
Hoffas Disease
Hoffas Disease
You might also like
- Strasinger, Susan King, Di Lorenzo, Marjorie Schaub - Urinalysis and Body Fluids 7th EdDocument426 pagesStrasinger, Susan King, Di Lorenzo, Marjorie Schaub - Urinalysis and Body Fluids 7th EdJocelle90% (10)
- Fintec 1107 Manual PDFDocument126 pagesFintec 1107 Manual PDFLogan100% (2)
- A Textbook of Sports and Exercise PhysiologyDocument347 pagesA Textbook of Sports and Exercise PhysiologyPraneeth KumarNo ratings yet
- 22 Medical School Interview: Questions & AnswersDocument10 pages22 Medical School Interview: Questions & AnswershoangptkNo ratings yet
- Epicondylitis, Lateral: (Tennis Elbow)Document6 pagesEpicondylitis, Lateral: (Tennis Elbow)ArieZta Kautsar RahmanNo ratings yet
- Piriformis SyndromeDocument3 pagesPiriformis SyndromeherikNo ratings yet
- SPONDYLOLYSTHESISDocument5 pagesSPONDYLOLYSTHESISMuhammad AbdullahNo ratings yet
- Fisioterapia en Prótesis de CaderaDocument24 pagesFisioterapia en Prótesis de CaderaGiusePpe MeatzaNo ratings yet
- IVDP: Inter Vertebral Disc ProlapseDocument34 pagesIVDP: Inter Vertebral Disc ProlapseShibinNo ratings yet
- Osgood Schlatter Disease With Exercises ChocDocument4 pagesOsgood Schlatter Disease With Exercises ChocJoni MokodoNo ratings yet
- Herniated DiscsDocument28 pagesHerniated DiscsEndah A. Rahmadhani SugiartoNo ratings yet
- Physiotherapy InformationDocument16 pagesPhysiotherapy InformationAlejandro SanchezNo ratings yet
- Tennis ElbowDocument11 pagesTennis ElbowMikael AdityaNo ratings yet
- ReportDocument19 pagesReportAlexandra RaciniNo ratings yet
- IT Band Handout Knee Jan 2021dDocument20 pagesIT Band Handout Knee Jan 2021dakfajarNo ratings yet
- PtendinopathyDocument16 pagesPtendinopathysmaouimohammedNo ratings yet
- EP0273 Plantar FasciitisDocument2 pagesEP0273 Plantar FasciitisFalayna Ithu DheisyaNo ratings yet
- An Introduction To The Mckenzie Method: Treating Your Own BackDocument24 pagesAn Introduction To The Mckenzie Method: Treating Your Own BackR HariNo ratings yet
- Spondylolysis SpondylolisthesisDocument89 pagesSpondylolysis SpondylolisthesisAh ZhangNo ratings yet
- Rehabilitation Post SurgeryDocument28 pagesRehabilitation Post SurgeryFederica PiccaroloNo ratings yet
- Achilles Tendinopathy: Advice and Management: Department of Physiotherapy Department of Sport and Exercise MedicineDocument16 pagesAchilles Tendinopathy: Advice and Management: Department of Physiotherapy Department of Sport and Exercise MedicinebiilNo ratings yet
- Trochanteric Bursitis Exercises Dec 5Document18 pagesTrochanteric Bursitis Exercises Dec 5CoupleFF BRNo ratings yet
- Advice Following Hip Fracture 2Document20 pagesAdvice Following Hip Fracture 2Nithu shanNo ratings yet
- Iliotibial BandsyndromeDocument24 pagesIliotibial BandsyndromeNada TahaNo ratings yet
- نسخة Back Pain TutorialDocument65 pagesنسخة Back Pain Tutorialabdulslamshukri1No ratings yet
- 2017 Hip RehabilitationDocument6 pages2017 Hip RehabilitationAdrianNo ratings yet
- Pathfit2 Midterm Safety TipsDocument58 pagesPathfit2 Midterm Safety TipsNICKO PACLEBNo ratings yet
- Ankle Sprain ED LeafletDocument2 pagesAnkle Sprain ED LeafletDeborayuni AstutiNo ratings yet
- Frozen ShoulderDocument18 pagesFrozen ShoulderChitra ChauhanNo ratings yet
- Helping Your Knee To Recover After A Ligament Sprain or RuptureDocument4 pagesHelping Your Knee To Recover After A Ligament Sprain or RuptureDiegoNo ratings yet
- Flyer Sosm Spondylolysis - Listhesis Rehab Guidelines 8 - 5x11Document3 pagesFlyer Sosm Spondylolysis - Listhesis Rehab Guidelines 8 - 5x11Muhammad AbdullahNo ratings yet
- Otago Level A - EnglishDocument10 pagesOtago Level A - EnglishHuyền NguyễnNo ratings yet
- Low Back and SacrumDocument27 pagesLow Back and SacrumdwNo ratings yet
- Groin-Strain Leaflet PDFDocument2 pagesGroin-Strain Leaflet PDFflorintrmNo ratings yet
- McKenzie LumbarDocument51 pagesMcKenzie LumbarRouqia HamedNo ratings yet
- HIP Bursitis ExercisesDocument6 pagesHIP Bursitis ExercisesAyesha ShafiqNo ratings yet
- Rehab Hip 3 PDFDocument6 pagesRehab Hip 3 PDFlapokNo ratings yet
- Overuse Knee InjuriesDocument4 pagesOveruse Knee InjuriesThe HomieNo ratings yet
- Varicose Vein Exercise and CareDocument8 pagesVaricose Vein Exercise and CareAtu KaushalNo ratings yet
- 2023-Rehab HipDocument6 pages2023-Rehab HipJade venterNo ratings yet
- Importance of First AidDocument20 pagesImportance of First AidHeroe SedicoNo ratings yet
- Off-Campus Placement ProjectDocument4 pagesOff-Campus Placement Projectapi-488042467No ratings yet
- Lumbar Herniated Disc Physical Therapy PrescriptionDocument4 pagesLumbar Herniated Disc Physical Therapy PrescriptionDiah PramuditaNo ratings yet
- Low Back Pain: Information For PatientsDocument0 pagesLow Back Pain: Information For PatientsRavisankar PeriasamyNo ratings yet
- 7 Patellofemoral SyndromeDocument2 pages7 Patellofemoral Syndromezilojian80No ratings yet
- Stabilization Side Plank Track Lumbar SIDocument1 pageStabilization Side Plank Track Lumbar SIasmaNo ratings yet
- Hip Exercises 1 1Document2 pagesHip Exercises 1 1Frozen Pandora MahayaNo ratings yet
- PT Guidelines For Ankle SprainDocument5 pagesPT Guidelines For Ankle SprainKirti GunjikarNo ratings yet
- Common Injuries in Sports and DeformitiesDocument28 pagesCommon Injuries in Sports and DeformitiesCherilyn SaagundoNo ratings yet
- Mckenzie Vs William Flexion ExerciseDocument38 pagesMckenzie Vs William Flexion ExerciseIftinan Amalia100% (1)
- Advice and Exercises For Patients With Plantar Fasciitis - Jul21Document7 pagesAdvice and Exercises For Patients With Plantar Fasciitis - Jul21timothy limNo ratings yet
- Spine Conditioning ProgramDocument7 pagesSpine Conditioning Programmaimunabegam766No ratings yet
- Ortho: Hip Conditioning ProgramDocument6 pagesOrtho: Hip Conditioning ProgramDrYoyoNo ratings yet
- 2017-Rehab Spine PDFDocument7 pages2017-Rehab Spine PDFPerpetua KamikadzeNo ratings yet
- PL 993.1 Patellar Knee Cap Tendon RupturesDocument8 pagesPL 993.1 Patellar Knee Cap Tendon RupturesYova TmbxNo ratings yet
- Calcaneal SpursDocument10 pagesCalcaneal Spurskrishnamoorthy abiramanNo ratings yet
- TendinitisDocument7 pagesTendinitisIceLeg SamUelNo ratings yet
- Reporter 5 Cool Down PeDocument45 pagesReporter 5 Cool Down PepasonmykieNo ratings yet
- Esguince TerminadoDocument30 pagesEsguince Terminadostephany cebeNo ratings yet
- P AnkleDocument8 pagesP AnkleJessica Hammer HarrellNo ratings yet
- Ankle Sprains PDFDocument2 pagesAnkle Sprains PDFAtishNo ratings yet
- Tight Hip Flexors: Comprehensive Guide on How to Efficiently Relieve All Kinds of Pain Associated with Tight Hip Flexors in less Than 5 minutes; Tight Hip Flexor Home/Gym Remedies (Beginner's Guide)From EverandTight Hip Flexors: Comprehensive Guide on How to Efficiently Relieve All Kinds of Pain Associated with Tight Hip Flexors in less Than 5 minutes; Tight Hip Flexor Home/Gym Remedies (Beginner's Guide)No ratings yet
- Tabata Fatblaster System: Complete Training and Nutrition Guide to Insane Fat LossFrom EverandTabata Fatblaster System: Complete Training and Nutrition Guide to Insane Fat LossNo ratings yet
- 6276b044fbcd27867651a7b86a8fa446Document46 pages6276b044fbcd27867651a7b86a8fa446Praneeth KumarNo ratings yet
- Motor Neuron DiseasesDocument24 pagesMotor Neuron DiseasesPraneeth Kumar100% (1)
- Ethics Integrity and Wrong DoingDocument15 pagesEthics Integrity and Wrong DoingPraneeth Kumar100% (1)
- Eccentric Hamstring ExercisesDocument4 pagesEccentric Hamstring ExercisesPraneeth KumarNo ratings yet
- Date: 02/03/2023: Sale PriceDocument2 pagesDate: 02/03/2023: Sale PricePraneeth KumarNo ratings yet
- Cerebrospinal Fluid Its StructureDocument1 pageCerebrospinal Fluid Its StructurePraneeth KumarNo ratings yet
- Mobilization 2 - Saloni ShettyDocument18 pagesMobilization 2 - Saloni ShettyPraneeth KumarNo ratings yet
- Sports in MRDocument7 pagesSports in MRPraneeth KumarNo ratings yet
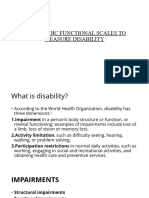
- Orthopedic Functional Scales To Measure DisabilityDocument9 pagesOrthopedic Functional Scales To Measure DisabilityPraneeth KumarNo ratings yet
- De Quervains 72776304Document31 pagesDe Quervains 72776304Praneeth KumarNo ratings yet
- TOS Rehab CompleteDocument5 pagesTOS Rehab CompletePraneeth KumarNo ratings yet
- Arthrofibrosis Ebook PDF To Word UPDATED 7-31-23Document68 pagesArthrofibrosis Ebook PDF To Word UPDATED 7-31-23Praneeth KumarNo ratings yet
- Cubital Tunnel SyndromeDocument18 pagesCubital Tunnel SyndromePraneeth KumarNo ratings yet
- 07.03.09 Chest PhysiotherapyDocument9 pages07.03.09 Chest PhysiotherapyPraneeth KumarNo ratings yet
- 13d8b9732fd2fd2aafaf1787463bd635Document11 pages13d8b9732fd2fd2aafaf1787463bd635Praneeth KumarNo ratings yet
- IvdpDocument42 pagesIvdpPraneeth KumarNo ratings yet
- OrthopedicSpecialTests LOWER-Extremity StandAloneCourseDocument51 pagesOrthopedicSpecialTests LOWER-Extremity StandAloneCoursePraneeth KumarNo ratings yet
- LL Orthoses MechanicsDocument22 pagesLL Orthoses MechanicsPraneeth KumarNo ratings yet
- NascimentoLR FunctionalDisabilityScalesDocument5 pagesNascimentoLR FunctionalDisabilityScalesPraneeth KumarNo ratings yet
- 57633e6496d8842b660f866fb36596d8Document51 pages57633e6496d8842b660f866fb36596d8Praneeth KumarNo ratings yet
- Functional Disability ScalesDocument6 pagesFunctional Disability ScalesPraneeth KumarNo ratings yet
- Ankle FootDocument5 pagesAnkle FootPraneeth KumarNo ratings yet
- GDBDocument63 pagesGDBPraneeth KumarNo ratings yet
- Renal FailureDocument25 pagesRenal FailurePraneeth KumarNo ratings yet
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingDocument16 pagesSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingMarcoNo ratings yet
- Rama Daryl Marie C. Module 4 Bustat Elestat Act. 4Document2 pagesRama Daryl Marie C. Module 4 Bustat Elestat Act. 4RACHEL NAVARRONo ratings yet
- Bibliografie: 14. Basmajian J.V. Et Al - A New Bipolar Electrode For EMG, J. of AppliedDocument15 pagesBibliografie: 14. Basmajian J.V. Et Al - A New Bipolar Electrode For EMG, J. of AppliedciuriuseaNo ratings yet
- Drug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofDocument4 pagesDrug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofKamal PatidarNo ratings yet
- TFN Chapter 2Document97 pagesTFN Chapter 2mx odd100% (1)
- Examination of The Motor System: Approach To Weakness: Key Teaching PointsDocument20 pagesExamination of The Motor System: Approach To Weakness: Key Teaching PointsMiravay ChavezNo ratings yet
- SWMS FOR INSTALLATION OF 5x500 KVA GENERATORS AND TOTALIZING PANEL 25.01.23Document8 pagesSWMS FOR INSTALLATION OF 5x500 KVA GENERATORS AND TOTALIZING PANEL 25.01.23Md Shahbaz AlamNo ratings yet
- SEOT JSA For Energizing Site DBDocument3 pagesSEOT JSA For Energizing Site DBArchana SoorajNo ratings yet
- Lab 3 Mid Term ExamDocument3 pagesLab 3 Mid Term ExamAudrey AndinoNo ratings yet
- OPT EP Kimber Student Insurance BrochureDocument20 pagesOPT EP Kimber Student Insurance BrochureKanakamedala Sai Rithvik ee18b051No ratings yet
- The Oxford Handbook of Hoarding (1856)Document433 pagesThe Oxford Handbook of Hoarding (1856)rosysenadoNo ratings yet
- Geriatric LecturesDocument36 pagesGeriatric LecturesJohn DoeNo ratings yet
- BÀI TẬP CỦNG CỐ TUẦN 1Document12 pagesBÀI TẬP CỦNG CỐ TUẦN 1Nguyệt ÁnhNo ratings yet
- An Islamic CBT Approach For Helping Clients With Gender Identity and Sexual Orientation ProblemsDocument26 pagesAn Islamic CBT Approach For Helping Clients With Gender Identity and Sexual Orientation ProblemsNadiyah EliasNo ratings yet
- SDL 2 Wound and Wound HealingDocument4 pagesSDL 2 Wound and Wound HealingDn Ezrinah Dn EshamNo ratings yet
- Case 4Document14 pagesCase 4bekbekk cabahugNo ratings yet
- To Study The Efficacy of Nirgundipatra Swaras Taila Karnapurana in The Management of Pootikarna With Special Reference To Chronic Suppurative Otitis MediaDocument6 pagesTo Study The Efficacy of Nirgundipatra Swaras Taila Karnapurana in The Management of Pootikarna With Special Reference To Chronic Suppurative Otitis MediaEditor IJTSRDNo ratings yet
- Advance Copy 2022 NEGRIHP Final ManuscriptDocument440 pagesAdvance Copy 2022 NEGRIHP Final ManuscriptSchool NursingNo ratings yet
- Intimate Partner Violence Among Pregnant Women inDocument6 pagesIntimate Partner Violence Among Pregnant Women inNove Claire Labawan EnteNo ratings yet
- Metabolism Clinical and ExperimentalDocument4 pagesMetabolism Clinical and ExperimentalusingwebNo ratings yet
- The Boston Globe 30 10 2020 PDFDocument40 pagesThe Boston Globe 30 10 2020 PDFDeadnightvikernesNo ratings yet
- Dignity in Death and Dying: Joyce D. Cajigal, RNDocument14 pagesDignity in Death and Dying: Joyce D. Cajigal, RNWendell Gian GolezNo ratings yet
- Song Review I Lived by OnerepublicDocument2 pagesSong Review I Lived by OnerepublicNur AdilaNo ratings yet
- CKD PDFDocument15 pagesCKD PDFJendrale SudirmanNo ratings yet
- Going All-In For Well-BeingDocument6 pagesGoing All-In For Well-BeingarielNo ratings yet
- The Independent Review of Childrens Social Care Final ReportDocument278 pagesThe Independent Review of Childrens Social Care Final ReportNeil ShellardNo ratings yet
- COPARDocument21 pagesCOPAREdra VillanuevaNo ratings yet
















































































































Download as pdf or txt
You might also like
- Strasinger, Susan King, Di Lorenzo, Marjorie Schaub - Urinalysis and Body Fluids 7th EdDocument426 pagesStrasinger, Susan King, Di Lorenzo, Marjorie Schaub - Urinalysis and Body Fluids 7th EdJocelle90% (10)
- Fintec 1107 Manual PDFDocument126 pagesFintec 1107 Manual PDFLogan100% (2)
- A Textbook of Sports and Exercise PhysiologyDocument347 pagesA Textbook of Sports and Exercise PhysiologyPraneeth KumarNo ratings yet
- 22 Medical School Interview: Questions & AnswersDocument10 pages22 Medical School Interview: Questions & AnswershoangptkNo ratings yet
- Epicondylitis, Lateral: (Tennis Elbow)Document6 pagesEpicondylitis, Lateral: (Tennis Elbow)ArieZta Kautsar RahmanNo ratings yet
- Piriformis SyndromeDocument3 pagesPiriformis SyndromeherikNo ratings yet
- SPONDYLOLYSTHESISDocument5 pagesSPONDYLOLYSTHESISMuhammad AbdullahNo ratings yet
- Fisioterapia en Prótesis de CaderaDocument24 pagesFisioterapia en Prótesis de CaderaGiusePpe MeatzaNo ratings yet
- IVDP: Inter Vertebral Disc ProlapseDocument34 pagesIVDP: Inter Vertebral Disc ProlapseShibinNo ratings yet
- Osgood Schlatter Disease With Exercises ChocDocument4 pagesOsgood Schlatter Disease With Exercises ChocJoni MokodoNo ratings yet
- Herniated DiscsDocument28 pagesHerniated DiscsEndah A. Rahmadhani SugiartoNo ratings yet
- Physiotherapy InformationDocument16 pagesPhysiotherapy InformationAlejandro SanchezNo ratings yet
- Tennis ElbowDocument11 pagesTennis ElbowMikael AdityaNo ratings yet
- ReportDocument19 pagesReportAlexandra RaciniNo ratings yet
- IT Band Handout Knee Jan 2021dDocument20 pagesIT Band Handout Knee Jan 2021dakfajarNo ratings yet
- PtendinopathyDocument16 pagesPtendinopathysmaouimohammedNo ratings yet
- EP0273 Plantar FasciitisDocument2 pagesEP0273 Plantar FasciitisFalayna Ithu DheisyaNo ratings yet
- An Introduction To The Mckenzie Method: Treating Your Own BackDocument24 pagesAn Introduction To The Mckenzie Method: Treating Your Own BackR HariNo ratings yet
- Spondylolysis SpondylolisthesisDocument89 pagesSpondylolysis SpondylolisthesisAh ZhangNo ratings yet
- Rehabilitation Post SurgeryDocument28 pagesRehabilitation Post SurgeryFederica PiccaroloNo ratings yet
- Achilles Tendinopathy: Advice and Management: Department of Physiotherapy Department of Sport and Exercise MedicineDocument16 pagesAchilles Tendinopathy: Advice and Management: Department of Physiotherapy Department of Sport and Exercise MedicinebiilNo ratings yet
- Trochanteric Bursitis Exercises Dec 5Document18 pagesTrochanteric Bursitis Exercises Dec 5CoupleFF BRNo ratings yet
- Advice Following Hip Fracture 2Document20 pagesAdvice Following Hip Fracture 2Nithu shanNo ratings yet
- Iliotibial BandsyndromeDocument24 pagesIliotibial BandsyndromeNada TahaNo ratings yet
- نسخة Back Pain TutorialDocument65 pagesنسخة Back Pain Tutorialabdulslamshukri1No ratings yet
- 2017 Hip RehabilitationDocument6 pages2017 Hip RehabilitationAdrianNo ratings yet
- Pathfit2 Midterm Safety TipsDocument58 pagesPathfit2 Midterm Safety TipsNICKO PACLEBNo ratings yet
- Ankle Sprain ED LeafletDocument2 pagesAnkle Sprain ED LeafletDeborayuni AstutiNo ratings yet
- Frozen ShoulderDocument18 pagesFrozen ShoulderChitra ChauhanNo ratings yet
- Helping Your Knee To Recover After A Ligament Sprain or RuptureDocument4 pagesHelping Your Knee To Recover After A Ligament Sprain or RuptureDiegoNo ratings yet
- Flyer Sosm Spondylolysis - Listhesis Rehab Guidelines 8 - 5x11Document3 pagesFlyer Sosm Spondylolysis - Listhesis Rehab Guidelines 8 - 5x11Muhammad AbdullahNo ratings yet
- Otago Level A - EnglishDocument10 pagesOtago Level A - EnglishHuyền NguyễnNo ratings yet
- Low Back and SacrumDocument27 pagesLow Back and SacrumdwNo ratings yet
- Groin-Strain Leaflet PDFDocument2 pagesGroin-Strain Leaflet PDFflorintrmNo ratings yet
- McKenzie LumbarDocument51 pagesMcKenzie LumbarRouqia HamedNo ratings yet
- HIP Bursitis ExercisesDocument6 pagesHIP Bursitis ExercisesAyesha ShafiqNo ratings yet
- Rehab Hip 3 PDFDocument6 pagesRehab Hip 3 PDFlapokNo ratings yet
- Overuse Knee InjuriesDocument4 pagesOveruse Knee InjuriesThe HomieNo ratings yet
- Varicose Vein Exercise and CareDocument8 pagesVaricose Vein Exercise and CareAtu KaushalNo ratings yet
- 2023-Rehab HipDocument6 pages2023-Rehab HipJade venterNo ratings yet
- Importance of First AidDocument20 pagesImportance of First AidHeroe SedicoNo ratings yet
- Off-Campus Placement ProjectDocument4 pagesOff-Campus Placement Projectapi-488042467No ratings yet
- Lumbar Herniated Disc Physical Therapy PrescriptionDocument4 pagesLumbar Herniated Disc Physical Therapy PrescriptionDiah PramuditaNo ratings yet
- Low Back Pain: Information For PatientsDocument0 pagesLow Back Pain: Information For PatientsRavisankar PeriasamyNo ratings yet
- 7 Patellofemoral SyndromeDocument2 pages7 Patellofemoral Syndromezilojian80No ratings yet
- Stabilization Side Plank Track Lumbar SIDocument1 pageStabilization Side Plank Track Lumbar SIasmaNo ratings yet
- Hip Exercises 1 1Document2 pagesHip Exercises 1 1Frozen Pandora MahayaNo ratings yet
- PT Guidelines For Ankle SprainDocument5 pagesPT Guidelines For Ankle SprainKirti GunjikarNo ratings yet
- Common Injuries in Sports and DeformitiesDocument28 pagesCommon Injuries in Sports and DeformitiesCherilyn SaagundoNo ratings yet
- Mckenzie Vs William Flexion ExerciseDocument38 pagesMckenzie Vs William Flexion ExerciseIftinan Amalia100% (1)
- Advice and Exercises For Patients With Plantar Fasciitis - Jul21Document7 pagesAdvice and Exercises For Patients With Plantar Fasciitis - Jul21timothy limNo ratings yet
- Spine Conditioning ProgramDocument7 pagesSpine Conditioning Programmaimunabegam766No ratings yet
- Ortho: Hip Conditioning ProgramDocument6 pagesOrtho: Hip Conditioning ProgramDrYoyoNo ratings yet
- 2017-Rehab Spine PDFDocument7 pages2017-Rehab Spine PDFPerpetua KamikadzeNo ratings yet
- PL 993.1 Patellar Knee Cap Tendon RupturesDocument8 pagesPL 993.1 Patellar Knee Cap Tendon RupturesYova TmbxNo ratings yet
- Calcaneal SpursDocument10 pagesCalcaneal Spurskrishnamoorthy abiramanNo ratings yet
- TendinitisDocument7 pagesTendinitisIceLeg SamUelNo ratings yet
- Reporter 5 Cool Down PeDocument45 pagesReporter 5 Cool Down PepasonmykieNo ratings yet
- Esguince TerminadoDocument30 pagesEsguince Terminadostephany cebeNo ratings yet
- P AnkleDocument8 pagesP AnkleJessica Hammer HarrellNo ratings yet
- Ankle Sprains PDFDocument2 pagesAnkle Sprains PDFAtishNo ratings yet
- Tight Hip Flexors: Comprehensive Guide on How to Efficiently Relieve All Kinds of Pain Associated with Tight Hip Flexors in less Than 5 minutes; Tight Hip Flexor Home/Gym Remedies (Beginner's Guide)From EverandTight Hip Flexors: Comprehensive Guide on How to Efficiently Relieve All Kinds of Pain Associated with Tight Hip Flexors in less Than 5 minutes; Tight Hip Flexor Home/Gym Remedies (Beginner's Guide)No ratings yet
- Tabata Fatblaster System: Complete Training and Nutrition Guide to Insane Fat LossFrom EverandTabata Fatblaster System: Complete Training and Nutrition Guide to Insane Fat LossNo ratings yet
- 6276b044fbcd27867651a7b86a8fa446Document46 pages6276b044fbcd27867651a7b86a8fa446Praneeth KumarNo ratings yet
- Motor Neuron DiseasesDocument24 pagesMotor Neuron DiseasesPraneeth Kumar100% (1)
- Ethics Integrity and Wrong DoingDocument15 pagesEthics Integrity and Wrong DoingPraneeth Kumar100% (1)
- Eccentric Hamstring ExercisesDocument4 pagesEccentric Hamstring ExercisesPraneeth KumarNo ratings yet
- Date: 02/03/2023: Sale PriceDocument2 pagesDate: 02/03/2023: Sale PricePraneeth KumarNo ratings yet
- Cerebrospinal Fluid Its StructureDocument1 pageCerebrospinal Fluid Its StructurePraneeth KumarNo ratings yet
- Mobilization 2 - Saloni ShettyDocument18 pagesMobilization 2 - Saloni ShettyPraneeth KumarNo ratings yet
- Sports in MRDocument7 pagesSports in MRPraneeth KumarNo ratings yet
- Orthopedic Functional Scales To Measure DisabilityDocument9 pagesOrthopedic Functional Scales To Measure DisabilityPraneeth KumarNo ratings yet
- De Quervains 72776304Document31 pagesDe Quervains 72776304Praneeth KumarNo ratings yet
- TOS Rehab CompleteDocument5 pagesTOS Rehab CompletePraneeth KumarNo ratings yet
- Arthrofibrosis Ebook PDF To Word UPDATED 7-31-23Document68 pagesArthrofibrosis Ebook PDF To Word UPDATED 7-31-23Praneeth KumarNo ratings yet
- Cubital Tunnel SyndromeDocument18 pagesCubital Tunnel SyndromePraneeth KumarNo ratings yet
- 07.03.09 Chest PhysiotherapyDocument9 pages07.03.09 Chest PhysiotherapyPraneeth KumarNo ratings yet
- 13d8b9732fd2fd2aafaf1787463bd635Document11 pages13d8b9732fd2fd2aafaf1787463bd635Praneeth KumarNo ratings yet
- IvdpDocument42 pagesIvdpPraneeth KumarNo ratings yet
- OrthopedicSpecialTests LOWER-Extremity StandAloneCourseDocument51 pagesOrthopedicSpecialTests LOWER-Extremity StandAloneCoursePraneeth KumarNo ratings yet
- LL Orthoses MechanicsDocument22 pagesLL Orthoses MechanicsPraneeth KumarNo ratings yet
- NascimentoLR FunctionalDisabilityScalesDocument5 pagesNascimentoLR FunctionalDisabilityScalesPraneeth KumarNo ratings yet
- 57633e6496d8842b660f866fb36596d8Document51 pages57633e6496d8842b660f866fb36596d8Praneeth KumarNo ratings yet
- Functional Disability ScalesDocument6 pagesFunctional Disability ScalesPraneeth KumarNo ratings yet
- Ankle FootDocument5 pagesAnkle FootPraneeth KumarNo ratings yet
- GDBDocument63 pagesGDBPraneeth KumarNo ratings yet
- Renal FailureDocument25 pagesRenal FailurePraneeth KumarNo ratings yet
- Safety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingDocument16 pagesSafety Data Sheet: SECTION 1: Identification of The Substance/mixture and of The Company/undertakingMarcoNo ratings yet
- Rama Daryl Marie C. Module 4 Bustat Elestat Act. 4Document2 pagesRama Daryl Marie C. Module 4 Bustat Elestat Act. 4RACHEL NAVARRONo ratings yet
- Bibliografie: 14. Basmajian J.V. Et Al - A New Bipolar Electrode For EMG, J. of AppliedDocument15 pagesBibliografie: 14. Basmajian J.V. Et Al - A New Bipolar Electrode For EMG, J. of AppliedciuriuseaNo ratings yet
- Drug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofDocument4 pagesDrug Proving Is The Systematic Process of Acquiring Knowledge of The Instruments Intended For The Cure ofKamal PatidarNo ratings yet
- TFN Chapter 2Document97 pagesTFN Chapter 2mx odd100% (1)
- Examination of The Motor System: Approach To Weakness: Key Teaching PointsDocument20 pagesExamination of The Motor System: Approach To Weakness: Key Teaching PointsMiravay ChavezNo ratings yet
- SWMS FOR INSTALLATION OF 5x500 KVA GENERATORS AND TOTALIZING PANEL 25.01.23Document8 pagesSWMS FOR INSTALLATION OF 5x500 KVA GENERATORS AND TOTALIZING PANEL 25.01.23Md Shahbaz AlamNo ratings yet
- SEOT JSA For Energizing Site DBDocument3 pagesSEOT JSA For Energizing Site DBArchana SoorajNo ratings yet
- Lab 3 Mid Term ExamDocument3 pagesLab 3 Mid Term ExamAudrey AndinoNo ratings yet
- OPT EP Kimber Student Insurance BrochureDocument20 pagesOPT EP Kimber Student Insurance BrochureKanakamedala Sai Rithvik ee18b051No ratings yet
- The Oxford Handbook of Hoarding (1856)Document433 pagesThe Oxford Handbook of Hoarding (1856)rosysenadoNo ratings yet
- Geriatric LecturesDocument36 pagesGeriatric LecturesJohn DoeNo ratings yet
- BÀI TẬP CỦNG CỐ TUẦN 1Document12 pagesBÀI TẬP CỦNG CỐ TUẦN 1Nguyệt ÁnhNo ratings yet
- An Islamic CBT Approach For Helping Clients With Gender Identity and Sexual Orientation ProblemsDocument26 pagesAn Islamic CBT Approach For Helping Clients With Gender Identity and Sexual Orientation ProblemsNadiyah EliasNo ratings yet
- SDL 2 Wound and Wound HealingDocument4 pagesSDL 2 Wound and Wound HealingDn Ezrinah Dn EshamNo ratings yet
- Case 4Document14 pagesCase 4bekbekk cabahugNo ratings yet
- To Study The Efficacy of Nirgundipatra Swaras Taila Karnapurana in The Management of Pootikarna With Special Reference To Chronic Suppurative Otitis MediaDocument6 pagesTo Study The Efficacy of Nirgundipatra Swaras Taila Karnapurana in The Management of Pootikarna With Special Reference To Chronic Suppurative Otitis MediaEditor IJTSRDNo ratings yet
- Advance Copy 2022 NEGRIHP Final ManuscriptDocument440 pagesAdvance Copy 2022 NEGRIHP Final ManuscriptSchool NursingNo ratings yet
- Intimate Partner Violence Among Pregnant Women inDocument6 pagesIntimate Partner Violence Among Pregnant Women inNove Claire Labawan EnteNo ratings yet
- Metabolism Clinical and ExperimentalDocument4 pagesMetabolism Clinical and ExperimentalusingwebNo ratings yet
- The Boston Globe 30 10 2020 PDFDocument40 pagesThe Boston Globe 30 10 2020 PDFDeadnightvikernesNo ratings yet
- Dignity in Death and Dying: Joyce D. Cajigal, RNDocument14 pagesDignity in Death and Dying: Joyce D. Cajigal, RNWendell Gian GolezNo ratings yet
- Song Review I Lived by OnerepublicDocument2 pagesSong Review I Lived by OnerepublicNur AdilaNo ratings yet
- CKD PDFDocument15 pagesCKD PDFJendrale SudirmanNo ratings yet
- Going All-In For Well-BeingDocument6 pagesGoing All-In For Well-BeingarielNo ratings yet
- The Independent Review of Childrens Social Care Final ReportDocument278 pagesThe Independent Review of Childrens Social Care Final ReportNeil ShellardNo ratings yet
- COPARDocument21 pagesCOPAREdra VillanuevaNo ratings yet