Download as pdf or txt
You might also like
- Med PPT Pneumonia For LectureDocument67 pagesMed PPT Pneumonia For LectureManisanthosh Kumar100% (1)
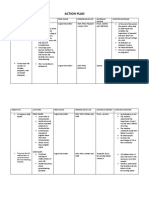
- Action PlanDocument4 pagesAction PlanJosette Mae Atanacio67% (3)
- Nonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovanniDocument14 pagesNonimaging Diagnostic Tests For Pneumonia: Anupama Gupta Brixey,, Raju Reddy,, Shewit P. GiovannikaeranNo ratings yet
- Clinical Practice Guidelines: Immune-Related PneumonitisDocument3 pagesClinical Practice Guidelines: Immune-Related PneumonitisAlin Ionut BurlacuNo ratings yet
- 05 Investigations For PneumoniaDocument4 pages05 Investigations For Pneumoniause4meNo ratings yet
- Pneumonia in Critical Patients - KARTIKADocument29 pagesPneumonia in Critical Patients - KARTIKAKartika JuwitaNo ratings yet
- FullDocument12 pagesFulljuan carlosNo ratings yet
- Selected Oncologic Emergencies: Sandra S. Ugras-ReyDocument13 pagesSelected Oncologic Emergencies: Sandra S. Ugras-ReyJustene PeñamoraNo ratings yet
- Pneumoniae (22%) Was The Most Frequently Isolated Causative Agent, Followed S. Aureus (10%), EnterobacteriaceaeDocument2 pagesPneumoniae (22%) Was The Most Frequently Isolated Causative Agent, Followed S. Aureus (10%), EnterobacteriaceaehawhawnurNo ratings yet
- Review: Atypical Pathogen Infection in Community-Acquired PneumoniaDocument7 pagesReview: Atypical Pathogen Infection in Community-Acquired PneumoniaDebi SusantiNo ratings yet
- 1 s2.0 S1198743X1464194X Main - 2Document8 pages1 s2.0 S1198743X1464194X Main - 2Andy SetiawanNo ratings yet
- Pneumocystis PneumoniaDocument16 pagesPneumocystis PneumoniaMaría Luisa MantillaNo ratings yet
- Jurnal Bahasa InggrisDocument12 pagesJurnal Bahasa InggrisVanessa Angelica SitepuNo ratings yet
- Hospital PneumoniaDocument15 pagesHospital Pneumoniarivai anwarNo ratings yet
- 2007 Diagnostic Strategies in Nosocomial PneumoniaDocument6 pages2007 Diagnostic Strategies in Nosocomial PneumoniaIvana Daniela BelloNo ratings yet
- Section - PCP From Guideline For The Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIVDocument19 pagesSection - PCP From Guideline For The Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIVoralposter PIPKRA2023No ratings yet
- Etiología de La Neumonía Adquirida en La Comunidad en El Adulto InmunocompetenteDocument8 pagesEtiología de La Neumonía Adquirida en La Comunidad en El Adulto InmunocompetenteEileen Torres CerdaNo ratings yet
- Ventilator Associated Pneumonia TreatmentDocument43 pagesVentilator Associated Pneumonia Treatmentmkc71No ratings yet
- Nac 2017Document18 pagesNac 2017Nataly CortesNo ratings yet
- PR JE Mikro Jenjang 1 Frany FinalDocument5 pagesPR JE Mikro Jenjang 1 Frany FinalFrany CharismaNo ratings yet
- Imp bn1Document5 pagesImp bn1Karito FloresNo ratings yet
- 1 s2.0 S2211568412001702 Main PDFDocument10 pages1 s2.0 S2211568412001702 Main PDFGordana PuzovicNo ratings yet
- Nosocomial Pneumonia: Self AssessmentDocument10 pagesNosocomial Pneumonia: Self AssessmentZali AhmadNo ratings yet
- Imaging of Pulmonary Infection: Tomás Franquet and Johnathan H. ChungDocument13 pagesImaging of Pulmonary Infection: Tomás Franquet and Johnathan H. ChungVictor ChiabaiNo ratings yet
- Procalcitonin 2Document6 pagesProcalcitonin 2zivl1984No ratings yet
- JCDR 11 TC06 PDFDocument4 pagesJCDR 11 TC06 PDFPutra PratamaNo ratings yet
- M C - A P: Clinical PracticeDocument7 pagesM C - A P: Clinical PracticeKak DhenyNo ratings yet
- Respiratory and Pulmonary Medicine: ClinmedDocument5 pagesRespiratory and Pulmonary Medicine: ClinmedPutri Zeahan Ramadhini YedismanNo ratings yet
- De Pascale 2012Document9 pagesDe Pascale 2012HellcroZNo ratings yet
- Basic Concepts On Communityacquired Bacterial Pneumonia in PediatricsDocument6 pagesBasic Concepts On Communityacquired Bacterial Pneumonia in PediatricsJesselle LasernaNo ratings yet
- Pneumonia in Immunocompromised Patients: Respirology (2009) 14 (Suppl. 2) S44 - S50Document7 pagesPneumonia in Immunocompromised Patients: Respirology (2009) 14 (Suppl. 2) S44 - S50intankmlsNo ratings yet
- Community Acquired PneumoniaDocument6 pagesCommunity Acquired PneumoniaMaleja Alfaro TangNo ratings yet
- 394 Full PDFDocument20 pages394 Full PDFHaltiNo ratings yet
- 30794136: Aspiration Pneumonia in Older AdultsDocument7 pages30794136: Aspiration Pneumonia in Older AdultsNilson Morales CordobaNo ratings yet
- Diagnostic and Prognostic Role of Procalcitonin in CAPDocument5 pagesDiagnostic and Prognostic Role of Procalcitonin in CAPKarito FloresNo ratings yet
- Cip On CovidDocument40 pagesCip On CovidLorenz L. Llamas IIINo ratings yet
- Biomarcadores en UCIDocument4 pagesBiomarcadores en UCIGrisel MezaNo ratings yet
- PIIS0167814024000689Document11 pagesPIIS0167814024000689Raul Matute MartinNo ratings yet
- DeteksionDocument9 pagesDeteksionkasandraharahapNo ratings yet
- Cap PhilippinesDocument13 pagesCap PhilippinesRaine CentinoNo ratings yet
- Pneumonia Panel GuidelineDocument8 pagesPneumonia Panel Guidelineilham perdiansyahNo ratings yet
- Lung Ultrasonography For The Diagnosis of SARS-CoV-2 Pneumonia in The Emergency DepartmentDocument10 pagesLung Ultrasonography For The Diagnosis of SARS-CoV-2 Pneumonia in The Emergency DepartmentFannyRivera27No ratings yet
- Plasma Cytokine Profile On Admission Related To Aetiology in Community Acquired PneumoniaDocument9 pagesPlasma Cytokine Profile On Admission Related To Aetiology in Community Acquired Pneumoniahusni gunawanNo ratings yet
- Practice Essentials: Essential Update: Telavancin Approved For Bacterial PneumoniaDocument12 pagesPractice Essentials: Essential Update: Telavancin Approved For Bacterial PneumoniaAnnette CraigNo ratings yet
- NeumoniaDocument28 pagesNeumoniaresidentes isssteNo ratings yet
- Jurnal 20Document5 pagesJurnal 20Ahmad Fari Arief LopaNo ratings yet
- Cap AsmaDocument10 pagesCap AsmaAuliaNo ratings yet
- CAP Diagnostic (Uptoptodate 2019)Document34 pagesCAP Diagnostic (Uptoptodate 2019)elizabeth perezzNo ratings yet
- Non-Tuberculous Mycobacterial Pulmonary Infections: ReviewDocument12 pagesNon-Tuberculous Mycobacterial Pulmonary Infections: Reviewmgoez077No ratings yet
- Ventilator Associated Pneumonia (Vap)Document11 pagesVentilator Associated Pneumonia (Vap)Suresh KumarNo ratings yet
- Pneumonia With Pleural EffusionDocument24 pagesPneumonia With Pleural EffusionMund CheleNo ratings yet
- TBR PCPDocument28 pagesTBR PCPAyahnya Rafli100% (1)
- AJRM MARCH PP 5-7Document3 pagesAJRM MARCH PP 5-7Vito Sahala TobiasNo ratings yet
- Pi Is 2058534917300689Document5 pagesPi Is 2058534917300689Tina woldegebrielNo ratings yet
- Neumonía en iMS Review PDFDocument14 pagesNeumonía en iMS Review PDFSofia SimpertigueNo ratings yet
- Lower Respiratory Tract InfectionDocument21 pagesLower Respiratory Tract InfectionJohn Vincent Dy OcampoNo ratings yet
- 2021 - TorresDocument28 pages2021 - TorresCarlosNo ratings yet
- Optimizingdiagnosisand Managementofcommunity-Acquiredpneumoniainthe EmergencydepartmentDocument17 pagesOptimizingdiagnosisand Managementofcommunity-Acquiredpneumoniainthe Emergencydepartmentهادي تركي شنبارةNo ratings yet
- Glchunk 321Document19 pagesGlchunk 321Hai SheikhNo ratings yet
- International Kawasaki Disease Symposium ProgramDocument208 pagesInternational Kawasaki Disease Symposium ProgramNikka Moreen DagdagNo ratings yet
- 01 - 08 - Chapter 8 INFANT - CHILD MORTALITY-NDHS - BAY - Chap8 - July28 Rev-Formatted08042014 - Revaug14 PDFDocument10 pages01 - 08 - Chapter 8 INFANT - CHILD MORTALITY-NDHS - BAY - Chap8 - July28 Rev-Formatted08042014 - Revaug14 PDFIrwin FajaritoNo ratings yet
- Generic Substitution Binu ThapaDocument13 pagesGeneric Substitution Binu ThapabimuNo ratings yet
- Future Trends in Nursing Research-PresentationDocument49 pagesFuture Trends in Nursing Research-PresentationSr theresejoseNo ratings yet
- Mental Health Nursing 6Th Edition Fontaine Test Bank Full Chapter PDFDocument17 pagesMental Health Nursing 6Th Edition Fontaine Test Bank Full Chapter PDFkhuyentryphenakj1100% (13)
- 9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEDocument12 pages9 Safe Nursing Indicators - Safe Staffing For Nursing in Adult Inpatient Wards in Acute Hospitals - Guidance - NICEmiftakhul jannahNo ratings yet
- Creativity - Wellbeing - and - Mental - Health - Practice Творчество, благополучие и практика психического здоровьяDocument167 pagesCreativity - Wellbeing - and - Mental - Health - Practice Творчество, благополучие и практика психического здоровьяVasily Zabelin100% (1)
- Senior Living (March 1, 2024)Document8 pagesSenior Living (March 1, 2024)The Livingston County NewsNo ratings yet
- Risk For Constipation Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Independent: Goal MetDocument10 pagesRisk For Constipation Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Independent: Goal MetHydie Mae AlcabedosNo ratings yet
- Pharmacokinetics Pharmacodynamics of Controlled Release SystemsDocument33 pagesPharmacokinetics Pharmacodynamics of Controlled Release SystemsSumant SainiNo ratings yet
- Training Philiipine Paramedical & Technical School of Davao Nurse DirectoryDocument4 pagesTraining Philiipine Paramedical & Technical School of Davao Nurse Directorydgina8800No ratings yet
- B2.4 Student WorksheetDocument5 pagesB2.4 Student WorksheetAbdullaahNo ratings yet
- College of Our Lady of Mt. Carmel (Pampanga) : Course SyllabusDocument4 pagesCollege of Our Lady of Mt. Carmel (Pampanga) : Course Syllabus;'SiLeNt';No ratings yet
- Uttarakhand Ayush POLICY 2018Document31 pagesUttarakhand Ayush POLICY 2018Vishy BhatiaNo ratings yet
- The Connection of Evidence-Based Practice and The Quadruple AimDocument7 pagesThe Connection of Evidence-Based Practice and The Quadruple AimMichael KairithiaNo ratings yet
- RRL KoDocument1 pageRRL KoAira FrancescaNo ratings yet
- Ic 38 Non Life SyllabusDocument4 pagesIc 38 Non Life SyllabusSKNo ratings yet
- Jaymie-Lyn Labelle: Highlight of QualificationsDocument2 pagesJaymie-Lyn Labelle: Highlight of QualificationsHassan Mohamed FarajNo ratings yet
- Pangkalan Data Pendidikan Tinggi: Login SistemDocument4 pagesPangkalan Data Pendidikan Tinggi: Login Sistemanindini winda amaliaNo ratings yet
- Faith HealingDocument23 pagesFaith Healingcreamyfrappe0% (1)
- CDC Malaria ProgramDocument2 pagesCDC Malaria ProgramabthakurNo ratings yet
- CMS1500 ANSI837v5010 CrosswalkDocument5 pagesCMS1500 ANSI837v5010 CrosswalkMuhammad MubasherNo ratings yet
- Gundayao, Sheryl SDocument4 pagesGundayao, Sheryl SFitz Jerome JagonaseNo ratings yet
- IPT Students - Non-Hospital Based Specialists KUANTANDocument113 pagesIPT Students - Non-Hospital Based Specialists KUANTANFatin nadhirah Kamaludin latifiNo ratings yet
- Jurnal Paliatif 1Document10 pagesJurnal Paliatif 1Anisa SilviaNo ratings yet
- Aop 2023Document26 pagesAop 2023ilog ndp100% (3)
- Classification of Facilities (Doh Ao-0012a)Document42 pagesClassification of Facilities (Doh Ao-0012a)Marissa AsimNo ratings yet
- Reference ThesisDocument13 pagesReference ThesisGhina SalsabilaNo ratings yet
- Proceedings of The National Workshop On INTRODUCING YOGA IN MEDICAL CURRICULUMDocument76 pagesProceedings of The National Workshop On INTRODUCING YOGA IN MEDICAL CURRICULUMYogacharya Dr Ananda Balayogi Bhavanani0% (1)