
E News Vol 3 Issue 1
E News Vol 3 Issue 1
You might also like
- Yasser El Miedany Musculoskeletal Ultrasound Guided RegenerativeDocument554 pagesYasser El Miedany Musculoskeletal Ultrasound Guided RegenerativeMarielly EllerNo ratings yet
- The Road To Pass PrometricDocument460 pagesThe Road To Pass PrometricMuhammad FahmyNo ratings yet
- MSBTE Diploma Project Report TempletDocument8 pagesMSBTE Diploma Project Report Templet53 Hirole Aadesh100% (5)
- AI Architectures A Culinary GuideDocument30 pagesAI Architectures A Culinary GuideskyonNo ratings yet
- Maximum Pain Relief with Your TENS Unit: Easy, Drug-Free Techniques for Treating Chronic Pain, Muscle Injuries and Common Ailments at HomeFrom EverandMaximum Pain Relief with Your TENS Unit: Easy, Drug-Free Techniques for Treating Chronic Pain, Muscle Injuries and Common Ailments at HomeNo ratings yet
- Self Assessment in Axial Skeleton Musculoskeletal Trauma X-raysFrom EverandSelf Assessment in Axial Skeleton Musculoskeletal Trauma X-raysRating: 5 out of 5 stars5/5 (2)
- Foundations of International Law: History, Nature, Sources, AnswersDocument65 pagesFoundations of International Law: History, Nature, Sources, AnswersGromobranNo ratings yet
- Skewed CoordinatesDocument22 pagesSkewed Coordinatesstoimie100% (1)
- E News Vol 3 Issue 2Document16 pagesE News Vol 3 Issue 2Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 4Document22 pagesE News Vol 2 Issue 4Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 3Document13 pagesE News Vol 2 Issue 3Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 1Document8 pagesE News Vol 2 Issue 1Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 2Document11 pagesE News Vol 2 Issue 2Muhammad FahmyNo ratings yet
- Tim Watson Chapter 6Document15 pagesTim Watson Chapter 6krista100717No ratings yet
- E News Vol 1 Issue 2Document5 pagesE News Vol 1 Issue 2Muhammad FahmyNo ratings yet
- 1 s2.0 S0004951414610059 Main PDFDocument10 pages1 s2.0 S0004951414610059 Main PDFIkramul Hussain KhanNo ratings yet
- Abat 2016Document8 pagesAbat 2016toaldoNo ratings yet
- E News Vol 3 Issue 4Document19 pagesE News Vol 3 Issue 4ebookNo ratings yet
- Tens Us Ic Neck PainDocument5 pagesTens Us Ic Neck PainMahnoor AqeelNo ratings yet
- Ultrasound Thesis TopicsDocument6 pagesUltrasound Thesis Topicsdw9x1bxb100% (2)
- Ebm in Ultrasounds and Schock WavesDocument35 pagesEbm in Ultrasounds and Schock Wavessabina vladeanuNo ratings yet
- Rasmussen 2008. SWT Chronic Achilles Tendinopathy. A Double-Blind Randomized Clinical Trial of EfficacyDocument9 pagesRasmussen 2008. SWT Chronic Achilles Tendinopathy. A Double-Blind Randomized Clinical Trial of EfficacyJavier MartinNo ratings yet
- Musculoskeletal EMF TreatmentDocument16 pagesMusculoskeletal EMF Treatmentdrmarwayaseen85No ratings yet
- Use of Neuromuscular Electrical Stimulation in The Treatment of Neonatal Brachial Plexus Palsy: A Literature ReviewDocument13 pagesUse of Neuromuscular Electrical Stimulation in The Treatment of Neonatal Brachial Plexus Palsy: A Literature ReviewRock RockkNo ratings yet
- Therapeutic Ultrasound Research PaperDocument6 pagesTherapeutic Ultrasound Research Paperwrglrkrhf100% (1)
- 2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyDocument25 pages2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyAni Fran SolarNo ratings yet
- Shockwave May 2014Document13 pagesShockwave May 2014Mskola Karlovac100% (1)
- Treatment of Temporomandibular Disorder Using Synergistic Laser Andultrasound ApplicationDocument6 pagesTreatment of Temporomandibular Disorder Using Synergistic Laser Andultrasound ApplicationMohamed FaizalNo ratings yet
- Ij2023 14Document7 pagesIj2023 14Julenda CintarinovaNo ratings yet
- Clinical Applications of Acupuncture: An Overview of The EvidenceDocument8 pagesClinical Applications of Acupuncture: An Overview of The EvidenceAntonio ANo ratings yet
- Extracorporeal Shockwave TherapyDocument1 pageExtracorporeal Shockwave Therapywr48f26rjmNo ratings yet
- Model of ElectrotherapyDocument11 pagesModel of ElectrotherapykapilphysioNo ratings yet
- Ian's Update Newsletter: Ultrasound Procedures-Time To Start Respecting The Guide-Lines?Document10 pagesIan's Update Newsletter: Ultrasound Procedures-Time To Start Respecting The Guide-Lines?salsa0479No ratings yet
- Agentes ElectrofisicosDocument10 pagesAgentes Electrofisicososcar eduardo mateus ariasNo ratings yet
- Therapeutic UltrasoundDocument18 pagesTherapeutic UltrasoundPhysio Ebook100% (1)
- Kelompok 2Document23 pagesKelompok 2lutfiah nabilahNo ratings yet
- Effects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialDocument14 pagesEffects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialLorena Rico ArtigasNo ratings yet
- SE Magnet TherapyDocument4 pagesSE Magnet TherapyDionisCebanNo ratings yet
- Mechanisms of TENSDocument13 pagesMechanisms of TENSOana Budugan0% (1)
- TENS Literature - Review - and - Meta - Analysis - Of.99266Document9 pagesTENS Literature - Review - and - Meta - Analysis - Of.99266Adam ForshawNo ratings yet
- Ultrasound and Laser As Stand-Alone Therapies For Myofascial Trigger Points: A Randomized, Double-Blind, Placebo-Controlled StudyDocument10 pagesUltrasound and Laser As Stand-Alone Therapies For Myofascial Trigger Points: A Randomized, Double-Blind, Placebo-Controlled StudyVikborn TjgNo ratings yet
- Chen 2013Document5 pagesChen 2013RenaldiPrimaSaputraNo ratings yet
- Alexander 2009Document14 pagesAlexander 2009Emiliano SterliNo ratings yet
- Ryodoraku 2Document7 pagesRyodoraku 2Alexandre ManentiNo ratings yet
- 4 Way Analysis of Body Talk Technique On Body and Energy FieldsDocument86 pages4 Way Analysis of Body Talk Technique On Body and Energy FieldssohailuddinNo ratings yet
- VibrationDocument11 pagesVibrationFernando BrantalikNo ratings yet
- Dissertation TmsDocument4 pagesDissertation TmsBuyPsychologyPapersUK100% (1)
- ISMST Shockwave Medical Papers 2012Document24 pagesISMST Shockwave Medical Papers 2012Dr-Gehad Samy Halwagy100% (1)
- Artigo - US Pra Dor CrônicaDocument12 pagesArtigo - US Pra Dor CrônicaJose Carlos CamposNo ratings yet
- Atlases of Clinical Nuclear Medicine: Series Editor: Douglas Van NostrandDocument149 pagesAtlases of Clinical Nuclear Medicine: Series Editor: Douglas Van NostrandNeide CarvalhoNo ratings yet
- Journal ESWT Pada DewasaDocument7 pagesJournal ESWT Pada DewasaPhilipusHendryHartonoNo ratings yet
- Low Back PainDocument6 pagesLow Back PainMuhammad Adzan Al QadriNo ratings yet
- A Multicentre Randomized Controlled Follow-Up Study of The Effects of The Underwater Traction Therapy in Chronic Low Back PainDocument8 pagesA Multicentre Randomized Controlled Follow-Up Study of The Effects of The Underwater Traction Therapy in Chronic Low Back PainhanifahNo ratings yet
- Manual of Diagnostic Imaging Musculoskeletal SystemDocument211 pagesManual of Diagnostic Imaging Musculoskeletal SystemKatiasal100% (1)
- Key Concepts With EPAs 2021Document10 pagesKey Concepts With EPAs 2021Syed Abdul HafeezNo ratings yet
- Tens PDFDocument62 pagesTens PDFJay Muhammad100% (1)
- Low Level Laser Therapy (LLLT) and World Association For Laser Therapy (WALT) Dosage RecommendationsDocument4 pagesLow Level Laser Therapy (LLLT) and World Association For Laser Therapy (WALT) Dosage RecommendationsChung Tze YangNo ratings yet
- ElectroMedicine From The Rife Hand Book of FrequencyDocument17 pagesElectroMedicine From The Rife Hand Book of FrequencySean MoonshineNo ratings yet
- The Effectiveness of Electroconvulsive TDocument15 pagesThe Effectiveness of Electroconvulsive TEd WrightNo ratings yet
- The Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyDocument8 pagesThe Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyAlexandra-Andreea BroascăNo ratings yet
- Editorial: Whole Lotta Shakin' Goin' OnDocument3 pagesEditorial: Whole Lotta Shakin' Goin' OndfhvjNo ratings yet
- Practice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyFrom EverandPractice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyRating: 5 out of 5 stars5/5 (1)
- Pain Imaging: A Clinical-Radiological Approach to Pain DiagnosisFrom EverandPain Imaging: A Clinical-Radiological Approach to Pain DiagnosisMaria Assunta CovaNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Laser TherapyDocument6 pagesLaser TherapyMuhammad FahmyNo ratings yet
- E News Vol 3 Issue 2Document16 pagesE News Vol 3 Issue 2Muhammad FahmyNo ratings yet
- Transcutaneous Electrical Nerve Stimulation Basic ScienceDocument13 pagesTranscutaneous Electrical Nerve Stimulation Basic ScienceMuhammad FahmyNo ratings yet
- Biomechanics-Lumbar Facet Pain Biomechanics, Neuroanatomy and NeurophysiologyDocument13 pagesBiomechanics-Lumbar Facet Pain Biomechanics, Neuroanatomy and NeurophysiologyMuhammad FahmyNo ratings yet
- Biomechanics05 001Document72 pagesBiomechanics05 001Muhammad FahmyNo ratings yet
- Emg 1211.2017Document20 pagesEmg 1211.2017Muhammad FahmyNo ratings yet
- Biomechanics of Soft TissuesDocument10 pagesBiomechanics of Soft TissuesMuhammad FahmyNo ratings yet
- Self Myofascial ReleaseDocument22 pagesSelf Myofascial ReleaseMuhammad Fahmy100% (1)
- Article Perfect Posture PuzzleDocument6 pagesArticle Perfect Posture PuzzleMuhammad FahmyNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- Biomechanics of Craniofacial Sutures Orthopedic ImplicationsDocument8 pagesBiomechanics of Craniofacial Sutures Orthopedic ImplicationsMuhammad FahmyNo ratings yet
- Neurological ExaminationDocument23 pagesNeurological ExaminationMuhammad Fahmy100% (1)
- KneeDocument24 pagesKneeMuhammad Fahmy100% (1)
- Joel Bialosky UFDocument28 pagesJoel Bialosky UFMuhammad FahmyNo ratings yet
- LungDocument20 pagesLungMuhammad Fahmy100% (1)
- TractionDocument21 pagesTractionMuhammad FahmyNo ratings yet
- The Role of Manual Therapy in Headache ManagementDocument36 pagesThe Role of Manual Therapy in Headache ManagementMuhammad FahmyNo ratings yet
- Shoulder ExamDocument24 pagesShoulder ExamMuhammad FahmyNo ratings yet
- Scan (718) 20180921191026Document2 pagesScan (718) 20180921191026Muhammad FahmyNo ratings yet
- Chapter 4 - CORE STRENGTHENING FOR GOLFDocument10 pagesChapter 4 - CORE STRENGTHENING FOR GOLFMuhammad FahmyNo ratings yet
- Pal ElbowDocument8 pagesPal ElbowMuhammad FahmyNo ratings yet
- Clinical InstructorsDocument1 pageClinical InstructorsMuhammad FahmyNo ratings yet
- ملزمة محمد مرعي الشاملهDocument98 pagesملزمة محمد مرعي الشاملهMuhammad FahmyNo ratings yet
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyNo ratings yet
- AbdomenDocument18 pagesAbdomenMuhammad FahmyNo ratings yet
- Upper Extremity Exercise Program: Patient Information BookletDocument8 pagesUpper Extremity Exercise Program: Patient Information BookletMuhammad FahmyNo ratings yet
- Wrist HandDocument10 pagesWrist HandMuhammad FahmyNo ratings yet
- Video Transcript-Principles of ArtDocument2 pagesVideo Transcript-Principles of ArtJanine GelagaNo ratings yet
- Normal and Abnormal Characteristic of SputumDocument2 pagesNormal and Abnormal Characteristic of SputumKim Chamos100% (2)
- The ABCs of DR Desmond Ford S Theology W H JohnsDocument16 pagesThe ABCs of DR Desmond Ford S Theology W H JohnsBogdan PlaticaNo ratings yet
- Modern Music in ChileDocument6 pagesModern Music in Chilemaru717No ratings yet
- Proceedings of The Sixth IEEE International Conference On Fuzzy Systems - Volume IDocument20 pagesProceedings of The Sixth IEEE International Conference On Fuzzy Systems - Volume IFrancisca SotoNo ratings yet
- Flight1 441 Conquest TutorialDocument10 pagesFlight1 441 Conquest TutorialJosé A. Montiel QuirósNo ratings yet
- 1 PBDocument7 pages1 PBIdhamNo ratings yet
- Extended Essay IB DiplomaDocument20 pagesExtended Essay IB Diplomasol GonzalezNo ratings yet
- P3. Farmakoterapi Penyakit Gangguan EndokrinDocument84 pagesP3. Farmakoterapi Penyakit Gangguan EndokrinRidzal Ade PutraNo ratings yet
- Mechanics For Tiktok ChallengeDocument7 pagesMechanics For Tiktok ChallengeSCSC PE2No ratings yet
- Math G 5 Model Paper Part ADocument4 pagesMath G 5 Model Paper Part Aapi-251341286No ratings yet
- Understanding Second Life As An Extension of OurselvesDocument19 pagesUnderstanding Second Life As An Extension of OurselvesgloriagdiagoNo ratings yet
- THE UlTIMATE SAFARIDocument5 pagesTHE UlTIMATE SAFARIapi-19776105100% (1)
- 011 - Descriptive Writing - UpdatedDocument39 pages011 - Descriptive Writing - UpdatedLeroy ChengNo ratings yet
- 00b. 華文1課程介紹 (網上教學)Document16 pages00b. 華文1課程介紹 (網上教學)Lukmanul HakimNo ratings yet
- Course Code: 5653-01 Programme: M.L.I.S: Assignment No. 1Document14 pagesCourse Code: 5653-01 Programme: M.L.I.S: Assignment No. 1Qazi zubairNo ratings yet
- African Language PoliciesDocument121 pagesAfrican Language PoliciesBradNo ratings yet
- India Since Independence NotesDocument8 pagesIndia Since Independence NotesDilip PanchalNo ratings yet
- Mth601 (19 Files Merged)Document490 pagesMth601 (19 Files Merged)Hafsa Dawood100% (1)
- Adverbs of Quantity & FrequencyDocument1 pageAdverbs of Quantity & FrequencyIngenieria Ejecuciòn en Prevenciòn de Riegos 2021No ratings yet
- BM Wed Wild LordDocument2 pagesBM Wed Wild Lordcori sabauNo ratings yet
- Basic Electrical Circuits DR Nagendra Krishnapura Department of Electrical Engineering Indian Institute of Technology Madras Lecture - 01Document2 pagesBasic Electrical Circuits DR Nagendra Krishnapura Department of Electrical Engineering Indian Institute of Technology Madras Lecture - 01Ranjeet Singh BishtNo ratings yet
- Chess Game RelatedDocument6 pagesChess Game RelatedSakthi Suba RajaNo ratings yet
- 10 Basic Elements of Visual DesignDocument2 pages10 Basic Elements of Visual DesignsunshinesunshineNo ratings yet
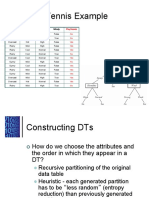
- Play Tennis Example: Outlook Temperature Humidity WindyDocument29 pagesPlay Tennis Example: Outlook Temperature Humidity Windyioi123No ratings yet
- Syllabus African Politics Fall2020Document15 pagesSyllabus African Politics Fall2020gusNo ratings yet




















































































































Download as pdf or txt
You might also like
- Yasser El Miedany Musculoskeletal Ultrasound Guided RegenerativeDocument554 pagesYasser El Miedany Musculoskeletal Ultrasound Guided RegenerativeMarielly EllerNo ratings yet
- The Road To Pass PrometricDocument460 pagesThe Road To Pass PrometricMuhammad FahmyNo ratings yet
- MSBTE Diploma Project Report TempletDocument8 pagesMSBTE Diploma Project Report Templet53 Hirole Aadesh100% (5)
- AI Architectures A Culinary GuideDocument30 pagesAI Architectures A Culinary GuideskyonNo ratings yet
- Maximum Pain Relief with Your TENS Unit: Easy, Drug-Free Techniques for Treating Chronic Pain, Muscle Injuries and Common Ailments at HomeFrom EverandMaximum Pain Relief with Your TENS Unit: Easy, Drug-Free Techniques for Treating Chronic Pain, Muscle Injuries and Common Ailments at HomeNo ratings yet
- Self Assessment in Axial Skeleton Musculoskeletal Trauma X-raysFrom EverandSelf Assessment in Axial Skeleton Musculoskeletal Trauma X-raysRating: 5 out of 5 stars5/5 (2)
- Foundations of International Law: History, Nature, Sources, AnswersDocument65 pagesFoundations of International Law: History, Nature, Sources, AnswersGromobranNo ratings yet
- Skewed CoordinatesDocument22 pagesSkewed Coordinatesstoimie100% (1)
- E News Vol 3 Issue 2Document16 pagesE News Vol 3 Issue 2Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 4Document22 pagesE News Vol 2 Issue 4Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 3Document13 pagesE News Vol 2 Issue 3Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 1Document8 pagesE News Vol 2 Issue 1Muhammad FahmyNo ratings yet
- E News Vol 2 Issue 2Document11 pagesE News Vol 2 Issue 2Muhammad FahmyNo ratings yet
- Tim Watson Chapter 6Document15 pagesTim Watson Chapter 6krista100717No ratings yet
- E News Vol 1 Issue 2Document5 pagesE News Vol 1 Issue 2Muhammad FahmyNo ratings yet
- 1 s2.0 S0004951414610059 Main PDFDocument10 pages1 s2.0 S0004951414610059 Main PDFIkramul Hussain KhanNo ratings yet
- Abat 2016Document8 pagesAbat 2016toaldoNo ratings yet
- E News Vol 3 Issue 4Document19 pagesE News Vol 3 Issue 4ebookNo ratings yet
- Tens Us Ic Neck PainDocument5 pagesTens Us Ic Neck PainMahnoor AqeelNo ratings yet
- Ultrasound Thesis TopicsDocument6 pagesUltrasound Thesis Topicsdw9x1bxb100% (2)
- Ebm in Ultrasounds and Schock WavesDocument35 pagesEbm in Ultrasounds and Schock Wavessabina vladeanuNo ratings yet
- Rasmussen 2008. SWT Chronic Achilles Tendinopathy. A Double-Blind Randomized Clinical Trial of EfficacyDocument9 pagesRasmussen 2008. SWT Chronic Achilles Tendinopathy. A Double-Blind Randomized Clinical Trial of EfficacyJavier MartinNo ratings yet
- Musculoskeletal EMF TreatmentDocument16 pagesMusculoskeletal EMF Treatmentdrmarwayaseen85No ratings yet
- Use of Neuromuscular Electrical Stimulation in The Treatment of Neonatal Brachial Plexus Palsy: A Literature ReviewDocument13 pagesUse of Neuromuscular Electrical Stimulation in The Treatment of Neonatal Brachial Plexus Palsy: A Literature ReviewRock RockkNo ratings yet
- Therapeutic Ultrasound Research PaperDocument6 pagesTherapeutic Ultrasound Research Paperwrglrkrhf100% (1)
- 2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyDocument25 pages2014 Effectiveness of Continuous Vertebral Resonant Oscillation Using The POLD Method in The Treatment of Lumbar Disc Hernia. A Randomized Controlled Pilot StudyAni Fran SolarNo ratings yet
- Shockwave May 2014Document13 pagesShockwave May 2014Mskola Karlovac100% (1)
- Treatment of Temporomandibular Disorder Using Synergistic Laser Andultrasound ApplicationDocument6 pagesTreatment of Temporomandibular Disorder Using Synergistic Laser Andultrasound ApplicationMohamed FaizalNo ratings yet
- Ij2023 14Document7 pagesIj2023 14Julenda CintarinovaNo ratings yet
- Clinical Applications of Acupuncture: An Overview of The EvidenceDocument8 pagesClinical Applications of Acupuncture: An Overview of The EvidenceAntonio ANo ratings yet
- Extracorporeal Shockwave TherapyDocument1 pageExtracorporeal Shockwave Therapywr48f26rjmNo ratings yet
- Model of ElectrotherapyDocument11 pagesModel of ElectrotherapykapilphysioNo ratings yet
- Ian's Update Newsletter: Ultrasound Procedures-Time To Start Respecting The Guide-Lines?Document10 pagesIan's Update Newsletter: Ultrasound Procedures-Time To Start Respecting The Guide-Lines?salsa0479No ratings yet
- Agentes ElectrofisicosDocument10 pagesAgentes Electrofisicososcar eduardo mateus ariasNo ratings yet
- Therapeutic UltrasoundDocument18 pagesTherapeutic UltrasoundPhysio Ebook100% (1)
- Kelompok 2Document23 pagesKelompok 2lutfiah nabilahNo ratings yet
- Effects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialDocument14 pagesEffects of Transcutaneous Electrical Nerve Stimulation On Pain Pain Sensitivity and Function in People With Knee Osteoarthritis. A Randomized Controlled TrialLorena Rico ArtigasNo ratings yet
- SE Magnet TherapyDocument4 pagesSE Magnet TherapyDionisCebanNo ratings yet
- Mechanisms of TENSDocument13 pagesMechanisms of TENSOana Budugan0% (1)
- TENS Literature - Review - and - Meta - Analysis - Of.99266Document9 pagesTENS Literature - Review - and - Meta - Analysis - Of.99266Adam ForshawNo ratings yet
- Ultrasound and Laser As Stand-Alone Therapies For Myofascial Trigger Points: A Randomized, Double-Blind, Placebo-Controlled StudyDocument10 pagesUltrasound and Laser As Stand-Alone Therapies For Myofascial Trigger Points: A Randomized, Double-Blind, Placebo-Controlled StudyVikborn TjgNo ratings yet
- Chen 2013Document5 pagesChen 2013RenaldiPrimaSaputraNo ratings yet
- Alexander 2009Document14 pagesAlexander 2009Emiliano SterliNo ratings yet
- Ryodoraku 2Document7 pagesRyodoraku 2Alexandre ManentiNo ratings yet
- 4 Way Analysis of Body Talk Technique On Body and Energy FieldsDocument86 pages4 Way Analysis of Body Talk Technique On Body and Energy FieldssohailuddinNo ratings yet
- VibrationDocument11 pagesVibrationFernando BrantalikNo ratings yet
- Dissertation TmsDocument4 pagesDissertation TmsBuyPsychologyPapersUK100% (1)
- ISMST Shockwave Medical Papers 2012Document24 pagesISMST Shockwave Medical Papers 2012Dr-Gehad Samy Halwagy100% (1)
- Artigo - US Pra Dor CrônicaDocument12 pagesArtigo - US Pra Dor CrônicaJose Carlos CamposNo ratings yet
- Atlases of Clinical Nuclear Medicine: Series Editor: Douglas Van NostrandDocument149 pagesAtlases of Clinical Nuclear Medicine: Series Editor: Douglas Van NostrandNeide CarvalhoNo ratings yet
- Journal ESWT Pada DewasaDocument7 pagesJournal ESWT Pada DewasaPhilipusHendryHartonoNo ratings yet
- Low Back PainDocument6 pagesLow Back PainMuhammad Adzan Al QadriNo ratings yet
- A Multicentre Randomized Controlled Follow-Up Study of The Effects of The Underwater Traction Therapy in Chronic Low Back PainDocument8 pagesA Multicentre Randomized Controlled Follow-Up Study of The Effects of The Underwater Traction Therapy in Chronic Low Back PainhanifahNo ratings yet
- Manual of Diagnostic Imaging Musculoskeletal SystemDocument211 pagesManual of Diagnostic Imaging Musculoskeletal SystemKatiasal100% (1)
- Key Concepts With EPAs 2021Document10 pagesKey Concepts With EPAs 2021Syed Abdul HafeezNo ratings yet
- Tens PDFDocument62 pagesTens PDFJay Muhammad100% (1)
- Low Level Laser Therapy (LLLT) and World Association For Laser Therapy (WALT) Dosage RecommendationsDocument4 pagesLow Level Laser Therapy (LLLT) and World Association For Laser Therapy (WALT) Dosage RecommendationsChung Tze YangNo ratings yet
- ElectroMedicine From The Rife Hand Book of FrequencyDocument17 pagesElectroMedicine From The Rife Hand Book of FrequencySean MoonshineNo ratings yet
- The Effectiveness of Electroconvulsive TDocument15 pagesThe Effectiveness of Electroconvulsive TEd WrightNo ratings yet
- The Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyDocument8 pagesThe Effect of Electroacupuncture Merged With Rehabilitation For Frozen Shoulder Syndrome: A Single-Blind Randomized Sham-Acupuncture Controlled StudyAlexandra-Andreea BroascăNo ratings yet
- Editorial: Whole Lotta Shakin' Goin' OnDocument3 pagesEditorial: Whole Lotta Shakin' Goin' OndfhvjNo ratings yet
- Practice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyFrom EverandPractice Of Osteopathy - Its Practical Application To The Various Diseases Of The Human BodyRating: 5 out of 5 stars5/5 (1)
- Pain Imaging: A Clinical-Radiological Approach to Pain DiagnosisFrom EverandPain Imaging: A Clinical-Radiological Approach to Pain DiagnosisMaria Assunta CovaNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Laser TherapyDocument6 pagesLaser TherapyMuhammad FahmyNo ratings yet
- E News Vol 3 Issue 2Document16 pagesE News Vol 3 Issue 2Muhammad FahmyNo ratings yet
- Transcutaneous Electrical Nerve Stimulation Basic ScienceDocument13 pagesTranscutaneous Electrical Nerve Stimulation Basic ScienceMuhammad FahmyNo ratings yet
- Biomechanics-Lumbar Facet Pain Biomechanics, Neuroanatomy and NeurophysiologyDocument13 pagesBiomechanics-Lumbar Facet Pain Biomechanics, Neuroanatomy and NeurophysiologyMuhammad FahmyNo ratings yet
- Biomechanics05 001Document72 pagesBiomechanics05 001Muhammad FahmyNo ratings yet
- Emg 1211.2017Document20 pagesEmg 1211.2017Muhammad FahmyNo ratings yet
- Biomechanics of Soft TissuesDocument10 pagesBiomechanics of Soft TissuesMuhammad FahmyNo ratings yet
- Self Myofascial ReleaseDocument22 pagesSelf Myofascial ReleaseMuhammad Fahmy100% (1)
- Article Perfect Posture PuzzleDocument6 pagesArticle Perfect Posture PuzzleMuhammad FahmyNo ratings yet
- Low BackDocument7 pagesLow BackMuhammad FahmyNo ratings yet
- Biomechanics of Craniofacial Sutures Orthopedic ImplicationsDocument8 pagesBiomechanics of Craniofacial Sutures Orthopedic ImplicationsMuhammad FahmyNo ratings yet
- Neurological ExaminationDocument23 pagesNeurological ExaminationMuhammad Fahmy100% (1)
- KneeDocument24 pagesKneeMuhammad Fahmy100% (1)
- Joel Bialosky UFDocument28 pagesJoel Bialosky UFMuhammad FahmyNo ratings yet
- LungDocument20 pagesLungMuhammad Fahmy100% (1)
- TractionDocument21 pagesTractionMuhammad FahmyNo ratings yet
- The Role of Manual Therapy in Headache ManagementDocument36 pagesThe Role of Manual Therapy in Headache ManagementMuhammad FahmyNo ratings yet
- Shoulder ExamDocument24 pagesShoulder ExamMuhammad FahmyNo ratings yet
- Scan (718) 20180921191026Document2 pagesScan (718) 20180921191026Muhammad FahmyNo ratings yet
- Chapter 4 - CORE STRENGTHENING FOR GOLFDocument10 pagesChapter 4 - CORE STRENGTHENING FOR GOLFMuhammad FahmyNo ratings yet
- Pal ElbowDocument8 pagesPal ElbowMuhammad FahmyNo ratings yet
- Clinical InstructorsDocument1 pageClinical InstructorsMuhammad FahmyNo ratings yet
- ملزمة محمد مرعي الشاملهDocument98 pagesملزمة محمد مرعي الشاملهMuhammad FahmyNo ratings yet
- Vital SignsDocument10 pagesVital SignsMuhammad FahmyNo ratings yet
- AbdomenDocument18 pagesAbdomenMuhammad FahmyNo ratings yet
- Upper Extremity Exercise Program: Patient Information BookletDocument8 pagesUpper Extremity Exercise Program: Patient Information BookletMuhammad FahmyNo ratings yet
- Wrist HandDocument10 pagesWrist HandMuhammad FahmyNo ratings yet
- Video Transcript-Principles of ArtDocument2 pagesVideo Transcript-Principles of ArtJanine GelagaNo ratings yet
- Normal and Abnormal Characteristic of SputumDocument2 pagesNormal and Abnormal Characteristic of SputumKim Chamos100% (2)
- The ABCs of DR Desmond Ford S Theology W H JohnsDocument16 pagesThe ABCs of DR Desmond Ford S Theology W H JohnsBogdan PlaticaNo ratings yet
- Modern Music in ChileDocument6 pagesModern Music in Chilemaru717No ratings yet
- Proceedings of The Sixth IEEE International Conference On Fuzzy Systems - Volume IDocument20 pagesProceedings of The Sixth IEEE International Conference On Fuzzy Systems - Volume IFrancisca SotoNo ratings yet
- Flight1 441 Conquest TutorialDocument10 pagesFlight1 441 Conquest TutorialJosé A. Montiel QuirósNo ratings yet
- 1 PBDocument7 pages1 PBIdhamNo ratings yet
- Extended Essay IB DiplomaDocument20 pagesExtended Essay IB Diplomasol GonzalezNo ratings yet
- P3. Farmakoterapi Penyakit Gangguan EndokrinDocument84 pagesP3. Farmakoterapi Penyakit Gangguan EndokrinRidzal Ade PutraNo ratings yet
- Mechanics For Tiktok ChallengeDocument7 pagesMechanics For Tiktok ChallengeSCSC PE2No ratings yet
- Math G 5 Model Paper Part ADocument4 pagesMath G 5 Model Paper Part Aapi-251341286No ratings yet
- Understanding Second Life As An Extension of OurselvesDocument19 pagesUnderstanding Second Life As An Extension of OurselvesgloriagdiagoNo ratings yet
- THE UlTIMATE SAFARIDocument5 pagesTHE UlTIMATE SAFARIapi-19776105100% (1)
- 011 - Descriptive Writing - UpdatedDocument39 pages011 - Descriptive Writing - UpdatedLeroy ChengNo ratings yet
- 00b. 華文1課程介紹 (網上教學)Document16 pages00b. 華文1課程介紹 (網上教學)Lukmanul HakimNo ratings yet
- Course Code: 5653-01 Programme: M.L.I.S: Assignment No. 1Document14 pagesCourse Code: 5653-01 Programme: M.L.I.S: Assignment No. 1Qazi zubairNo ratings yet
- African Language PoliciesDocument121 pagesAfrican Language PoliciesBradNo ratings yet
- India Since Independence NotesDocument8 pagesIndia Since Independence NotesDilip PanchalNo ratings yet
- Mth601 (19 Files Merged)Document490 pagesMth601 (19 Files Merged)Hafsa Dawood100% (1)
- Adverbs of Quantity & FrequencyDocument1 pageAdverbs of Quantity & FrequencyIngenieria Ejecuciòn en Prevenciòn de Riegos 2021No ratings yet
- BM Wed Wild LordDocument2 pagesBM Wed Wild Lordcori sabauNo ratings yet
- Basic Electrical Circuits DR Nagendra Krishnapura Department of Electrical Engineering Indian Institute of Technology Madras Lecture - 01Document2 pagesBasic Electrical Circuits DR Nagendra Krishnapura Department of Electrical Engineering Indian Institute of Technology Madras Lecture - 01Ranjeet Singh BishtNo ratings yet
- Chess Game RelatedDocument6 pagesChess Game RelatedSakthi Suba RajaNo ratings yet
- 10 Basic Elements of Visual DesignDocument2 pages10 Basic Elements of Visual DesignsunshinesunshineNo ratings yet
- Play Tennis Example: Outlook Temperature Humidity WindyDocument29 pagesPlay Tennis Example: Outlook Temperature Humidity Windyioi123No ratings yet
- Syllabus African Politics Fall2020Document15 pagesSyllabus African Politics Fall2020gusNo ratings yet