Download as pdf or txt
You might also like
- Rutina Hipertrofia Mike IsraetelDocument24 pagesRutina Hipertrofia Mike Israetelyorman santamariaNo ratings yet
- The Card Magic of Edward Marlo PDFDocument250 pagesThe Card Magic of Edward Marlo PDFMatthew McCoy100% (19)
- Supraspinatus TendinitisDocument7 pagesSupraspinatus Tendinitismilananand100% (1)
- Atlas of Nerve Conduction Studies and ElectromyographyDocument326 pagesAtlas of Nerve Conduction Studies and ElectromyographySalazar Ángel100% (13)
- Clinical Anatomy Maxillary ArteryDocument7 pagesClinical Anatomy Maxillary ArteryNivedha AvoodaiappanNo ratings yet
- Master Anatomy ChartDocument21 pagesMaster Anatomy ChartMonica Moya100% (5)
- Retro Molar Ref GionDocument6 pagesRetro Molar Ref GionAulia Nawa FadillahNo ratings yet
- Erdogmus Et Al 2014 - BonesDocument8 pagesErdogmus Et Al 2014 - Bonesmattlight07No ratings yet
- Bilateral Double Parotid Ducts A Case Report (#316531) - 371025Document3 pagesBilateral Double Parotid Ducts A Case Report (#316531) - 371025Evaristo GomesNo ratings yet
- Morphometric Study of Foramen Magnum at The Base of Human Skull in South GujaratDocument3 pagesMorphometric Study of Foramen Magnum at The Base of Human Skull in South GujaratInternational Organization of Scientific Research (IOSR)No ratings yet
- Morphometric Study of Supratrochlear Foramen of The Humerus Related With Clinical Implications in A Thai PopulationDocument6 pagesMorphometric Study of Supratrochlear Foramen of The Humerus Related With Clinical Implications in A Thai PopulationAbner PortilhoNo ratings yet
- 11 Jatin EtalDocument4 pages11 Jatin EtaleditorijmrhsNo ratings yet
- Dimensions and Morphology of The Sinus Tympani: An Anatomical StudyDocument4 pagesDimensions and Morphology of The Sinus Tympani: An Anatomical StudyKennedy NgoseyweNo ratings yet
- Art 08Document7 pagesArt 08Orangzaib OrangzaibNo ratings yet
- Ymj 49 1004Document5 pagesYmj 49 1004Ottofianus Hewick KalangiNo ratings yet
- 1728 PDFDocument3 pages1728 PDFDeepak NaiduNo ratings yet
- The Deltoid Muscle: An Anatomic Description of The Deltoid Insertion To The Proximal HumerusDocument3 pagesThe Deltoid Muscle: An Anatomic Description of The Deltoid Insertion To The Proximal HumerusDeepak NaiduNo ratings yet
- Bio Meth RicsDocument4 pagesBio Meth RicsAulia Nawa FadillahNo ratings yet
- Anthropometricstudy of Proximal End of Dried Adult Human Femur: A Cross Sectional StudyDocument5 pagesAnthropometricstudy of Proximal End of Dried Adult Human Femur: A Cross Sectional StudyIJAR JOURNALNo ratings yet
- Al-Kayat and BramliDocument13 pagesAl-Kayat and BramliAshish Dadhania100% (1)
- Ijo 26 163Document6 pagesIjo 26 163Javi ChavezNo ratings yet
- Bare Olecranon PDFDocument6 pagesBare Olecranon PDFGhassen BouaouajaNo ratings yet
- Morphometric Analysis of The Foramen Magnum and Jugular Foramen in Adult Skulls in Southern Nigerian PopulationDocument3 pagesMorphometric Analysis of The Foramen Magnum and Jugular Foramen in Adult Skulls in Southern Nigerian Populationjaiswal.ayu2403No ratings yet
- Lig Hyrtl+Porul Crotaphitico-BuccinatorDocument4 pagesLig Hyrtl+Porul Crotaphitico-BuccinatorMatei HerminaNo ratings yet
- Incisive Canal and Its Propinquity To Maxillary Central Incisors in Various Sagittal Growth Patterns: A CBCT StudyDocument11 pagesIncisive Canal and Its Propinquity To Maxillary Central Incisors in Various Sagittal Growth Patterns: A CBCT StudyIJAR JOURNALNo ratings yet
- Biceps y Ligamento Trasnverso HumeralDocument7 pagesBiceps y Ligamento Trasnverso HumeraljesusglezctNo ratings yet
- Morphological Variation in The Structure of The Jugular Foramen in Adult Human Dried Skull in North IndiaDocument3 pagesMorphological Variation in The Structure of The Jugular Foramen in Adult Human Dried Skull in North Indiajaiswal.ayu2403No ratings yet
- Toxina Masseter TopographyDocument5 pagesToxina Masseter TopographyMarioOk KreasNo ratings yet
- Delhiraj EtalDocument4 pagesDelhiraj EtaleditorijmrhsNo ratings yet
- Descriptive Characteristics of The Area of Origin of The Deltoid Musc - 2018 - HDocument5 pagesDescriptive Characteristics of The Area of Origin of The Deltoid Musc - 2018 - HHenrique Paranhos FernandesNo ratings yet
- Taurodontism: An Endodontic Challenge. Report of A Case: Journal of Endodontics June 2003Document4 pagesTaurodontism: An Endodontic Challenge. Report of A Case: Journal of Endodontics June 2003raissa callistaNo ratings yet
- Ymj 49 1004Document4 pagesYmj 49 1004Juan Jos� Beltr�n Hern�ndezNo ratings yet
- Radiographic Measurements of Normal Elbows: Clinical Relevance To Olecranon FracturesDocument4 pagesRadiographic Measurements of Normal Elbows: Clinical Relevance To Olecranon Fracturesjmhinos4833No ratings yet
- Triangular Fiibrocartilage Complex: Anatomico-Clinical CorrelationsDocument7 pagesTriangular Fiibrocartilage Complex: Anatomico-Clinical CorrelationsPaula BautistaNo ratings yet
- Morphological Variations of Jugular Foramen in Dry Skulls of Central Indian Population: A Cross-Sectional StudyDocument4 pagesMorphological Variations of Jugular Foramen in Dry Skulls of Central Indian Population: A Cross-Sectional Studyjaiswal.ayu2403No ratings yet
- CT of The Paranasal Sinuses Normal Anatomyvariants and PathologyDocument10 pagesCT of The Paranasal Sinuses Normal Anatomyvariants and PathologyAndi FirdaNo ratings yet
- Anatomical Causes of Costen's Syndrome: Research ArticleDocument5 pagesAnatomical Causes of Costen's Syndrome: Research Articlefilky .M.nandaNo ratings yet
- Comparison of Overjet Among 3 Arch Types in Normal OcclusionDocument8 pagesComparison of Overjet Among 3 Arch Types in Normal OcclusionAlexandra308No ratings yet
- Iaim 2015 0208 13Document5 pagesIaim 2015 0208 13miskica miskicaNo ratings yet
- Morphometric Study of The Pterion in Dry Human Skulls in Northeast BrazilDocument7 pagesMorphometric Study of The Pterion in Dry Human Skulls in Northeast BrazilDesiré MagalhãesNo ratings yet
- Anthropometric Measurements of Jugular Foramen in Ethiopian Dried Adult SkullsDocument9 pagesAnthropometric Measurements of Jugular Foramen in Ethiopian Dried Adult Skullsjaiswal.ayu2403No ratings yet
- The Anatomy of The Deltoid Insertion by Rispoli, Athwal, Sperling, CofieldDocument5 pagesThe Anatomy of The Deltoid Insertion by Rispoli, Athwal, Sperling, CofieldTensegrity WikiNo ratings yet
- Foramen Huschke PatologicoDocument7 pagesForamen Huschke PatologicoLM AdrianneNo ratings yet
- Clinical Anatomy of The Maxillary Artery: Ippei OTAKE, Ikuo Kageyama and Izumi MATAGADocument10 pagesClinical Anatomy of The Maxillary Artery: Ippei OTAKE, Ikuo Kageyama and Izumi MATAGARajan KarmakarNo ratings yet
- Diaphyseal Nutrient Foramina in Human Femur: Nirmalya Saha, Moirangthem Matum Singh, Ningthoujam Damayanti DeviDocument3 pagesDiaphyseal Nutrient Foramina in Human Femur: Nirmalya Saha, Moirangthem Matum Singh, Ningthoujam Damayanti DeviIOSRjournalNo ratings yet
- Preoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianDocument7 pagesPreoperative Diagnosis of A Third Root Canal in First and Second Maxillary Premolars A Challenge For The ClinicianS S Saad SaadNo ratings yet
- Neuralgia MandibularDocument4 pagesNeuralgia Mandibularkubra_tuncel6296No ratings yet
- An Anatomical Study On Various Types of Suprascapular Notch, Its Relation With Glenoid Cavity and Morphometry of Scapula in South Indian PopulationDocument5 pagesAn Anatomical Study On Various Types of Suprascapular Notch, Its Relation With Glenoid Cavity and Morphometry of Scapula in South Indian PopulationRaviprasanna K HNo ratings yet
- Canovas Et Al 1998 Clinical Anatomy 2Document7 pagesCanovas Et Al 1998 Clinical Anatomy 2ChrissNo ratings yet
- 19 Khanapurkar EtalDocument5 pages19 Khanapurkar EtaleditorijmrhsNo ratings yet
- Surface Ultrastructure of Heterophyes Collected From A ManDocument5 pagesSurface Ultrastructure of Heterophyes Collected From A ManRiandika SusilaNo ratings yet
- 1 s2.0 S1743919106600538 Main PDFDocument3 pages1 s2.0 S1743919106600538 Main PDFTarun MathurNo ratings yet
- Maxillary Width and Hard Palate Thickness in Men and Women With Different Vertical and Sagittal Skeletal PatternsDocument10 pagesMaxillary Width and Hard Palate Thickness in Men and Women With Different Vertical and Sagittal Skeletal PatternsLily CANo ratings yet
- Male Genitalial Morphology of The Carob Moth, Ectomyelois Ceratoniae (Zeller) (Lepidoptera: Pyralidae) With Reference To Their ChemoreceptorDocument7 pagesMale Genitalial Morphology of The Carob Moth, Ectomyelois Ceratoniae (Zeller) (Lepidoptera: Pyralidae) With Reference To Their Chemoreceptorray m deraniaNo ratings yet
- Artigo Bad SplitDocument6 pagesArtigo Bad SplitCarolinaNo ratings yet
- Trochlear Morphology in Healthy People ImplicatioDocument7 pagesTrochlear Morphology in Healthy People ImplicatioNacho TorreroNo ratings yet
- The Temporomandibular Joint: Pneumatic Temporal Cells Open Into The Articular and Extradural SpacesDocument7 pagesThe Temporomandibular Joint: Pneumatic Temporal Cells Open Into The Articular and Extradural SpacesBs PhuocNo ratings yet
- 3 PBDocument8 pages3 PBfabian hernandez medinaNo ratings yet
- Dental Arch WidthsDocument6 pagesDental Arch WidthsShiva PrasadNo ratings yet
- Abstract-The Adverse Effects of Periodontal Disease On Dental Pulp Have Been Debated For ManyDocument11 pagesAbstract-The Adverse Effects of Periodontal Disease On Dental Pulp Have Been Debated For ManySri RahmawatiNo ratings yet
- Is There Any Relation Between Distal Parameters of The Femur and Its Height and Width?Document9 pagesIs There Any Relation Between Distal Parameters of The Femur and Its Height and Width?juanibirisNo ratings yet
- A Morphometric Study of Patella in Lucknow RegionDocument10 pagesA Morphometric Study of Patella in Lucknow RegionIJAR JOURNALNo ratings yet
- Branching of Mandibular Canal On Cone BeamDocument5 pagesBranching of Mandibular Canal On Cone BeamKarina CarlinNo ratings yet
- Thoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeFrom EverandThoracic and Coracoid Arteries In Two Families of Birds, Columbidae and HirundinidaeNo ratings yet
- Throwers Ten Exercise Program PDFDocument5 pagesThrowers Ten Exercise Program PDFAndresLeivaMckendrickNo ratings yet
- Ditaranto 2004Document4 pagesDitaranto 2004karthikeyan eswaranNo ratings yet
- How To Overhead Press With Proper Form - The Definitive Guide - StrongLiftsDocument39 pagesHow To Overhead Press With Proper Form - The Definitive Guide - StrongLiftssjeyarajah21No ratings yet
- The Shoulder GirdleDocument26 pagesThe Shoulder GirdleVeena VishwanathNo ratings yet
- Limbs 1b - Overview of Anatomy of Upper and Lower LimbsDocument5 pagesLimbs 1b - Overview of Anatomy of Upper and Lower LimbsTarmizi Md NorNo ratings yet
- Physical Exam Shoulder EditDocument28 pagesPhysical Exam Shoulder EditNur Syamsiah MNo ratings yet
- Teste UmarDocument30 pagesTeste UmarIoana Temeliescu Ex Zamfir100% (2)
- Piano Hand TechniqueDocument12 pagesPiano Hand TechniquevaneriolamaNo ratings yet
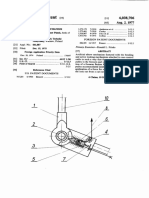
- 1977 - Artificial Elbow Mechanism - Us4038706Document7 pages1977 - Artificial Elbow Mechanism - Us4038706Arturo VaineNo ratings yet
- Radial Nerve PalsyDocument10 pagesRadial Nerve Palsycemm_11No ratings yet
- Curs 3 - EnglDocument94 pagesCurs 3 - EnglSorin BarbuNo ratings yet
- Bednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009Document9 pagesBednar MS, James MA, Light TR. Congenital Longitudinal Deficiency. J Hand Surg Am. 2009AsdfNo ratings yet
- Anat Recall Que - Dr. AzamDocument24 pagesAnat Recall Que - Dr. AzamSurya VummadisettyNo ratings yet
- 2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDocument3 pages2.08 Brachial Region (Arm) - Compartments, Muscles, Nerves, and VesselsDi CanNo ratings yet
- St. Luke's College of Medicine - William H. Quasha Memorial: AnatomyDocument7 pagesSt. Luke's College of Medicine - William H. Quasha Memorial: AnatomyMavic VillanuevaNo ratings yet
- Shoulder and Elbow Scored and Recorded Self-Assessment ExaminationDocument73 pagesShoulder and Elbow Scored and Recorded Self-Assessment ExaminationZia Ur RehmanNo ratings yet
- Assignment No. 6Document12 pagesAssignment No. 6Regina GambayanNo ratings yet
- Medial Vs Lateral Winging of The ScapulaDocument11 pagesMedial Vs Lateral Winging of The ScapulaanjelikaNo ratings yet
- Classification of Full-Thickness Rotator Cuff Lesions - A ReviewDocument11 pagesClassification of Full-Thickness Rotator Cuff Lesions - A ReviewEllan Giulianno FerreiraNo ratings yet
- The Terrible Triad of The ElbowDocument5 pagesThe Terrible Triad of The Elbowapi-250084607No ratings yet
- Av Shunt PPDocument34 pagesAv Shunt PPwahyuartyningsihNo ratings yet
- Jospt.2002.32.10.497 2Document13 pagesJospt.2002.32.10.497 2cderosasNo ratings yet
- Introduction To Regional Biomechanics 2Document12 pagesIntroduction To Regional Biomechanics 2Rokia AlmazNo ratings yet
- Nerve InjuriesDocument3 pagesNerve InjuriesAmber MerrittNo ratings yet
- Workout Sheet-Hybrid p90x P90xplusDocument2 pagesWorkout Sheet-Hybrid p90x P90xplusHaess RomaniNo ratings yet