Professional Documents
Culture Documents
Tesis Fenotipos de Sibilancias Infancia y Adolescentes
Tesis Fenotipos de Sibilancias Infancia y Adolescentes
Uploaded by
María Nurys Acevedo CerchiaroOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Tesis Fenotipos de Sibilancias Infancia y Adolescentes
Tesis Fenotipos de Sibilancias Infancia y Adolescentes
Uploaded by
María Nurys Acevedo CerchiaroCopyright:
Available Formats
ORIGINAL RESEARCH
Distinguishing Wheezing Phenotypes from Infancy to Adolescence
A Pooled Analysis of Five Birth Cohorts
Ceyda Oksel1, Raquel Granell2, Sadia Haider1, Sara Fontanella1, Angela Simpson3, Steve Turner4, Graham Devereux5,
Syed Hasan Arshad6,7, Clare S. Murray3, Graham Roberts6,7,8, John W. Holloway6,8, Paul Cullinan9, John Henderson2*,
and Adnan Custovic1*; on behalf of STELAR‡ and Breathing Together Investigatorsx
1
Department of Paediatrics, and 9National Heart and Lung Institute, Imperial College London, London, United Kingdom; 2MRC Integrative
Epidemiology Unit, Department of Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, United Kingdom; 3Division
of Infection, Immunity and Respiratory Medicine, School of Biological Sciences, Faculty of Biology, Medicine and Health, University of
Manchester, Manchester, United Kingdom; 4Child Health, University of Aberdeen, Aberdeen, United Kingdom; 5Liverpool School of Tropical
Medicine, Liverpool, United Kingdom; 6David Hide Asthma and Allergy Research Centre, Isle of Wight, United Kingdom; 7Respiratory
Biomedical Research Unit, University Hospitals Southampton NHS Foundation Trust, Southampton, United Kingdom; and 8Human
Development and Health, Faculty of Medicine, University of Southampton, Southampton, United Kingdom
ORCID ID: 0000-0001-8393-5060 (S.T.).
Abstract vital capacity in adolescence. The association with asthma was
strongest for persistent wheeze (adjusted odds ratio, 56.54; 95%
Rationale: Pooling data from multiple cohorts and extending the confidence interval, 43.75–73.06). We observed considerable within-
time frame across childhood should minimize study-specific effects, class heterogeneity at the individual level, with 913 (12%) children
enabling better characterization of childhood wheezing. having low membership probability (,0.60) of any phenotype.
Class membership certainty was highest in persistent and
Objectives: To analyze wheezing patterns from early childhood to never/infrequent, and lowest in late-onset wheeze (with 51% of
adolescence using combined data from five birth cohorts. participants having membership probabilities ,0.80). Individual
Methods: We used latent class analysis to derive wheeze phenotypes wheezing patterns were particularly heterogeneous in late-onset
among 7,719 participants from five birth cohorts with complete report wheeze, whereas many children assigned to early onset preschool
of wheeze at five time periods. We tested the associations of derived remitting class reported wheezing at later time points.
phenotypes with late asthma outcomes and lung function, and Conclusions: All wheeze phenotypes had significantly diminished
investigated the uncertainty in phenotype assignment. lung function in school-age children, suggesting that the notion that
Results: We identified five phenotypes: never/infrequent wheeze early life episodic wheeze has a benign prognosis may not be true for
(52.1%), early onset preschool remitting (23.9%), early onset a proportion of transient wheezers. We observed considerable
midchildhood remitting (9%), persistent (7.9%), and late-onset within-phenotype heterogeneity in individual wheezing patterns.
wheeze (7.1%). Compared with the never/infrequent wheeze, all
phenotypes had higher odds of asthma and lower forced expiratory Keywords: wheezing phenotypes; childhood; adolescence; latent
volume in 1 second and forced expiratory volume in 1 second/forced class
(Received in original form November 29, 2018; accepted in final form March 19, 2019 )
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial No Derivatives License 4.0 (http://
creativecommons.org/licenses/by-nc-nd/4.0/). For commercial usage and reprints, please contact Diane Gern (dgern@thoracic.org).
*These authors contributed equally.
‡
A complete list of members may be found before the beginning of the REFERENCES.
x
A complete list of members may be found before the beginning of the REFERENCES.
Author Contributions: C.O., R.G., J.H., and A.C. conceived and planned the study and wrote the manuscript. C.O. and R.G. analyzed the data. S.H., S.F., A.S.,
S.T., G.D., S.H.A., C.S.M., G.R., J.W.H., and P.C. contributed to the interpretation of the results. All authors provided critical feedback and helped shape the
research, analysis, and manuscript.
Correspondence and requests for reprints should be addressed to Professor John Henderson, M.D., Department of Population Health Sciences, Bristol Medical
School, University of Bristol, 1-5 Whiteladies Road, Bristol BS8 1NU, UK. E-mail: A.J.Henderson@bristol.ac.uk.
This article has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Ann Am Thorac Soc Vol 16, No 7, pp 868–876, Jul 2019
Copyright © 2019 by the American Thoracic Society
DOI: 10.1513/AnnalsATS.201811-837OC
Internet address: www.atsjournals.org
868 AnnalsATS Volume 16 Number 7 | July 2019
ORIGINAL RESEARCH
Wheezing is one of the most common phenotype should be used to compensate for Data Sources and Definition of
symptoms in infants and young children. uncertainty in phenotype assignment (3, 16). Outcomes
Childhood wheezing is highly We propose that pooling data from Validated questionnaires were completed
heterogeneous (1–4), and distinguishing multiple birth cohorts and extending the time on multiple occasions from infancy to
subtypes of wheezing and their underlying frame from early childhood to adolescence adolescence (14 time points in ALSPAC
mechanisms is a prerequisite to develop should minimize study-specific effects, over 16.5 yr, 7 in ASHFORD over 14 yr, 6 in
interventions to target children whose thereby enabling us to better understand the MAAS over 16 yr, 6 in SEATON over 14 yr,
wheezing persists, while avoiding true variation in the natural history of and 5 in IOW over 18 yr). The cohort-
overtreatment of transient wheeze (5). wheezing, and the individual differences specific time points and sample size
Over the last two decades, substantial within apparently homogeneous phenotypes. included in this analysis are shown in Table
effort has been devoted to understanding the We therefore proceeded to analyze wheezing E1 in the online supplement. We used data
heterogeneity of childhood wheezing (5–9). patterns from early childhood to adolescence/ on current wheeze collected at proximate
In a pioneering study using clinical insights young adulthood using combined data from time periods across cohorts: infancy (0.5–
about the age of onset, progression, and five birth cohorts in the U.K. STELAR 1 yr), early childhood (2–3 yr), preschool/
remission of wheezing, Martinez and consortium (6), and their associations with early school age (4–5 yr), middle childhood
coworkers (1) described three mutually early life risk factors, asthma-related (8–10 yr), and adolescence (14–18 yr).
exclusive wheezing phenotypes (transient outcomes, and lung function measures in late Current wheeze was defined as a positive
early, late-onset, and persistent). These childhood. We then investigated the extent of response to the question “Has your child
findings were confirmed in several uncertainty in phenotype assignment, and had wheezing or whistling in the chest in the
independent cohorts (4, 10, 11). individual variations in wheezing within and last 12 months?” Definitions of other
Subsequently, the approach to discovering across phenotypes. variables are provided in the online
longitudinal wheezing phenotypes was We acknowledge that the wheeze supplement (see Table E2).
extended to data-driven approaches, such as classes discovered using data-driven Skin prick testing was performed at age
the latent class analysis (LCA), which approaches are not observed but are 4 years in IOW; age 5 years in SEATON,
suggested the existence of one or two (12) latent by nature, and ideally should not be ASHFORD, and MAAS; and 7.5 years in
further intermediate phenotypes. However, referred to as “phenotypes” (i.e., observable ALSPAC. Allergic sensitization was defined
although phenotypes derived using LCA in characteristics); however, because the term as a wheal diameter of 3 mm greater than the
different studies are usually designated with “phenotype” has been used in this context negative control to one or more common
the same name, they often differ in temporal for more than a decade, we maintain this allergens.
trajectories, distributions within a nomenclature in this manuscript. We performed spirometry and
population, and associated risk factors (9). recorded forced expiratory volume in one
This is in part a consequence of the second (FEV1) and forced vital capacity
study characteristics, including sample Methods (FVC). To reduce variability, we restricted
size and the timing and frequency of data our analyses to lung function measured at
collection (8). Study Design, Setting, and comparable ages (8.5 yr in ALSPAC, 10 yr in
A further reason may arise from the Participants SEATON and IOW, and 11 yr in MAAS).
heterogeneity between children within The STELAR consortium (6) brings
each phenotype, which has seldom been together five U.K. population-based birth Statistical Analysis
investigated. For example, in most LCA cohorts: Avon Longitudinal Study of Parents A detailed description of statistical analysis
models, there are individuals who cannot be and Children (ALSPAC) (17), Ashford is presented in the online supplement.
classified with a high degree of certainty. (ASHFORD) (18), and Isle of Wight (IOW) Briefly, we used LCA to identify longitudinal
Latent class model estimates class (4, 19) cohorts; Manchester Asthma and trajectories of wheeze among 7,719 children
membership probabilities (each individual’s Allergy Study (MAAS) (20); and the with complete data on wheezing at five time
probability of membership of each class), Aberdeen Study of Eczema and Asthma to periods. Cohort ID was included as an
which are traditionally used to assign Observe the Effects of Nutrition (SEATON) additional covariate by transforming the
individuals to the latent class with the highest (21). The cohorts are described in detail in five-category variable into a set of four
posterior probability (13–15). the online supplement. All studies were dummy variables. The optimal number of
Such maximum-probability phenotype approved by research ethics committees. classes was selected based on the Bayesian
assignment is equivalent to fixing individuals’ Informed consent was obtained from information criterion and interpretability.
membership probabilities of their highest parents, and study subjects gave their assent/ We repeated analyses among 15,941
phenotype to 1 and all others to 0, and may consent when applicable. Data were children with at least two observations, and
introduce within-class heterogeneity. imported into a web-based knowledge examined the stability of allocation of 7,719
Therefore, models that are weighted for the management platform, Asthma eLab children with complete data to their most
probability of each subject belonging to each (www.asthmaelab.org) (6). probable class when using a larger but
Supported by the Wellcome Trust Strategic Award (108,818/15/Z). STELAR consortium is funded by the UK Medical Research Council (Grants G0601361 and
MR/K002449/1). The U.K. Medical Research Council and the Wellcome Trust (Grant 102,215/2/13/2) and the University of Bristol provide core support for
ALSPAC.
Oksel, Granell, Haider, et al.: Distinguishing Wheezing Phenotypes 869
ORIGINAL RESEARCH
incomplete data set. We also assessed the Table E3, see online supplement for more Wheeze Phenotypes, Family History,
stability of the optimal number of classes details on model selection). Trajectories of Early Life Factors, Environmental
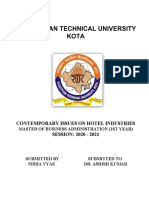
excluding the largest cohort, ALSPAC. To wheeze for each class are shown in Figure 1. Exposures, and Atopy
understand how children are reassigned to Based on the onset and duration of wheeze, Results of univariate analyses among
different phenotypes when the number of the classes were labeled as 1) never/ participants with complete and incomplete
phenotypes increases, we compared LCA infrequent wheeze (52.1%); 2) early onset data are shown in Tables E4 and E5. Table
models constrained to four classes to models preschool remitting wheeze (23.9%), with E6 shows results of multivariable logistic
with five classes. 50–60% prevalence of wheeze during regression models weighted for the probability
We then examined the relationships of infancy, decreasing to 20% around early of each individual belonging to each
the derived phenotypes with asthma and childhood and to less than 10% afterward; 3) phenotype, using the never/infrequent wheeze
asthma medication use at the latest follow- early onset midchildhood remitting wheeze as the reference. Males had a higher risk of
up, and lung function (z scores for adjusted (9%), with early onset and peak prevalence developing the three early onset phenotypes,
FEV1, FVC, and FEV1/FVC) using logistic (z75%) in preschool/early school age, but not late-onset wheezing. Maternal asthma
regression models weighted for the decreasing to 23% in midchildhood, and was associated with all four phenotypes, with
probability of each individual belonging to diminishing further by adolescence; 4) the strongest association with persistent
each phenotype. Models were adjusted for persistent wheeze (7.9%) with 53% wheeze wheezing (RRR, 3.12; 95% CI, 2.5123.89;
potential confounders, including allergic prevalence during infancy, and an P , 0.0001). Compared with never/
sensitization (midchildhood), maternal increasing prevalence thereafter to a high infrequent wheeze, all wheezing phenotypes
history of asthma/allergy, maternal prevalence of approximately 80%; and 5) except early onset preschool remitting wheeze,
smoking, and low birth weight. We used late-onset wheeze (7.1%) with a low showed significant associations with maternal
weighted multinomial logistic regression prevalence of 27% until preschool/early smoking during pregnancy. There was little
models to ascertain early life risk factors school age, increasing rapidly to a peak evidence of association between wheeze
associated with each phenotype; results are prevalence of 74% in adolescence. phenotypes and pet ownership or paternal
reported as relative risk ratios (RRR) with Characteristics of children across different smoking. Paternal asthma was significantly
95% confidence intervals (CI). phenotypes are presented in Table 1. LCA of associated with persistent wheeze in both
We then investigated individual four cohorts with complete data (excluding genders, but was a predictor of late-onset
variations in wheezing within and across ALSPAC) provided very similar results. wheeze in males only (see Table E4).
phenotypes. We defined categories of class Figure 2A shows the changes in the The strongest association with allergic
membership certainty based on class allocation of 7,719 individuals with sensitization (ages 4–7.5 yr) was observed
membership probabilities (high >0.80, complete data from the model using only for persistent wheeze (RRR, 5.12; 95% CI,
medium = 0.60–0.80, low ,0.60) to elicit the children with data on wheezing at all five 4.0426.47; P , 0.0001). Two early onset
extent of within-class homogeneity in time periods to their most probable class in remitting classes differed substantially in
different certainty thresholds. Analyses were the model using 15,941 individuals with at their association with sensitization: there
performed using Mplus 8, R (http://www.r‐ least two observations. The optimal solution was little evidence of association between
project.org/) and Stata 14 (StataCorp). in the model using 15,941 children sensitization and preschool remitting
remained five classes (see Table E3, Figure wheeze, but clear evidence of an association
E1), and was very similar to that derived between sensitization and midchildhood
Results from a complete data set. Never/infrequent remitting wheeze (RRR, 1.61; 95% CI, 1.24–
and persistent phenotype assignments were 2.11; P , 0.0001).
Characteristics of the Study very stable, but there were considerable
Population transitions between other classes (e.g., 39% Asthma and Lung Function
Of 7,719 children with complete data on of children assigned to the early onset Associations of wheeze phenotypes with
wheezing, 50.3% were male, 14.1% had midchildhood remitting wheeze using current asthma and asthma medication use
current asthma, and 13.4% reported using complete data were assigned to persistent at the last follow-up are shown in Table 2.
asthma medication at the last available wheeze in the model with incomplete data). Compared with never/infrequent wheeze, all
follow-up. Mean (standard deviation) birth To understand how class allocation four wheeze phenotypes were associated
weight in the combined dataset was 3.44 kg changes in models with increasing number with higher asthma prevalence. This
(0.53), with 314 (4.1%) children having a of phenotypes, we compared LCA models association was weakest for early onset
low birth weight (<2.5 kg); mean maternal with four and five phenotypes using preschool remitting wheeze (RRR, 2.28; 95%
age at delivery was 29.1 years (standard complete data (Figure 2B). Never/ CI, 1.76–2.96 P , 0.0001) and strongest for
deviation, 4.64), and 1,198 (16%) mothers infrequent and late-onset phenotypes were persistent wheeze (RRR, 56.54; 95% CI,
reported smoking during pregnancy similar in both models. With the addition 43.75–73.06; P , 0.0001). We obtained
(Table 1). of a fifth phenotype, transient-early wheeze similar results in the analysis of 8,223
divided into two remitting classes children with incomplete reports of
Wheeze Phenotypes from Infancy to (preschool and midchildhood resolution), wheezing (excluding 7,719 children with
Adolescence and Transitions in whereas a third of children from the complete reports at five time points) (see
Phenotype Membership persistent wheeze in a four-class solution Table E7). Characteristics of children with
A five-class solution was selected as the transitioned, mainly to early onset complete report of wheeze and those with
optimal model based on statistical fit (see midchildhood remitting wheeze. missing data are shown in Table E8.
870 AnnalsATS Volume 16 Number 7 | July 2019
ORIGINAL RESEARCH
Table 1. Per cohort and combined characteristics of children with complete reports of wheezing
Most Likely Wheezing Phenotypes
Never/Infrequent Early Onset Early Onset Persistent Late
Wheeze Preschool Midchildhood Onset
Remitting Remitting
SEATON, n (%) 499 305 (61) 108 (22) 16 (3) 31 (6) 39 (8)
ALSPAC, n (%) 5,149 3,119 (61) 1,058 (20) 476 (9) 253 (5) 243 (5)
MAAS, n (%) 667 421 (63) 96 (14) 34 (5) 84 (13) 32 (5)
Ashford, n (%) 492 233 (47) 176 (36) 28 (6) 50 (10) 5 (1)
IOW, n (%) 912 548 (60) 46 (5) 37 (4) 66 (7) 215 (24)
5-Cohort data, n (%) 7,719 4,626 (60) 1,484 (19) 591 (8) 484 (6) 534 (7)
Sex Male, n (%) 3,881 (50) 2,162 (47) 830 (56) 343 (58) 288 (60) 258 (48)
Birth weight, kg Mean (SD) 3.44 (0.53) 3.44 (0.51) 3.46 (0.54) 3.41 (0.58) 3.48 (0.57) 3.43 (0.52)
Low birth weight (<2.5) Yes, n (%) 314 (4.1) 161 (3) 63 (4) 36 (6) 31 (6) 23 (4)
Maternal age Mean (SD) 29.1 (4.64) 29.2 (4.57) 28.9 (4.58) 28.8 (4.73) 28.7 (4.78) 28.8 (5.07)
Advanced maternal Yes, n (%) 947 (12) 572 (13) 177 (12) 72 (12) 53 (11) 73 (14)
age (>35)
Maternal smoking Yes, n (%) 6,491 (16) 647 (14) 249 (17) 117 (20) 88 (18) 97 (18)
Paternal smoking Yes, n (%) 1,702 (27) 979 (26) 306 (25) 144 (31) 132 (32) 141 (29)
Pet ownership Yes, n (%) 4,149 (54) 2,449 (54) 818 (56) 334 (58) 264 (55) 284 (54)
Sensitization (midchildhood) Yes, n (%) 1,042 (17) 461 (13) 134 (12) 106 (23) 181 (47) 160 (39)
Current asthma (last Yes, n (%) 1,000 (14) 121 (3) 113 (8) 86 (15) 352 (75) 328 (67)
follow-up)
Asthma ever Yes, n (%) 1,737 (26) 452 (11) 291 (24) 274 (59) 374 (91) 346 (72)
Asthma medication (last Yes, n (%) 949 (13) 120 (3) 113 (8) 87 (15) 345 (73) 284 (58)
follow-up)
Asthma medication ever Yes, n (%) 2,125 (42) 591 (14) 294 (20) 374 (64) 451 (93) 415 (89)
Definition of abbreviations: ALSPAC = Avon Longitudinal Study of Parents and Children; IOW = Isle of Wight; MAAS = Manchester Asthma and Allergy Study;
SD = standard deviation; SEATON = Aberdeen Study of Eczema and Asthma to Observe the Effects of Nutrition study.
Associations of wheeze phenotypes never/infrequent class. Association was Individual Variation within and across
with lung function in middle childhood particularly strong for persistent wheeze Wheezing Phenotypes
(8.5–11 yr) are shown in Table 3. FEV1 (z scores 20.60; 95% CI, 20.70 to 20.50; Figure 3 shows the presence/absence of
and FEV1/FVC were significantly lower P , 0.0001). There was no evidence of wheeze at five time periods among each
in all wheeze phenotypes compared with differences in FVC. individual across latent classes, stratified by
0.8
Probability of wheezing
0.6
0.4
0.2
0
Infancy Early Childhood Pre-/Early- Middle Childhood Adolescence
School Age
Never/Infrequent wheeze (52.1%) Early-onset pre-school remitting wheeze (23.9%)
Early-onset mid-childhood remitting wheeze (9.0%) Persistent wheeze (7.9%)
Late-onset wheeze (7.1%)
Figure 1. Estimated prevalence of wheeze for each of the five wheezing phenotypes identified by latent class analysis in 7,719 children (infancy, age 0.521;
early childhood, age 223; preschool age/early school age, age 425; middle childhood, age 8210; adolescence, age 14218). Class proportions shown in
the figure legend are computed based on estimated posterior probabilities.
Oksel, Granell, Haider, et al.: Distinguishing Wheezing Phenotypes 871
ORIGINAL RESEARCH
Complete Data Early-onset Early-onset
Late Never or
Persistent pre-school mid-childhood
onset infrequent
remitting remitting
99% 1% 79% 20% 39% 61% 12% 83% 3% 96%
Incomplete Data
Early-onset Early-onset
Late Never or
Persistent pre-school mid-childhood
onset infrequent
remitting remitting
B
Late Transient Never or
Persistent
onset early infrequent
66% 26% 2% 8% 1% 39% 97% 1% 0.2% 2% 58% 16% 2% 82%
Early-onset Early-onset
Late Never or
Persistent mid-childhood pre-school
onset infrequent
remitting remitting
Figure 2. (A) Transition of most likely membership class between latent models constructed with complete (n = 7,719) and incomplete (n = 15,942) data.
(B) Assignment of children into wheeze phenotypes over a sequence of latent class analysis models with four and five classes based on most likely
membership class. Ellipse nodes show class membership (most likely phenotype), whereas the values along the arrow represent the percentage of children
moving from one class to another. This figure reflects whether the members of distinct wheeze phenotypes will remain in the same group or shift into another.
cohort and class membership certainty. wheezing only once, up to three times wheeze and z0.40 probability of belonging
More than 80% of children in never/ persistently, or intermittently. Of 113 to early onset preschool remitting wheeze).
infrequent and persistent wheeze classes children who were assigned to the early
were assigned with a high degree of certainty onset preschool remitting class, but reported
(membership probability .0.80), whereas current asthma at the last follow-up, 78 Discussion
class membership certainty was the lowest (69%) reported wheezing at later time
for late-onset wheeze, with 51% of its points. By jointly modeling data on parent/self-
members having posterior probabilities Over a tenth of individuals (913/7,719; reported wheezing from birth to adolescence
less than 0.80. Sorting individuals in the 12%) had low posterior probabilities in five population-based birth cohorts, we
vertical space and stratifying them by class (,0.60) of membership to any class identified five distinct phenotypes. In
assignment probability revealed fairly (Figure 3). Figure E2 shows a heat map of addition to never/infrequent wheezing, the
consistent between-individual patterns each individual’s posterior class latent structure of wheezing disorders from
when assignment probability was greater membership probabilities, lying between infancy to adolescence comprised two
than or equal to 0.80, but heterogeneity 0 (low) and 1 (high). Inspection of the figure persisting (early onset and late-onset) and
increased as assignment became less certain reveals that there are individuals whose two remitting (preschool remitting and
(,0.80). Individual wheezing patterns were patterns do not fit well within the assigned midchildhood remitting) phenotypes. The
particularly heterogeneous in late-onset phenotype (e.g., some have z0.40 model assigned 33% of children to remitting
wheeze, whereby participants reported probability of belonging to never/infrequent (24% remitting in preschool, and 9% in
872 AnnalsATS Volume 16 Number 7 | July 2019
ORIGINAL RESEARCH
Table 2. Adjusted associations of wheezing phenotypes with late outcomes including current asthma, asthma ever, current use of
asthma medication, asthma medication ever, and eczema ever using weighted membership probabilities
Adjusted Odds Ratio (95% Cl)*
†
Current Asthma Asthma Ever Current† Asthma Asthma Eczema
Medication Medication Ever Ever
Never/infrequent Reference Reference Reference Reference Reference
Early onset preschool remitting 2.34 2.05 2.35 1.36 1.24
95% Cl 1.73 to 3.17 1.70 to 2.46 1.74 to 3.18 1.14 to 1.62 1.07 to 1.42
P value ,0.0001 ,0.0001 ,0.0001 0.001 0.003
Early onset midchildhood remitting 3.65 6.41 3.53 5.97 1.31
95% Cl 2.55 to 5.21 5.11 to 8.03 2.47 to 5.05 4.85 to 7.35 1.06 to 1.61
P value ,0.0001 ,0.0001 ,0.0001 ,0.0001 0.010
Persistent 48.31 37.95 42.45 38.67 3.22
95% Cl 35.87 to 65.07 27.78 to 51.84 31.57 to 57.09 28.27 to 52.90 2.55 to 4.08
P value ,0.0001 ,0.0001 ,0.0001 ,0.0001 ,0.0001
Late onset 36.39 12.00 24.51 17.75 2.03
95% Cl 26.89 to 49.25 9.41 to 15.31 18.07 to 33.23 13.59 to 23.17 1.62 to 2.53
P value ,0.0001 ,0.0001 ,0.0001 ,0.0001 ,0.0001
Definition of abbreviations: ALSPAC = Avon Longitudinal Study of Parents and Children; CI = confidence interval; IOW = Isle of Wight; MAAS = Manchester
Asthma and Allergy Study; SEATON = Aberdeen Study of Eczema and Asthma to Observe the Effects of Nutrition Study.
*Adjusted for sensitization (midchildhood), sex, maternal history of asthma or allergy, maternal smoking, and low birth weight.
†
Available at the latest follow-up (e.g., 18 yr in IOW, 16 yr in MAAS, 15 yr in SEATON, 15 yr in Ashford, and 14 yr in ALSPAC).
midchildhood), and 15% to persisting associations between wheeze phenotypes cohorts was that a substantial number of
phenotypes (7.9% with onset in early life, and asthma in adolescence confirmed the children were classified imprecisely and did
and 7.1% with onset in later childhood). By validity of derived phenotypes. not follow wheeze patterns suggested by
pooling the cohorts and restricting our To our knowledge, this is the first the label ascribed to the class when the
analyses to participants with complete data, study to investigate the nature of within- individual’s likelihood of belonging to the
we obtained a better representation of the phenotype heterogeneity by looking at assigned class was less than 0.80. Moreover,
latent structure, while maintaining the individual patterns of wheeze within the precision with which children were
power to detect less prevalent phenotypes different thresholds of class assignment. In assigned to a “label” varied across
and making meaningful analyses of their the context of wheeze phenotyping, data- different classes. The greatest level of
associations with risk factors and outcomes. driven techniques, such as LCA, have been uncertainty in assignment was for the late-
This allowed us to determine that an used to discover subgroups within the onset class. This within-class heterogeneity
obstructive pattern of lung function, with study population, which were presumed may, in part, be responsible for a lack
significantly diminished FEV 1 and to be homogeneous. However, we have of consistent associations of phenotypes
FEV 1 /FVC, was a feature of all four demonstrated that this may not always be with risk factors reported in previous
wheeze phenotypes. Differing the case. A consistent finding across all five studies (22).
Table 3. Associations of wheezing phenotypes with lung function measures adjusted for sex, height, and gender using weighted
membership probabilities
Mean Difference (95% Cl)* P value
†
z Scores for FEV1 z Scores for FVC† z Scores for FEV1/FVC†
Never/infrequent Reference Reference Reference
Early onset preschool remitting 20.11 (20.17 to 20.04) 20.05 (20.12 to 0.02) 20.09 (20.16 to 20.02)
0.002 0.144 0.001
Early onset midchildhood remitting 20.19 (20.28 to 20.09) 20.03 (20.13 to 0.06) 20.26 (20.35 to 20.16)
,0.0001 0.531 ,0.0001
Persistent 20.34 (20.44 to 20.24) 0.03 (20.07 to 0.13) 20.60 (20.70 to 20.50)
,0.0001 0.577 ,0.0001
Late onset 20.22 (20.32 to 20.12) 20.04 (20.14 to 0.06) 20.30 (20.40 to 20.20)
,0.0001 0.406 ,0.0001
Definition of abbreviations: CI = confidence interval; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity.
*Adjusted for maternal history of asthma or allergy, maternal smoking, and low birth weight.
†
Sex-, age-, and height-adjusted standard deviation units.
Oksel, Granell, Haider, et al.: Distinguishing Wheezing Phenotypes 873
ORIGINAL RESEARCH
Never/Infrequent Early-onset Early-onset Persistent Late onset
pre-school remitting mid-childhood remitting
N=3,959 (86%) N=1,058 (72%) N=366 (62%) N=390 (80%) N=260 (49%)
ASI MS
MS
AS I MS
I MS
AS I M S
Class Probability 0.8
N=6,033 (78%)
I
AI
AI
AI
AI
AI
N=498 (11%) N=94 (6%) N=15 (2%) N=28 (6%) N=105 (20%)
0.6 Class Probability < 0.8
I MS
I MS
S
N=740 (10%)
M
M
AS
AI
AS
I
I
AI AS
AI
AI
AI
N=169 (3%) N=332 (22%) N=210 (36%) N=66 (14%) N=169 (31%)
ASIS
ASIMS
ASIMS
M S
Class Probability < 0.6
M S
N=913 (12%)
AS
I
AI
AI
AI
AS
AI
AI
TP1 TP2 TP3 TP4 TP5 TP1 TP2 TP3 TP4 TP5 TP1 TP2 TP3 TP4 TP5 TP1 TP2 TP3 TP4 TP5 TP1 TP2 TP3 TP4 TP5
Yes No
Figure 3. Presence/absence of wheeze at five time periods across latent classes stratified by cohort and class membership probabilities that have been
derived by including cohort site as a covariate. Al = Avon Longitudinal Study of Parents and Children; As = Ashford; I = Isle of Wight; M = Manchester Asthma
and Allergy Study; S = Aberdeen Study of Eczema and Asthma to Observe the Effects of Nutrition Study; TP = time period.
One limitation of this multicohort revealing a more accurate picture when phenotypes varied by study, with four
study is the heterogeneity between cohorts integrated together. The integration of five common classes identified in all cohorts:
that were integrated retrospectively (e.g., in cohorts and their pooled analysis enhanced never/infrequent wheeze, transient-early,
recruitment criteria, data collection time the credibility and generalizability of the late-onset, and persistent wheeze. In our joint
and intervals, question types and wording, phenotyping results to the U.K. population. analysis, a four-class solution identified the
and tools for collecting data). We observed A further advantage is to minimize the same classes, whereas the optimum solution
some level of variation in the proportion of study-specific biases (including cohort- included a fifth phenotype, early onset
children allocated to each phenotype in specific effects, attrition effects, different midchildhood remitting wheeze, which was
different cohorts. For example, ASHFORD recruitment strategies, and geographic previously observed in ALSPAC (3, 12, 16)
had the lowest prevalence of late-onset factors) affecting the certainty of allocation but not in another independent cohort (3).
wheeze and highest prevalence of early onset of individuals to each latent class, while School-age onset persisting wheeze that was
remitting wheeze, whereas IOW had the maximizing the benefits of individual cohort previously identified as a sixth phenotype in
lowest prevalence of early onset preschool studies (e.g., potentially important risk ALSPAC (12, 16) was not detected in our
remitting wheeze and the highest prevalence factors and outcomes are captured in some, joint analysis. One possible explanation could
for late-onset wheeze. We addressed this but not all cohorts). Another strength of be that we have focused on common ages that
limitation by including “cohort site” as a pooling cohort data is that a multicohort are approximately shared across all cohorts to
covariate for determining phenotypes. design allowed us to analyze a large sample ensure compatibility, resulting in the
One of the advantages of our with complete data on wheeze from birth to exclusion of potentially informative time
multicohort approach is that individual adolescence, thus increasing statistical points for identifying additional phenotypes
studies that might not provide conclusive power to detect less prevalent phenotypes. (8). An alternative explanation is that some
evidence to make inference about the Several birth cohorts have investigated phenotypes may arise as an artifact of the
general population because of cohort- wheeze phenotypes in childhood (1–4, analysis (e.g., caused by the increasing data
specific effects and biases can contribute to 10–12, 16, 23–26). The number of derived collection frequency).
874 AnnalsATS Volume 16 Number 7 | July 2019
ORIGINAL RESEARCH
When using 15,941 children with at have longer wheeze duration in association certain. Individual wheezing patterns were
least two observations of wheeze, individual with the development of sensitization. Most particularly heterogeneous in the late-onset
allocation to persistent and never/infrequent previous studies have shown that lung wheeze. It is also of note that a proportion of
phenotypes was consistent with the analysis function is impaired in some, but not all children in the early onset preschool
using 7,719 complete cases, but there was a wheeze phenotypes (11, 23, 24). In our remitting class reported wheezing at later
considerable transition in other classes (e.g., study, all wheeze phenotypes were time points. This can explain the increased
almost 40% of children in early onset associated with diminished lung function risk of asthma in transient wheezers,
midchildhood remitting class from compared with never/infrequent wheeze, because approximately 70% of individuals
complete data switched to persistent with the greatest impairment in persistent with later-life asthma within this class
wheeze). This finding raises questions about wheeze. This is particularly important in the reported wheezing beyond age 10.
the confidence with which allocation to early context of findings that low FEV1 at its In conclusion, our results suggest that
onset remitting classes can be applied in physiologic plateau in early adult age is early life episodic wheeze may not have a
cohorts with considerable missing data. important in the genesis of chronic benign prognosis for a proportion of
The analyses to understand how children’s obstructive pulmonary disease (27) and transient wheezers. Up to 12% of children
class allocations changed from one early cardiovascular mortality (28). Several have low membership probability of any
phenotype to another in models with recent studies have shown that low wheezing phenotype, and the mere presence
increasing number of classes have shown childhood lung function trajectory is or absence of a wheeze may be insufficient to
that when moving from a four- to five-class associated with future chronic obstructive derive homogenous phenotypes for probing
solution, transient early wheeze was pulmonary disease risk (29–31), and our causality. It is likely that more holistic
divided into two remitting classes. findings of impaired lung function in indicators of wheeze (including frequency
Preschool remitting phenotype included school age across all childhood wheezing and severity) are needed to describe
children who were assigned to transient early phenotypes suggest that the notion that individual trajectories and derive more
and never/infrequent wheeze, whereas episodic wheeze in early life has a benign homogenous phenotypes to facilitate better
midchildhood remitting phenotype was long-term prognosis may not be true for a understanding of the natural history and
formed by children assigned to transient early proportion of transient wheezers. causality of childhood wheezing illness. n
and persistent wheeze in a four-class model. It is often stated that temporal analyses
These newly formed remitting phenotypes may be crucial for distinguishing between Author disclosures are available with the text
showed different associations with risk different endotypes of asthma (6), and that of this article at www.atsjournals.org.
factors, lung function, and later asthma, derived latent classes (“phenotypes”) may be
suggesting that they may be distinct entities, used to improve discovery process in genetic STELAR investigators: Dr. John Curtin, Silvia
Colicino, and Professor Ashley Woodcock.
or that phenotype allocation also reflects and environmental studies (5). However, to
wheeze severity. date, there has been a lack of consistency in Breathing Together investigators: Professor
We have extended previous associations between wheeze phenotypes Andrew Bush, Professor Sejal Saglani, Professor
observations of the association between and genetic and environmental factors, and Clare M. Lloyd, Dr. Benjamin Marsland, Professor
persistent and late-onset wheezing with a scarcity of information on temporal Jonathan Grigg, Professor Jurgen Schwarze,
allergic sensitization (1), by demonstrating characteristics of individual profiles of Professor Mike Shields, Dr. Peter Ghazal, and
Dr. Multan Power.
that two early onset remitting classes symptoms within the longitudinal latent
differed in their association with classes. Our findings suggest that one of the Acknowledgment: The authors thank all the
sensitization: there was little evidence reasons for the inconsistencies may be families who took part in this study; the midwives
of association between sensitization because associations are diluted due to for their help in recruiting them; and the MAAS,
and preschool remitting wheeze, but within-phenotype heterogeneity. We IOW, Ashford, SEATON, and ALSPAC teams,
which includes interviewers, computer and
sensitization was strongly associated with observed considerable within-class laboratory technicians, clerical workers, research
midchildhood remitting wheeze. This heterogeneity in wheezing patterns, which scientists, volunteers, managers, receptionists,
suggests that some transient wheezers may increased as the assignment became less and nurses.
References 5 Deliu M, Belgrave D, Sperrin M, Buchan I, Custovic A. Asthma
phenotypes in childhood. Expert Rev Clin Immunol 2017;13:705–713.
1 Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan 6 Howard R, Rattray M, Prosperi M, Custovic A. Distinguishing asthma
WJ; The Group Health Medical Associates. Asthma and wheezing in phenotypes using machine learning approaches. Curr Allergy Asthma
the first six years of life. N Engl J Med 1995;332:133–138. Rep 2015;15:38.
2 Belgrave DC, Simpson A, Semic-Jusufagic A, Murray CS, Buchan I, 7 Saglani S, Custovic A. Childhood asthma: advances using
Pickles A, et al. Joint modeling of parentally reported and physician- machine learning and mechanistic studies. Am J Respir Crit Care
confirmed wheeze identifies children with persistent troublesome Med 2019;199:414–422.
wheezing. J Allergy Clin Immunol 2013;132:575–583. 8 Oksel C, Granell R, Mahmoud O, Custovic A, Henderson AJ; STELAR;
3 Savenije OE, Granell R, Caudri D, Koppelman GH, Smit HA, Wijga A, Breathing Together investigators. Causes of variability in latent
et al. Comparison of childhood wheezing phenotypes in 2 birth phenotypes of childhood wheeze. J Allergy Clin Immunol 2019;143:
cohorts: ALSPAC and PIAMA. J Allergy Clin Immunol 2011;127:1505–1512. 1783–1790.
4 Kurukulaaratchy RJ, Fenn MH, Waterhouse LM, Matthews SM, Holgate 9 Oksel C, Haider S, Fontanella S, Frainay C, Custovic A. Classification of
ST, Arshad SH. Characterization of wheezing phenotypes in the first pediatric asthma: from phenotype discovery to clinical practice. Front
10 years of life. Clin Exp Allergy 2003;33:573–578. Pediatr 2018;6:258.
Oksel, Granell, Haider, et al.: Distinguishing Wheezing Phenotypes 875
ORIGINAL RESEARCH
10 Cano-Garcinuño A, Mora-Gandarillas I; SLAM Study Group. Wheezing the first two years of life. Am J Respir Crit Care Med 2005;171:
phenotypes in young children: an historical cohort study. Prim Care 121–128.
Respir J 2014;23:60–66. 22 Belgrave DC, Custovic A, Simpson A. Characterizing wheeze
11 Lowe LA, Simpson A, Woodcock A, Morris J, Murray CS, Custovic A; phenotypes to identify endotypes of childhood asthma, and the
NAC Manchester Asthma and Allergy Study Group. Wheeze implications for future management. Expert Rev Clin Immunol 2013;9:
phenotypes and lung function in preschool children. Am J Respir Crit 921–936.
Care Med 2005;171:231–237. 23 Duijts L, Granell R, Sterne JA, Henderson AJ. Childhood wheezing
12 Henderson J, Granell R, Heron J, Sherriff A, Simpson A, Woodcock A, phenotypes influence asthma, lung function and exhaled nitric oxide
et al. Associations of wheezing phenotypes in the first 6 years of life
fraction in adolescence. Eur Respir J 2016;47:510–519.
with atopy, lung function and airway responsiveness in mid-
24 Morgan WJ, Stern DA, Sherrill DL, Guerra S, Holberg CJ, Guilbert TW,
childhood. Thorax 2008;63:974–980.
et al. Outcome of asthma and wheezing in the first 6 years of life:
13 Depner M, Fuchs O, Genuneit J, Karvonen AM, Hyvärinen A, Kaulek V,
et al.; PASTURE Study Group. Clinical and epidemiologic phenotypes follow-up through adolescence. Am J Respir Crit Care Med 2005;172:
of childhood asthma. Am J Respir Crit Care Med 2014;189:129–138. 1253–1258.
14 Siroux V, Basagaña X, Boudier A, Pin I, Garcia-Aymerich J, Vesin A, et al. 25 Sherriff A, Peters TJ, Henderson J, Strachan D. Risk factor associations
Identifying adult asthma phenotypes using a clustering approach. Eur with wheezing patterns in children followed longitudinally from birth to
Respir J 2011;38:310–317. 3 1/2 years. Int J Epidemiol 2001;30:1473–1484.
15 Spycher BD, Silverman M, Pescatore AM, Beardsmore CS, Kuehni CE. 26 van der Valk RJ, Caudri D, Savenije O, Koppelman GH, Smit HA, Wijga
Comparison of phenotypes of childhood wheeze and cough in 2 AH, et al. Childhood wheezing phenotypes and FeNO in atopic
independent cohorts. J Allergy Clin Immunol 2013;132:1058–1067. children at age 8. Clin Exp Allergy 2012;42:1329–1336.
16 Granell R, Henderson AJ, Sterne JA.Associations of wheezing 27 Lange P, Celli B, Agustı́ A, Boje Jensen G, Divo M, Faner R, et al. Lung-
phenotypes with late asthma outcomes in the Avon Longitudinal function trajectories leading to chronic obstructive pulmonary
Study of Parents and Children: A population-based birth cohort. J disease. N Engl J Med 2015;373:111–122.
Allergy Clin Immunol 2016;138:1060–1070. 28 Vasquez MM, Zhou M, Hu C, Martinez FD, Guerra S. Low lung function in
17 Golding J, Pembrey M, Jones R; ALSPAC Study Team. ALSPAC-the young adult life is associated with early mortality. Am J Respir Crit
Avon longitudinal study of parents and children. I. Study Care Med 2017;195:1399–1401.
methodology. Paediatr Perinat Epidemiol 2001;15:74–87. 29 Berry CE, Billheimer D, Jenkins IC, Lu ZJ, Stern DA, Gerald LB, et al. A
18 Atkinson W, Harris J, Mills P, Moffat S, White C, Lynch O, et al. Domestic distinct low lung function trajectory from childhood to the fourth
aeroallergen exposures among infants in an English town. Eur Respir J
decade of life. Am J Respir Crit Care Med 2016;194:607–612.
1999;13:583–589.
30 Bui DS, Lodge CJ, Burgess JA, Lowe AJ, Perret J, Bui MQ, et al.
19 Kurukulaaratchy RJ, Fenn M, Twiselton R, Matthews S, Arshad SH. The
Childhood predictors of lung function trajectories and future COPD
prevalence of asthma and wheezing illnesses amongst 10-year-old
schoolchildren. Respir Med 2002;96:163–169. risk: a prospective cohort study from the first to the sixth decade of
20 Custovic A, Simpson BM, Murray CS, Lowe L, Woodcock A; NAC life. Lancet Respir Med 2018;6:535–544.
Manchester Asthma and Allergy Study Group. The national asthma 31 Belgrave DCM, Granell R, Turner SW, Curtin JA, Buchan IE, Le Souëf
campaign Manchester asthma and allergy study. Pediatr Allergy PN, et al. Lung function trajectories from pre-school age to adulthood
Immunol 2002;13:32–37. and their associations with early life factors: a retrospective analysis of
21 Martindale S, McNeill G, Devereux G, Campbell D, Russell G, Seaton A. three population-based birth cohort studies. Lancet Respir Med 2018;
Antioxidant intake in pregnancy in relation to wheeze and eczema in 6:526–534.
876 AnnalsATS Volume 16 Number 7 | July 2019
You might also like
- ShakeDocument4 pagesShakesafak100% (3)
- WheezingRhinovirusIllnessesinEarlyLifePredict667 FullDocument6 pagesWheezingRhinovirusIllnessesinEarlyLifePredict667 Fullagungtn1No ratings yet
- Wheezing Phenotypes in PreschoolersDocument4 pagesWheezing Phenotypes in PreschoolersRannyNo ratings yet
- 2000 - IsaacDocument6 pages2000 - IsaacPaul ParrasNo ratings yet
- Global and Regional PrevalenceDocument13 pagesGlobal and Regional PrevalenceMacarena AlvarezNo ratings yet
- Radziavicius Et AlDocument7 pagesRadziavicius Et AlÉrica Engrácia ValentiNo ratings yet
- Effect of Aspiration On The Lungs in Children: A Comparison Using Chest Computed Tomography FindingsDocument7 pagesEffect of Aspiration On The Lungs in Children: A Comparison Using Chest Computed Tomography FindingsYuliaAntolisNo ratings yet
- Original Contribution Increased Prevalence of Sleep-Disordered Breathing in AdultsDocument12 pagesOriginal Contribution Increased Prevalence of Sleep-Disordered Breathing in AdultsAsti Sauna MentariNo ratings yet
- FEV Is Associated With Risk of Asthma Attacks in A Pediatric PopulationDocument7 pagesFEV Is Associated With Risk of Asthma Attacks in A Pediatric PopulationdelphineNo ratings yet
- Obesity and The Risk of Newly Diagnosed Asthma in School-Age ChildrenDocument10 pagesObesity and The Risk of Newly Diagnosed Asthma in School-Age ChildrenMar LindaNo ratings yet
- Humrep Des398 FullDocument9 pagesHumrep Des398 FullKinjal ShahNo ratings yet
- Asma 2Document7 pagesAsma 2alexvamaNo ratings yet
- T5 - Phenotypes of Wheezing and Asthma in Preschool Children Free AccesDocument11 pagesT5 - Phenotypes of Wheezing and Asthma in Preschool Children Free AccesAbby AldeaNo ratings yet
- Outcome in Childhood Guillain-Barré SyndromeDocument5 pagesOutcome in Childhood Guillain-Barré SyndromechristianFPTNo ratings yet
- 2019 - Changing Conceptualizations of Regression in Autism - OzonoffDocument9 pages2019 - Changing Conceptualizations of Regression in Autism - OzonoffJesus RiveraNo ratings yet
- Insecure Attachment in Severely Asthmatic Preschool ChildrenDocument5 pagesInsecure Attachment in Severely Asthmatic Preschool ChildrenMatt Van VelsenNo ratings yet
- KneeDocument10 pagesKneeidhamNo ratings yet
- The Oral HealthDocument7 pagesThe Oral HealthMario Zúñiga GonzalesNo ratings yet
- Foreign BodyDocument11 pagesForeign BodyVania Dwi AndhaniNo ratings yet
- Risk Factors For Persistence of Bilateral Otitis Media With EffusionDocument10 pagesRisk Factors For Persistence of Bilateral Otitis Media With EffusionCamila Abad ZapataNo ratings yet
- Wheezing in Children Approaches To Diagnosis and MDocument6 pagesWheezing in Children Approaches To Diagnosis and MMemory LastNo ratings yet
- BF and Otitis MediaDocument6 pagesBF and Otitis MediaValériaNo ratings yet
- 1750 1164 8 3 PDFDocument7 pages1750 1164 8 3 PDFRiley RilanNo ratings yet
- Corrigendum: Permanent Magnetic Resonance Elastography Along With Diffusion Heavy Image in The Look at Hepatic Fibrosis in Chronic Liver Disease WDocument1 pageCorrigendum: Permanent Magnetic Resonance Elastography Along With Diffusion Heavy Image in The Look at Hepatic Fibrosis in Chronic Liver Disease Wbombcollar8No ratings yet
- Development of Refractive Accommodative Esotropia in Children Initially Diagnosed With PseudoesotropiaDocument3 pagesDevelopment of Refractive Accommodative Esotropia in Children Initially Diagnosed With Pseudoesotropialuz mila sanchezNo ratings yet
- 2018 Article 1359Document5 pages2018 Article 1359SaskiahNo ratings yet
- Risk Factors For Sleep-Disordered Breathing in Children: Associations With Obesity, Race, and Respiratory ProblemsDocument6 pagesRisk Factors For Sleep-Disordered Breathing in Children: Associations With Obesity, Race, and Respiratory ProblemsMiral BassNo ratings yet
- OSAHS in Adolescents: Clinical Presentation and Differential DiagnosisDocument8 pagesOSAHS in Adolescents: Clinical Presentation and Differential Diagnosisdrzana78No ratings yet
- Mishra2017 PDFDocument9 pagesMishra2017 PDFJuan Jesus Gomez AlarconNo ratings yet
- Astma1 Jurnal ReadingDocument10 pagesAstma1 Jurnal ReadingRizki NabilaNo ratings yet
- Foreign Body Aspiration in Infants and Older Children: A Comparative StudyDocument5 pagesForeign Body Aspiration in Infants and Older Children: A Comparative Studyharyo wiryantoNo ratings yet
- Risk Factor WheezingDocument8 pagesRisk Factor WheezingliawijayaNo ratings yet
- Treating The Wheezing Infant: Ronina A. Covar, MD, Joseph D. Spahn, MDDocument24 pagesTreating The Wheezing Infant: Ronina A. Covar, MD, Joseph D. Spahn, MDSophia RoseNo ratings yet
- Jurnal AsmaDocument11 pagesJurnal AsmaAi Siti Rika FauziahNo ratings yet
- Effect of Low Birth Weight On Childhood Asthma: A Meta-AnalysisDocument8 pagesEffect of Low Birth Weight On Childhood Asthma: A Meta-Analysisnavali rahmaNo ratings yet
- 2018 - Ajslp 18 0150Document15 pages2018 - Ajslp 18 0150aninda F.RNo ratings yet
- DegluciónDocument9 pagesDegluciónNatalia Alfaro PetzoldNo ratings yet
- Tugas Ipg UlfaDocument8 pagesTugas Ipg UlfaUlfa Mukhlisa Putri UlfaNo ratings yet
- Detection of Respiratory Syncytial Virus and Rhinovirus in Healthy InfantsDocument5 pagesDetection of Respiratory Syncytial Virus and Rhinovirus in Healthy Infants8502474No ratings yet
- Acute Respiratory Infection Case Definitions For Young Children, A Systematic Review of Community-Based Epidemiologic Studies in South Asia 2012Document14 pagesAcute Respiratory Infection Case Definitions For Young Children, A Systematic Review of Community-Based Epidemiologic Studies in South Asia 2012amyNo ratings yet
- International Journal of Infectious Diseases: Clinical Features and Outcome of Acute Otitis Media in Early InfancyDocument6 pagesInternational Journal of Infectious Diseases: Clinical Features and Outcome of Acute Otitis Media in Early InfancyNana HeriyanaNo ratings yet
- Reference Ranges For Spirometry Across All Ages: A New ApproachDocument8 pagesReference Ranges For Spirometry Across All Ages: A New Approachmossad elevenNo ratings yet
- The Relationship Between Otitis Media With Effusion and Gastroesophageal Reflux Disease: A Meta-AnalysisDocument9 pagesThe Relationship Between Otitis Media With Effusion and Gastroesophageal Reflux Disease: A Meta-Analysisputri balqisNo ratings yet
- CDC 86099 DS1Document20 pagesCDC 86099 DS1klinik kf 275No ratings yet
- Factor Analysis of The Pediatric Symptom Checklist in A Population of Children With Voiding Dysfunction And/or Nocturnal EnuresisDocument9 pagesFactor Analysis of The Pediatric Symptom Checklist in A Population of Children With Voiding Dysfunction And/or Nocturnal EnuresisCris RodriguesNo ratings yet
- Study Effectiveness of Nebulization Improving Childrens Respiratory Status Nursing EssayDocument2 pagesStudy Effectiveness of Nebulization Improving Childrens Respiratory Status Nursing EssayNavinYattiNo ratings yet
- Prevalence of Tourette Syndrome and Chronic Tics I PDFDocument16 pagesPrevalence of Tourette Syndrome and Chronic Tics I PDFFitriazneNo ratings yet
- Nej M 200104193441601Document9 pagesNej M 200104193441601Tri Rahma Yani YawatiNo ratings yet
- PSIHOLOGIEDocument15 pagesPSIHOLOGIEMihaela IftodeNo ratings yet
- PARENTAL KNOWLEDGE ATTITUDES AND PRACTICES KAPs ONpDocument6 pagesPARENTAL KNOWLEDGE ATTITUDES AND PRACTICES KAPs ONpBerliana SitanggangNo ratings yet
- Pediatric Dentistry Aom Pacifier 2001Document5 pagesPediatric Dentistry Aom Pacifier 2001Kobayashi MaruNo ratings yet
- JCDR 10 LC08Document6 pagesJCDR 10 LC08kurniawan martNo ratings yet
- Laryngomalacia and Swallowing Function in ChildrenDocument7 pagesLaryngomalacia and Swallowing Function in ChildrenmelaniaNo ratings yet
- Tumor AbdomenDocument5 pagesTumor Abdomentriska antonyNo ratings yet
- 2021 Predictors of Lung Function Trajectories in Population-Based Studies A Systematic ReviewDocument22 pages2021 Predictors of Lung Function Trajectories in Population-Based Studies A Systematic Reviewjose.maletNo ratings yet
- Brockmann2012 Article PrimarySnoringInSchoolChildrenDocument7 pagesBrockmann2012 Article PrimarySnoringInSchoolChildrenAnonymous GbqNxHcNo ratings yet
- 05 38719Document17 pages05 38719Hafsatul husniNo ratings yet
- Hoarseness of VoiceDocument6 pagesHoarseness of VoiceJayantiNo ratings yet
- Dentofacial Characteristics of Oral Breathers in Different AgesDocument10 pagesDentofacial Characteristics of Oral Breathers in Different AgesAlejandro RuizNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 2: RespiratoryFrom EverandComplementary and Alternative Medical Lab Testing Part 2: RespiratoryNo ratings yet
- Phone ContractDocument2 pagesPhone ContractJaron KungNo ratings yet
- Share Contemporary Issues Project by Nisha VyasDocument41 pagesShare Contemporary Issues Project by Nisha VyasNisha vyasNo ratings yet
- Untitled Design PDFDocument14 pagesUntitled Design PDFRizka BelindaNo ratings yet
- Security Policy 6 E CommerceDocument6 pagesSecurity Policy 6 E CommerceShikha MehtaNo ratings yet
- D 1510 PDFDocument9 pagesD 1510 PDFDark57100% (1)
- IMO Shortlist 2010Document72 pagesIMO Shortlist 2010Florina TomaNo ratings yet
- Galle Four GravetsDocument1 pageGalle Four GravetsRavindra KumaraNo ratings yet
- Flashcards - Topic 7 Human Nutrition - CAIE Biology IGCSEDocument153 pagesFlashcards - Topic 7 Human Nutrition - CAIE Biology IGCSESamiullah TahirNo ratings yet
- Uwb AntennasDocument4 pagesUwb AntennasvutrangdtNo ratings yet
- Rudaga - Regulations - 2021Document7 pagesRudaga - Regulations - 2021sidharthNo ratings yet
- Module 2-Corporate Governance PDFDocument5 pagesModule 2-Corporate Governance PDFBhosx KimNo ratings yet
- Elk Consumer MathDocument7 pagesElk Consumer Mathapi-399013722No ratings yet
- Nej Mo A 2307563Document12 pagesNej Mo A 2307563Sussette SánchezNo ratings yet
- Equipment Testing LABDocument17 pagesEquipment Testing LABTamrat HailuNo ratings yet
- BRM Lecture4Document12 pagesBRM Lecture4amrj27609No ratings yet
- The Iron TradeDocument7 pagesThe Iron TradeEnock BarasaNo ratings yet
- Yom Ha'atzmaut Missing Letters: Fill in The Missing Letters To Complete The WordsDocument34 pagesYom Ha'atzmaut Missing Letters: Fill in The Missing Letters To Complete The WordsRachel MalagaNo ratings yet
- History of WirelessDocument7 pagesHistory of WirelessHarshaNo ratings yet
- Probability CheatsheetDocument10 pagesProbability Cheatsheetprash27kNo ratings yet
- CXC - Csec - Electrical Electronnics - Sba Booklet 2010Document38 pagesCXC - Csec - Electrical Electronnics - Sba Booklet 2010api-255989257No ratings yet
- Generalitat de Catalunya Departament D'educació Institut Eduard Fontseré Biology and Geology 1st First TermDocument22 pagesGeneralitat de Catalunya Departament D'educació Institut Eduard Fontseré Biology and Geology 1st First TermJosé Javier Carreto PascuaNo ratings yet
- History of Global Market IntegrationDocument3 pagesHistory of Global Market IntegrationsoringgamNo ratings yet
- 5 POWER HERBS and HERB BENEFITSDocument4 pages5 POWER HERBS and HERB BENEFITSheartmusic20No ratings yet
- Mosquito RepellentDocument11 pagesMosquito RepellentAkhil RajanNo ratings yet
- DLL-first-quarter Sci10Document4 pagesDLL-first-quarter Sci10Danilo Balbas, Jr.100% (1)
- Antepartum Fetal MonitoringDocument4 pagesAntepartum Fetal MonitoringChristoperJ.ErecreNo ratings yet
- Approved Steel FabricatorsDocument23 pagesApproved Steel FabricatorsMd TahreemNo ratings yet
- ResumeDocument2 pagesResumeapi-302153180No ratings yet
- Vintage Poster Lenormand 2013Document25 pagesVintage Poster Lenormand 2013Magdalena Sighild Petersson100% (2)