Download as pdf or txt
You might also like
- CCDM Manual PDFDocument715 pagesCCDM Manual PDFrehanaNo ratings yet
- Electricity BillDocument2 pagesElectricity BillRajesh0% (1)
- (Solution Manual) Fundamentals of Electric Circuits 4ed - Sadiku-Pages-774-800Document35 pages(Solution Manual) Fundamentals of Electric Circuits 4ed - Sadiku-Pages-774-800Leo Aude100% (1)
- 2 PBDocument6 pages2 PBaleon85No ratings yet
- BPJ Vol 14 No 2 P 921-938Document18 pagesBPJ Vol 14 No 2 P 921-938Satish SinghNo ratings yet
- Final-Galley Proof 2Document3 pagesFinal-Galley Proof 2rvfz9jw649No ratings yet
- Study On Ovarian Tumors in Pediatric and Adolescent Girls in A Tertiary Care CentreDocument7 pagesStudy On Ovarian Tumors in Pediatric and Adolescent Girls in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Age and Duration of Hormonal Therapy Affect The Recurrence of Ovarian Endometrioma After Conservative Surgery A Retrospective Analytical Observational StudyDocument7 pagesAge and Duration of Hormonal Therapy Affect The Recurrence of Ovarian Endometrioma After Conservative Surgery A Retrospective Analytical Observational Studytotok hendartoNo ratings yet
- Undescended Testis: Ravibindu RanawakaDocument2 pagesUndescended Testis: Ravibindu RanawakaBrianne LeeNo ratings yet
- Chen 2015Document6 pagesChen 2015ben_mantiriNo ratings yet
- A Study On Surgical Management of Undescended TestDocument6 pagesA Study On Surgical Management of Undescended TestAhmed teroNo ratings yet
- Medicine: Intrauterine Device Found in An Ovarian TumorDocument5 pagesMedicine: Intrauterine Device Found in An Ovarian TumorRezky amalia basirNo ratings yet
- Early Presentation of Gestational Trophoblastic Neoplasia After Term DeliveryDocument4 pagesEarly Presentation of Gestational Trophoblastic Neoplasia After Term DeliveryIJAR JOURNALNo ratings yet
- Treatment For Benign Thyroid Nodules With A CombinDocument7 pagesTreatment For Benign Thyroid Nodules With A CombindarthjesussithNo ratings yet
- The Cell Phone in The Twenty-First Century - Risk For Addiction or Ingestion - Case Report and Review of The LiteratureDocument2 pagesThe Cell Phone in The Twenty-First Century - Risk For Addiction or Ingestion - Case Report and Review of The LiteraturejernsssNo ratings yet
- Bartels 2014Document6 pagesBartels 2014docadax848No ratings yet
- Delforno 2021Document7 pagesDelforno 2021Putri Tamara DasantosNo ratings yet
- Predictive Factors For Recovery in Idiopathic Sudden Sensory Neural Hearing LossDocument8 pagesPredictive Factors For Recovery in Idiopathic Sudden Sensory Neural Hearing LossMiss AmyNo ratings yet
- Nutrients 14 04940 v3Document15 pagesNutrients 14 04940 v3Tamires SantanaNo ratings yet
- Fetal Anomalies Resulting in Termination of Pregnancy in Consanguineous Marriage - An Experience in Tertiary CareDocument8 pagesFetal Anomalies Resulting in Termination of Pregnancy in Consanguineous Marriage - An Experience in Tertiary CareIJAR JOURNALNo ratings yet
- Clinical Evidence of Positive Correlation Between Intrauterine Adhesions and Chronic Endometritis: A Retrospective StudyDocument7 pagesClinical Evidence of Positive Correlation Between Intrauterine Adhesions and Chronic Endometritis: A Retrospective Studyvita udiNo ratings yet
- Management of Abnormal Uterine Bleeding in Perimenarche: Diagnostic ChallengesDocument4 pagesManagement of Abnormal Uterine Bleeding in Perimenarche: Diagnostic ChallengesIda_Maryani94No ratings yet
- Primary Amenorrhea - A One Year Review: Obstetrics & Gynecology International JournalDocument4 pagesPrimary Amenorrhea - A One Year Review: Obstetrics & Gynecology International JournalGeta Okta PrayogiNo ratings yet
- Endometrial Tuberculosis Revealed by Post-Menopausal Metrorrhagia Report CaseDocument4 pagesEndometrial Tuberculosis Revealed by Post-Menopausal Metrorrhagia Report CaseIJAR JOURNALNo ratings yet
- JCM 10 04399Document11 pagesJCM 10 04399sherintheresa95No ratings yet
- Endometrial Adenocarcinoma A Tahbso CaseDocument78 pagesEndometrial Adenocarcinoma A Tahbso CaseJohn Mark Obrero100% (1)
- Response To Methylprednisolone Bolus in Children Treated For Nephrotic Syndrome at The Pediatric Nephrology Unit in AbidjanDocument5 pagesResponse To Methylprednisolone Bolus in Children Treated For Nephrotic Syndrome at The Pediatric Nephrology Unit in AbidjanIJAR JOURNALNo ratings yet
- Mikropenis NcbiDocument7 pagesMikropenis NcbiIceBearNo ratings yet
- Ajceu 0072410Document5 pagesAjceu 0072410Azad AhmedNo ratings yet
- Journal Gyn KETDocument8 pagesJournal Gyn KETImaylani S. SitanggangNo ratings yet
- Journal of Drug Discovery and Therapeutics 1 (4) 2013, 01-02Document2 pagesJournal of Drug Discovery and Therapeutics 1 (4) 2013, 01-02Bayu SaputroNo ratings yet
- Successful Laparoscopic Treatment of Intrauterine Device and Complication Causing Uterine RuptureDocument2 pagesSuccessful Laparoscopic Treatment of Intrauterine Device and Complication Causing Uterine Rupturepublishing groupNo ratings yet
- Aps 25 14Document6 pagesAps 25 14Mehul JainNo ratings yet
- Cell Proliferation - 2020 - Yan - Clinical Analysis of Human Umbilical Cord Mesenchymal Stem Cell Allotransplantation inDocument12 pagesCell Proliferation - 2020 - Yan - Clinical Analysis of Human Umbilical Cord Mesenchymal Stem Cell Allotransplantation inJuan FeivelNo ratings yet
- Laparoschisis: About A Case Report and Literature ReviewDocument10 pagesLaparoschisis: About A Case Report and Literature ReviewIJAR JOURNALNo ratings yet
- Timolol in Capillary Hemangioma in InfantDocument8 pagesTimolol in Capillary Hemangioma in InfantIJAR JOURNALNo ratings yet
- Vitiligo ObatDocument6 pagesVitiligo ObatLidwina DewiNo ratings yet
- CharacterDocument5 pagesCharacterYuliaNo ratings yet
- EndometritisDocument6 pagesEndometritisMuh Syarifullah ANo ratings yet
- Van Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournDocument5 pagesVan Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournRonald QuezadaNo ratings yet
- Clinico-Histopathological Study of Endometrium With and Without Hormone Therapy in Patients Withabnormal Uterine BleedingDocument6 pagesClinico-Histopathological Study of Endometrium With and Without Hormone Therapy in Patients Withabnormal Uterine BleedingIJAR JOURNALNo ratings yet
- Post Hysteroscopic Progesterone Hormone Therapy in The Treatment of Endometrial PolypsDocument5 pagesPost Hysteroscopic Progesterone Hormone Therapy in The Treatment of Endometrial PolypsherryNo ratings yet
- Gynecology & Reproductive HealthDocument6 pagesGynecology & Reproductive HealthtiaranindyNo ratings yet
- Admin A 10 1 85 3b9f306Document8 pagesAdmin A 10 1 85 3b9f306Dyanne BautistaNo ratings yet
- Doi 10.4297/najms.2010.2468Document7 pagesDoi 10.4297/najms.2010.2468Bayu Surya DanaNo ratings yet
- Diagnóstico Tardio de MARDocument8 pagesDiagnóstico Tardio de MARthedoctor1986No ratings yet
- Adenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFDocument5 pagesAdenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFPyuzz RemakeNo ratings yet
- Clinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaDocument7 pagesClinical Trends of Ectopic Pregnancy - A Study in A Tertiary Care Hospital of West Bengal, IndiaIJAR JOURNALNo ratings yet
- Craniopharyngioma-The Anesthetic, Critical Care and Syrgical Challenges in The Managemnet of CPNDocument5 pagesCraniopharyngioma-The Anesthetic, Critical Care and Syrgical Challenges in The Managemnet of CPNpitriaNo ratings yet
- Intl J Gynecology Obste - 2023 - Henry - FIGO Statement Fertility PreservationDocument5 pagesIntl J Gynecology Obste - 2023 - Henry - FIGO Statement Fertility Preservationcesarillo85No ratings yet
- Use of High-Dose Chemotherapy in Front-Line TherapDocument8 pagesUse of High-Dose Chemotherapy in Front-Line TherapSri Eka HandayaniNo ratings yet
- HHS Public Access: Management of Clinical Chorioamnionitis: An Evidence-Based ApproachDocument38 pagesHHS Public Access: Management of Clinical Chorioamnionitis: An Evidence-Based ApproachIdmNo ratings yet
- Study of Histopathological Pattern of Thyroid Lesions: International Journal of Biomedical and Advance ResearchDocument10 pagesStudy of Histopathological Pattern of Thyroid Lesions: International Journal of Biomedical and Advance ResearchAprilia Fani PNo ratings yet
- tmpC401 TMPDocument3 pagestmpC401 TMPFrontiersNo ratings yet
- Multiple Choice Questions in Medical Schools: Saudi Medical Journal December 2000Document10 pagesMultiple Choice Questions in Medical Schools: Saudi Medical Journal December 2000RAJESH SHARMANo ratings yet
- Sadeq Saad Abd El Moghny, Ahmed Kaid Allow, Belqees Ahmed and Bracamonte MaryamDocument7 pagesSadeq Saad Abd El Moghny, Ahmed Kaid Allow, Belqees Ahmed and Bracamonte Maryamgamal attamNo ratings yet
- Annals of Medicine and SurgeryDocument5 pagesAnnals of Medicine and SurgeryUsee TvNo ratings yet
- C01110916 PDFDocument8 pagesC01110916 PDFLestari Chye PouedanNo ratings yet
- Surgical Androgen Deprivation Therapy in Advanced Prostate Cancer in Patients of African Descent - Comparison of Biochemical Efficacy of Bilateral Total and Subcapsular OrchidectomyDocument9 pagesSurgical Androgen Deprivation Therapy in Advanced Prostate Cancer in Patients of African Descent - Comparison of Biochemical Efficacy of Bilateral Total and Subcapsular Orchidectomydr.tonichenNo ratings yet
- Hiperplasia EndometrialDocument12 pagesHiperplasia EndometrialJulián LópezNo ratings yet
- Successful Pregnancies in Female Cancer PatientsDocument16 pagesSuccessful Pregnancies in Female Cancer PatientsDolores GalloNo ratings yet
- A Prospective Study of Thyroid Function Test in Geriatric Population and Its Clinical Correlation in A Tertiary Teaching Care CenterDocument4 pagesA Prospective Study of Thyroid Function Test in Geriatric Population and Its Clinical Correlation in A Tertiary Teaching Care CenterLindia PrabhaswariNo ratings yet
- FFDocument238 pagesFFanon-860929100% (1)
- 1st August (Porifera)Document7 pages1st August (Porifera)tayyabuetlhrNo ratings yet
- MCQ On BiomoleculesDocument14 pagesMCQ On BiomoleculesUttkarsha kapoor100% (1)
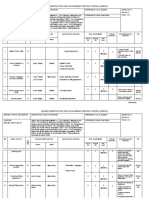
- HIRADC GGC - LiftingDocument3 pagesHIRADC GGC - Liftingfarizal EnterpriseNo ratings yet
- Worship Team Training Session - August 19, 2023Document7 pagesWorship Team Training Session - August 19, 2023Jed B de JesusNo ratings yet
- API EG - USE.ELEC - KH.PC DS2 en Excel v2 4251410Document67 pagesAPI EG - USE.ELEC - KH.PC DS2 en Excel v2 4251410upper paunglaungNo ratings yet
- Explained: Choosing Representation, Mutation, and Crossover in Genetic AlgorithmsDocument2 pagesExplained: Choosing Representation, Mutation, and Crossover in Genetic AlgorithmsJosephNo ratings yet
- Springs Are Fundamental Mechanical Components Found in Many Mechanical SystemsDocument4 pagesSprings Are Fundamental Mechanical Components Found in Many Mechanical SystemsZandro GagoteNo ratings yet
- Mipi-Tutorial PDF CompressedDocument13 pagesMipi-Tutorial PDF CompressedGeorgeNo ratings yet
- Lindo CVDocument1 pageLindo CVfriankylalindoNo ratings yet
- T-88 Structural Aircraft Adhesive: Technical Data SheetDocument2 pagesT-88 Structural Aircraft Adhesive: Technical Data Sheetanon_271015207No ratings yet
- 8 Retained Earnings and Quasi-ReorganizationDocument5 pages8 Retained Earnings and Quasi-ReorganizationNasiba M. AbdulcaderNo ratings yet
- Chapter 2 - Waveguide PDFDocument38 pagesChapter 2 - Waveguide PDFHiroshi RayNo ratings yet
- Cargoes PDFDocument2 pagesCargoes PDFnabaa sadiqNo ratings yet
- Info Pompe Pistonase PDFDocument44 pagesInfo Pompe Pistonase PDFMarin GarazNo ratings yet
- 36106901Document380 pages36106901thunderbox550% (2)
- 11 English Mixed Test Paper 02Document4 pages11 English Mixed Test Paper 02Robin AhujaNo ratings yet
- Two Separate WorldsDocument14 pagesTwo Separate WorldsmaryfeNo ratings yet
- Feed Formulation Manual 2017Document40 pagesFeed Formulation Manual 2017Jennifer Legaspi86% (7)
- Instruction Manual Il-Obct-R1: Slip-Over Current Transformer ObctDocument2 pagesInstruction Manual Il-Obct-R1: Slip-Over Current Transformer Obctبوحميدة كمالNo ratings yet
- Mozakkir Mohammad Jamil - Oracle HCM Techno Functional ConsultantDocument9 pagesMozakkir Mohammad Jamil - Oracle HCM Techno Functional Consultantعبدالرحمن فؤادNo ratings yet
- 2 PACK - DIRECTV Broadband DECA Ethernet To Coax Adapter - Third Generation (With 2 USB Power Cables)Document2 pages2 PACK - DIRECTV Broadband DECA Ethernet To Coax Adapter - Third Generation (With 2 USB Power Cables)Satheesh VenkataNo ratings yet
- Noncavernous Arteriovenous Shunts Mimicking Carotid Cavernous FistulaeDocument5 pagesNoncavernous Arteriovenous Shunts Mimicking Carotid Cavernous FistulaeClarithq LengguNo ratings yet
- Antecedentes 2Document26 pagesAntecedentes 2Carlos Mario Ortiz MuñozNo ratings yet
- 1kd FTV Rev 2 PDFDocument45 pages1kd FTV Rev 2 PDFEder BarreirosNo ratings yet
- Architectural Fasteners & Fittings - Stainless Steel - AnzorDocument18 pagesArchitectural Fasteners & Fittings - Stainless Steel - AnzorBhaiJan59No ratings yet
- EBS Period Close Analyzer-CompressedDocument29 pagesEBS Period Close Analyzer-CompressedRaoof AhmedNo ratings yet