonational Ministry of Health (Moh) Urgent Care Guideline in Eastern Region, Saudi ArabiaIJAR JOURNALNo ratings yet
- Artigo 2 CinhalDocument7 pagesArtigo 2 CinhalSara PereiraNo ratings yet
- Impact of CommercialDocument10 pagesImpact of Commercialmaya permata sariNo ratings yet
- Patients Preferences Regarding The Process and Outcomes of Lifesaving TechnologyDocument12 pagesPatients Preferences Regarding The Process and Outcomes of Lifesaving TechnologyGenevieve DavidNo ratings yet
- Jurnal Manajemen Patient SafetyDocument7 pagesJurnal Manajemen Patient SafetyfarizkaNo ratings yet
- Effect of Splint Application On The Functional Duration of Peripheral Intravenous Cannulation in Neonates: A Systematic Review and Meta-AnalysisDocument14 pagesEffect of Splint Application On The Functional Duration of Peripheral Intravenous Cannulation in Neonates: A Systematic Review and Meta-AnalysisABIR SANTRANo ratings yet
- The Michigan Appropriateness Guide For Intravenous Catheters (MAGIC) : Results From A Multispecialty Panel Using The RAND/UCLA Appropriateness MethodDocument48 pagesThe Michigan Appropriateness Guide For Intravenous Catheters (MAGIC) : Results From A Multispecialty Panel Using The RAND/UCLA Appropriateness Methodnanang criztaNo ratings yet
- Macam-Macam GuidelineDocument17 pagesMacam-Macam GuidelineFrederickSuryaNo ratings yet
- Nurses ' Perceptions of A Pressure Ulcer Prevention Care Bundle: A Qualitative Descriptive StudyDocument10 pagesNurses ' Perceptions of A Pressure Ulcer Prevention Care Bundle: A Qualitative Descriptive StudyBrekhna SaharNo ratings yet
- CDSSDocument16 pagesCDSSMartinus CiputraNo ratings yet
- Amiks-Ebn ProjectDocument9 pagesAmiks-Ebn Projectapi-530909386No ratings yet
- Fast Track Registration A Way To Increase Efficiency in The Ir DivisionDocument7 pagesFast Track Registration A Way To Increase Efficiency in The Ir DivisionAli MoosaviNo ratings yet
- Implementation and Use of Point of Care C R 2022 Journal of The American MedDocument11 pagesImplementation and Use of Point of Care C R 2022 Journal of The American MedPuttryNo ratings yet
- Colorectal BundlesDocument16 pagesColorectal BundlesDamie ChaulaNo ratings yet
- Siemieniuk Et Al Systematic ReviewDocument26 pagesSiemieniuk Et Al Systematic Reviewhadom73076No ratings yet
- A Bedside Swallowing Screen For The IdentificationDocument10 pagesA Bedside Swallowing Screen For The IdentificationGabriela BarriosNo ratings yet
- Implementation of A Spontantaneous Breathing Trial Protocol Friendly)Document16 pagesImplementation of A Spontantaneous Breathing Trial Protocol Friendly)Reema KhalafNo ratings yet
- Improving The WHO Surgical Safety Checklist Sign-ODocument7 pagesImproving The WHO Surgical Safety Checklist Sign-Obeny.rahman.khomaini-2022No ratings yet
- Journal SatuDocument6 pagesJournal SatuIntan DwiNo ratings yet
- A Nurse-Driven Protocol ForDocument8 pagesA Nurse-Driven Protocol ForWardah Fauziah El SofwanNo ratings yet
- Sedación ProtocolizadaDocument11 pagesSedación ProtocolizadaAlejandra LópezNo ratings yet
- The Accuracy of Implant Placement With Computer-GuidedDocument11 pagesThe Accuracy of Implant Placement With Computer-GuidedRyan Ardi PradanaNo ratings yet
- Use of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwideDocument7 pagesUse of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwidemochkurniawanNo ratings yet
- 1 s2.0 S000296101000454X MainDocument4 pages1 s2.0 S000296101000454X MainimNo ratings yet
- Ebp PaperDocument14 pagesEbp Paperapi-324392818No ratings yet
- J Clinic Periodontology - 2023 - StieschDocument22 pagesJ Clinic Periodontology - 2023 - StieschtzulinNo ratings yet
- A Framework For Evaluating The Appropriateness of Clinical Decision Support Alerts and ResponsesDocument8 pagesA Framework For Evaluating The Appropriateness of Clinical Decision Support Alerts and ResponsesSocorro Moreno LunaNo ratings yet
- Riad074 048Document2 pagesRiad074 048Melinda Surya UtariNo ratings yet
- The Impact of Thoracic Ultrasound On Clinical Management of CriticallyDocument8 pagesThe Impact of Thoracic Ultrasound On Clinical Management of CriticallyBruce Fredy Chino ChambillaNo ratings yet
- 2023 RS y MA 4 DíasDocument11 pages2023 RS y MA 4 DíasFrancisco OrmeñoNo ratings yet
- Ebp PresentationDocument30 pagesEbp Presentationapi-708254576No ratings yet
- 2016 S 0042 100186 PDFDocument4 pages2016 S 0042 100186 PDFMadalina StoicescuNo ratings yet
- A Multivariate Time Series Approach To Modeling and Forecasting Demand in The Emergency DepartmentDocument17 pagesA Multivariate Time Series Approach To Modeling and Forecasting Demand in The Emergency DepartmentmaleticjNo ratings yet
- How Long Does Treatment With Fixed Orthodontic Appliances Last? A Systematic ReviewDocument11 pagesHow Long Does Treatment With Fixed Orthodontic Appliances Last? A Systematic ReviewSrishti SyalNo ratings yet
- A Systematic Review of Perioperative Clinical PracDocument10 pagesA Systematic Review of Perioperative Clinical PracBhavani VuppuNo ratings yet
- Zurmehly 2018Document6 pagesZurmehly 2018DavennBacudNo ratings yet
- Journal Pre-Proof: International Journal of Medical InformaticsDocument29 pagesJournal Pre-Proof: International Journal of Medical InformaticsDityan KaleNo ratings yet
- Fmed 08 584813Document12 pagesFmed 08 584813Annisa SetyantiNo ratings yet
- Oncology Nursing Trends and Issues 3Document7 pagesOncology Nursing Trends and Issues 3DaichiNo ratings yet
- EVIDoa 2100016Document12 pagesEVIDoa 2100016anthonybear53No ratings yet
- THSS 10 1663974Document15 pagesTHSS 10 1663974Jamaah Ki HendroNo ratings yet
- Effect of Standardized Electronic Discharge Instructions On Post-Discharge Hospital UtilizationDocument7 pagesEffect of Standardized Electronic Discharge Instructions On Post-Discharge Hospital UtilizationAnonymous FqiDPxDW2No ratings yet
- J Nursing Management - 2021 - Saville - Ward Staffing Guided by A Patient Classification System A Multi Criteria AnalysisDocument10 pagesJ Nursing Management - 2021 - Saville - Ward Staffing Guided by A Patient Classification System A Multi Criteria AnalysisenfaraujoNo ratings yet
- J Nursing Management - 2021 - Hunt O Connor - The Effect of Discharge Planning On Length of Stay and Readmission Rates ofDocument10 pagesJ Nursing Management - 2021 - Hunt O Connor - The Effect of Discharge Planning On Length of Stay and Readmission Rates ofJumasing MasingNo ratings yet
- Callen2006 - OkDocument10 pagesCallen2006 - OkFernanda Gusmão LouredoNo ratings yet
- 10.1515 - CCLM 2018 0059Document8 pages10.1515 - CCLM 2018 0059Chris PaulNo ratings yet
- 1.4 Means (Opcional)Document13 pages1.4 Means (Opcional)Epi SidaNo ratings yet
- 1 s2.0 S1072751521021414 MainDocument24 pages1 s2.0 S1072751521021414 MainhendraNo ratings yet
- Rapid On-site Evaluation (ROSE): A Practical GuideFrom EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiNo ratings yet
- Bullying: A Cancer That Must Be EradicatedDocument2 pagesBullying: A Cancer That Must Be EradicatedMelaRiantiNo ratings yet
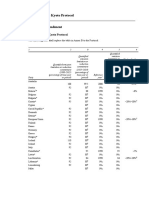
- Doha Amendment PDFDocument6 pagesDoha Amendment PDFPatricia BenildaNo ratings yet
- Veritas Check ID DocumentsDocument2 pagesVeritas Check ID DocumentsMax RamirezNo ratings yet
- MRR3 A51Document2 pagesMRR3 A51Gette-YzekNo ratings yet
- International Relations VocabularyDocument1 pageInternational Relations Vocabularyjeanneidys GNo ratings yet
- Qarardad e Lahore - Google SearchDocument1 pageQarardad e Lahore - Google Searchjc9wwmzbtsNo ratings yet
- Article Viii - Judicial Department Section 1-8Document21 pagesArticle Viii - Judicial Department Section 1-8Arnel M. MapaNo ratings yet
- Info Regulatory Burden Federal AgenciesDocument1 pageInfo Regulatory Burden Federal AgenciesAyesha khanNo ratings yet
- Piszel v. United StatesDocument23 pagesPiszel v. United StatesCato InstituteNo ratings yet
- Strunk and Phelps - Amicus Curiae Brief and Appendix USCA 9th Circuit 15-15343Document169 pagesStrunk and Phelps - Amicus Curiae Brief and Appendix USCA 9th Circuit 15-15343Christopher Earl Strunk100% (1)
- Alliance of Government Workers V MOLEDocument8 pagesAlliance of Government Workers V MOLEM Azeneth JJNo ratings yet
- Cindy Hyde SmithDocument128 pagesCindy Hyde SmithRuss LatinoNo ratings yet
- Naga National High School: West Poblacion, City of Naga, Cebu Telefax: 272-7912Document5 pagesNaga National High School: West Poblacion, City of Naga, Cebu Telefax: 272-7912Earl FrancisNo ratings yet
- Annotated BibliographyDocument11 pagesAnnotated Bibliographyknowlesall100% (1)
- Balkan Languages - Victor FriedmanDocument12 pagesBalkan Languages - Victor FriedmanBasiol Chulev100% (2)
- Design, Cost Estimation and Development of Guidelines For The Construction of Rain Water Harvesting Pond.Document80 pagesDesign, Cost Estimation and Development of Guidelines For The Construction of Rain Water Harvesting Pond.Umer Malik100% (1)
- Notice: Adjustment Assistance Applications, Determinations, Etc.: Eastman Kodak Co.Document1 pageNotice: Adjustment Assistance Applications, Determinations, Etc.: Eastman Kodak Co.Justia.comNo ratings yet
- The Mirror of Shakespeare (Hamlet Commentary)Document9 pagesThe Mirror of Shakespeare (Hamlet Commentary)Kaylee HallNo ratings yet
- Department of Health: "Quality Is Above Quantity" - Philosophy of DOHDocument2 pagesDepartment of Health: "Quality Is Above Quantity" - Philosophy of DOHPatricia RamosNo ratings yet
- Module 13 RevisedDocument6 pagesModule 13 Revisedapi-269269020No ratings yet
- The Hindu HD Delhi Edition 21-05-2024Document18 pagesThe Hindu HD Delhi Edition 21-05-2024work.shellysNo ratings yet
- Globalization in World System TheoryDocument3 pagesGlobalization in World System TheoryrumahbianglalaNo ratings yet
- Geopolitics AND SUPERPOWER ASSIGNMENTDocument11 pagesGeopolitics AND SUPERPOWER ASSIGNMENTAditi SinghNo ratings yet
- North Tonawanda NY Evening News 1939 Jul-Dec - Grayscale - 0348Document1 pageNorth Tonawanda NY Evening News 1939 Jul-Dec - Grayscale - 0348Kristina HyltonNo ratings yet
- William Cameron ForbesDocument3 pagesWilliam Cameron ForbesAndré BragaNo ratings yet
- Civil WarDocument7 pagesCivil WarChibi-KittyNo ratings yet
- Constitution of ApatzingánDocument2 pagesConstitution of ApatzingánThiago PiresNo ratings yet
- Tripartism and Social Dialogue-2Document32 pagesTripartism and Social Dialogue-2DOLE Region 6No ratings yet
- The Chronic Crisis of American Democracy The Way Is Shut Benjamin Studebaker Full ChapterDocument67 pagesThe Chronic Crisis of American Democracy The Way Is Shut Benjamin Studebaker Full Chapterivy.crawford638100% (11)