Download as pdf or txt
You might also like
- Letter - Closure of BusinessDocument1 pageLetter - Closure of BusinessB-an Javelosa91% (35)
- What Is Decarbonization ?: Main Engine Decarb Preparation, Procedure & Commissioning Sumit NarayanDocument3 pagesWhat Is Decarbonization ?: Main Engine Decarb Preparation, Procedure & Commissioning Sumit NarayanManisha100% (1)
- 1 s2.0 S2215036623001992Document13 pages1 s2.0 S2215036623001992Jorge SalazarNo ratings yet
- 2021 Grupo 1 Metanálise AntidepressivosDocument14 pages2021 Grupo 1 Metanálise AntidepressivosAmanda NelvoNo ratings yet
- Zhou 2020Document8 pagesZhou 2020Rosalía PattyNo ratings yet
- E Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisDocument10 pagesE Cacy of Modern Antipsychotics in Placebo-Controlled Trials in Bipolar Depression: A Meta-AnalysisRisda AprilianiNo ratings yet
- Incidence of Antidepressant Discontinuation SymptomsDocument10 pagesIncidence of Antidepressant Discontinuation SymptomsMarcNo ratings yet
- Mental Health Disorders and Addictions (DD)Document10 pagesMental Health Disorders and Addictions (DD)BalmaNo ratings yet
- Huhn Et Al. Efficacy of Pharmacotherapy and Psychotherapy For Adult Psychiatric DisordersDocument10 pagesHuhn Et Al. Efficacy of Pharmacotherapy and Psychotherapy For Adult Psychiatric DisordersNatalia López MedinaNo ratings yet
- Comparison of Nefazodone, The Cog Behav Sys of Psychotherapy TX DepressionDocument9 pagesComparison of Nefazodone, The Cog Behav Sys of Psychotherapy TX DepressionCarolina BerríosNo ratings yet
- Effectiveness of Videoconference-Delivered Cognitive Behavioral Therapy For Adults With Psychiatric Disorders: Systematic and Meta-Analytic ReviewDocument16 pagesEffectiveness of Videoconference-Delivered Cognitive Behavioral Therapy For Adults With Psychiatric Disorders: Systematic and Meta-Analytic ReviewlaiaNo ratings yet
- Clinician Guidelines For The Treatment of Psychiatric Disorders With Nutraceuticals and Phytoceuticals The World Federation of Societies of BiologicaDocument34 pagesClinician Guidelines For The Treatment of Psychiatric Disorders With Nutraceuticals and Phytoceuticals The World Federation of Societies of Biologicapatrick.arnonNo ratings yet
- Evaluation of Anti-Psychotics Prescribing Pattern Using Who Indicators in A Tertiary Care HospitalDocument14 pagesEvaluation of Anti-Psychotics Prescribing Pattern Using Who Indicators in A Tertiary Care HospitalInternational Journal of Innovative Science and Research Technology100% (1)
- Krist On 2014Document10 pagesKrist On 2014John DoeNo ratings yet
- 1 s2.0 S0165032723006389 MainDocument11 pages1 s2.0 S0165032723006389 MainIoana CoseruNo ratings yet
- Adjunctive Psychotherapy For Bipolar DisorderDocument10 pagesAdjunctive Psychotherapy For Bipolar DisorderAgustin NunezNo ratings yet
- Psychiatry2018 5183834Document6 pagesPsychiatry2018 5183834Bagus Abdillah WinataNo ratings yet
- Psychopharmacological Treatment in BorderlineDocument8 pagesPsychopharmacological Treatment in BorderlineAndres MartinezNo ratings yet
- Treatment of Anxiety Disorders by Psychiatrists From The American Psychiatric Practice Research NetworkDocument6 pagesTreatment of Anxiety Disorders by Psychiatrists From The American Psychiatric Practice Research NetworkStephNo ratings yet
- Mapping The Psychoanalytic Literature On Bipolar DisorderDocument13 pagesMapping The Psychoanalytic Literature On Bipolar DisorderYeliNo ratings yet
- Cannabidiol en PsicosisDocument10 pagesCannabidiol en PsicosissiralkNo ratings yet
- Comparative e Cacy and Acceptability of Antimanic Drugs in Acute Mania: A Multiple-Treatments Meta-AnalysisDocument10 pagesComparative e Cacy and Acceptability of Antimanic Drugs in Acute Mania: A Multiple-Treatments Meta-AnalysisCarolina PradoNo ratings yet
- Psychedelic-Assisted Psychotherapy: A Paradigm Shift in Psychiatric Research and DevelopmentDocument11 pagesPsychedelic-Assisted Psychotherapy: A Paradigm Shift in Psychiatric Research and DevelopmentIago LôboNo ratings yet
- Psychedelic-Assisted Psychotherapy - A Paradigm Shift in Psychiatric Research and DevelopmentDocument11 pagesPsychedelic-Assisted Psychotherapy - A Paradigm Shift in Psychiatric Research and DevelopmentmsrappNo ratings yet
- Journal of Affective Disorders en 2010Document8 pagesJournal of Affective Disorders en 2010Valentina Erazo.No ratings yet
- WFBSP SZ Guidelines Part1 2012 Acute SchizophreniaDocument61 pagesWFBSP SZ Guidelines Part1 2012 Acute Schizophreniascabrera_scribdNo ratings yet
- Schizophrenia Stigma in Mental Health Professionals and Associated Factors A Systematic ReviewDocument1 pageSchizophrenia Stigma in Mental Health Professionals and Associated Factors A Systematic ReviewFrida Ximena Perez CaballeroNo ratings yet
- Cuijpers Karyotaki 2021Document6 pagesCuijpers Karyotaki 2021Juliana AlvesNo ratings yet
- Anxious and Non Anxious Major Depression WorldwideDocument28 pagesAnxious and Non Anxious Major Depression WorldwideMariaAn DominguezNo ratings yet
- Reviewing Depot Injection Efficacy in The Treatment of SchizophreniaDocument10 pagesReviewing Depot Injection Efficacy in The Treatment of SchizophreniaAnonymous raLgWVyqNo ratings yet
- Panss ScoreDocument8 pagesPanss ScoretriaclaresiaNo ratings yet
- 2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesDocument16 pages2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesMarcos MouraNo ratings yet
- Schizophrenia Research: Markku Lähteenvuo, Heidi Taipale, Antti Tanskanen, Ellenor Mittendorfer-Rutz, Jari TiihonenDocument6 pagesSchizophrenia Research: Markku Lähteenvuo, Heidi Taipale, Antti Tanskanen, Ellenor Mittendorfer-Rutz, Jari TiihonenIndrajatiNo ratings yet
- 10 1016@j Jpsychires 2020 01 017Document9 pages10 1016@j Jpsychires 2020 01 017Arthur AlbertNo ratings yet
- Challenge and Prospect of Traditional Chinese MedicineDocument15 pagesChallenge and Prospect of Traditional Chinese MedicineLaura Rebeca Silva CNo ratings yet
- Background: Lancet Psychiatry 2017Document11 pagesBackground: Lancet Psychiatry 2017Manya DhuparNo ratings yet
- Group Treatment For Substance Use Disorder in Adults: A Systematic Review and Meta-Analysis of Randomized-Controlled TrialsDocument14 pagesGroup Treatment For Substance Use Disorder in Adults: A Systematic Review and Meta-Analysis of Randomized-Controlled TrialsCîmpeanu MădălinaNo ratings yet
- Pi Is 2215036616303789Document11 pagesPi Is 2215036616303789U of T MedicineNo ratings yet
- We Therell 2009Document10 pagesWe Therell 2009Oslo SaputraNo ratings yet
- Realworld Effectiveness of Pharmacological Treatments For Bipolar Disorder Registerbased National Cohort StudyDocument9 pagesRealworld Effectiveness of Pharmacological Treatments For Bipolar Disorder Registerbased National Cohort StudyJose BusaidNo ratings yet
- Provisional: Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment OptionsDocument73 pagesProvisional: Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment OptionsDewi NofiantiNo ratings yet
- Initial Severity Jama PDFDocument8 pagesInitial Severity Jama PDFnoeanisaNo ratings yet
- Initial Severity of Schizophrenia and Efficacy of Antipsychotics Participant-Level Meta-Analysis of 6 Placebo-Controlled StudiesDocument8 pagesInitial Severity of Schizophrenia and Efficacy of Antipsychotics Participant-Level Meta-Analysis of 6 Placebo-Controlled StudieseviantiNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundPsiquiatría CESAMENo ratings yet
- Penyuluhan CemasDocument7 pagesPenyuluhan CemasVeronica Yosita AnandaNo ratings yet
- TTO - EZF BR Fpsyt 13 859042Document26 pagesTTO - EZF BR Fpsyt 13 859042Eliana RieraNo ratings yet
- Sequential Combination of Pharmacotherapy and Psychotherapy in Major Depressive Disorder A Systematic Review and Meta-AnalysisDocument9 pagesSequential Combination of Pharmacotherapy and Psychotherapy in Major Depressive Disorder A Systematic Review and Meta-AnalysisDaniela SerbanNo ratings yet
- Psicofármacos y VIHDocument8 pagesPsicofármacos y VIHANDREA MATAMOROSNo ratings yet
- Patterns and Frequency of Atypical Antipsychotic Prescribing in Psychiatric Medical Centers: A Cross-Sectional National SurveyDocument9 pagesPatterns and Frequency of Atypical Antipsychotic Prescribing in Psychiatric Medical Centers: A Cross-Sectional National Surveymiron_ghiuNo ratings yet
- Raglio 2015 Effects of Music and Music Therapy On Mood in Neurological Patients PDFDocument12 pagesRaglio 2015 Effects of Music and Music Therapy On Mood in Neurological Patients PDFsimaso0% (1)
- Behavior TherapyDocument29 pagesBehavior TherapyKrisztina MkNo ratings yet
- Fusar Poli2016Document10 pagesFusar Poli2016Felipe VergaraNo ratings yet
- Fpsyt 11 600283Document3 pagesFpsyt 11 600283Daniel Pérez-RuizNo ratings yet
- Cuijpers Et Al., (2021)Document11 pagesCuijpers Et Al., (2021)Jonathan PitreNo ratings yet
- Jurnal DepresiDocument4 pagesJurnal DepresiBagus Ridho SetiadiNo ratings yet
- Psychosomatics and MentalizationDocument1 pagePsychosomatics and MentalizationBoyko TsenkovNo ratings yet
- Psic EdDocument27 pagesPsic EdNicolás Robertino LombardiNo ratings yet
- The Acute Efficacy of Antipsychotics in Schizophrenia: A Review of Recent Meta-AnalysesDocument16 pagesThe Acute Efficacy of Antipsychotics in Schizophrenia: A Review of Recent Meta-AnalysesrezkiwjNo ratings yet
- Bipolar 2Document5 pagesBipolar 2Kenny KenNo ratings yet
- Example 2Document5 pagesExample 2Сергей СтанишевNo ratings yet
- Real World Effectiveness of Pharmacological Treatments For Bipolar Disorder Register Based National Cohort StudyDocument9 pagesReal World Effectiveness of Pharmacological Treatments For Bipolar Disorder Register Based National Cohort StudySusana Pérez ReyesNo ratings yet
- Dimensional PsychopathologyFrom EverandDimensional PsychopathologyMassimo BiondiNo ratings yet
- A Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Document10 pagesA Clinical Pathway To Standardize Care of Children With Delirium in Pediatric Inpatient Settings-2019Juan ParedesNo ratings yet
- Valproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Document7 pagesValproate For Agitation in Critically Ill Patients - A Retrospective Study-2017Juan ParedesNo ratings yet
- The Balint Group and Its Application in Medical Education - A Systematic Review - 2019Document7 pagesThe Balint Group and Its Application in Medical Education - A Systematic Review - 2019Juan ParedesNo ratings yet
- Pediatric Delirium - Recognition, Management, and Outcome-2017Document7 pagesPediatric Delirium - Recognition, Management, and Outcome-2017Juan ParedesNo ratings yet
- Case 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Document10 pagesCase 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Juan ParedesNo ratings yet
- Analgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Document10 pagesAnalgesia, Sedation, and Delirium in Pediatric Surgical Critical Care-2019Juan ParedesNo ratings yet
- Alcohol and Other Substance Use Among Medical and Law Students at A UK University - A Cross-Sectional Questionnaire Survey-2017Document6 pagesAlcohol and Other Substance Use Among Medical and Law Students at A UK University - A Cross-Sectional Questionnaire Survey-2017Juan ParedesNo ratings yet
- Iatrogenic Opioid Withdrawal in Critically Ill Patients - A Review of Assessment Tools and Management-2017Document13 pagesIatrogenic Opioid Withdrawal in Critically Ill Patients - A Review of Assessment Tools and Management-2017Juan Paredes100% (1)
- Correlations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Document9 pagesCorrelations Between Brain Changes and Pain Management After Cognitive and Meditative Therapies - A Systematic Review of Neuroimaging Studies-2018Juan ParedesNo ratings yet
- Temporal Biomarker Profiles and Their Association With ICU Acquired Delirium - A Cohort Study-2018Document10 pagesTemporal Biomarker Profiles and Their Association With ICU Acquired Delirium - A Cohort Study-2018Juan ParedesNo ratings yet
- Suicide Risk in Chronic Heart Failure Patients and Its Association With Depression, Hopelessness and Self Esteem-2019Document4 pagesSuicide Risk in Chronic Heart Failure Patients and Its Association With Depression, Hopelessness and Self Esteem-2019Juan ParedesNo ratings yet
- Differentiation of Delirium, Dementia and Delirium Superimposed On Dementia in The Older Person-2018Document5 pagesDifferentiation of Delirium, Dementia and Delirium Superimposed On Dementia in The Older Person-2018Juan Paredes100% (1)
- Efficacy of Problem Solving Therapy For Spouses of Men With Prostate Cancer - A Randomized Controlled Trial-2018Document9 pagesEfficacy of Problem Solving Therapy For Spouses of Men With Prostate Cancer - A Randomized Controlled Trial-2018Juan ParedesNo ratings yet
- Key Updates in The Clinical Application of Electroconvulsive Therapy-2017Document10 pagesKey Updates in The Clinical Application of Electroconvulsive Therapy-2017Juan ParedesNo ratings yet
- Consultation-Liaison Psychiatry - How Far Have We Come - 2006Document8 pagesConsultation-Liaison Psychiatry - How Far Have We Come - 2006Juan ParedesNo ratings yet
- Delirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Document7 pagesDelirium in Elderly Patients - Prospective Prevalence Across Hospital Services-2020Juan ParedesNo ratings yet
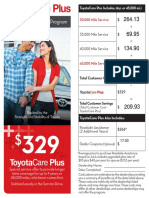
- ToyotaCare Plus CalculationDocument2 pagesToyotaCare Plus CalculationShao MaNo ratings yet
- Bomba 750 GPM 130 McaDocument1 pageBomba 750 GPM 130 McaEDWIN HUMBERTO QUICENO CANONo ratings yet
- What Is Total Quality ManagementDocument4 pagesWhat Is Total Quality ManagementJayson Villena MalimataNo ratings yet
- Food & Beverage Service Operation: Prepared By: Mr. Lance MercadoDocument22 pagesFood & Beverage Service Operation: Prepared By: Mr. Lance MercadoLyzelNo ratings yet
- Group 1 Dorb001 Bsce3aDocument16 pagesGroup 1 Dorb001 Bsce3aJan TheGamerNo ratings yet
- PHREEQ C Modelling Tool Application To Determine The Effect of Anions On Speciation of Selected Metals in Water Systems Within Kajiado North Constituency in KenyaDocument71 pagesPHREEQ C Modelling Tool Application To Determine The Effect of Anions On Speciation of Selected Metals in Water Systems Within Kajiado North Constituency in KenyaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Wizard - School of DiabolismDocument1 pageWizard - School of DiabolismHope LaneNo ratings yet
- Deif SynchronizersDocument4 pagesDeif SynchronizerssdiamanNo ratings yet
- Free Bhel Transformer Book PDFDocument4 pagesFree Bhel Transformer Book PDFMilan ShahNo ratings yet
- Activity - 2 - (Discretel) (A1)Document1 pageActivity - 2 - (Discretel) (A1)AnkitChutaniNo ratings yet
- Imj 13707Document11 pagesImj 13707Santiago López JosueNo ratings yet
- Yi PDFDocument2 pagesYi PDFAnonymous La5rPMYNo ratings yet
- (20635303 - Journal of Behavioral Addictions) Fear of Missing Out (FoMO) and Internet Use - A Comprehensive Systematic Review and Meta-AnalysisDocument22 pages(20635303 - Journal of Behavioral Addictions) Fear of Missing Out (FoMO) and Internet Use - A Comprehensive Systematic Review and Meta-AnalysisNeeraj raiNo ratings yet
- Transition Guide-Leadership Team Simulation Everest v3Document7 pagesTransition Guide-Leadership Team Simulation Everest v3Mariana A SecasNo ratings yet
- Braintree 15Document6 pagesBraintree 15paypaltrexNo ratings yet
- Interfacing Seven Segment Display To 8051Document16 pagesInterfacing Seven Segment Display To 8051Virang PatelNo ratings yet
- HTWL Service Manual: Failure ListDocument2 pagesHTWL Service Manual: Failure ListClaudio Valencia MarínNo ratings yet
- Blake Problem ComputationDocument3 pagesBlake Problem ComputationNiño del Mundo75% (4)
- Talent Acquisition 2008 - Survey and Analysis of The Changing Recruiting Landscape PDFDocument20 pagesTalent Acquisition 2008 - Survey and Analysis of The Changing Recruiting Landscape PDFVaishnavi SivaNo ratings yet
- Ubuntu FeistyDocument242 pagesUbuntu FeistySlamet Budi SantosoNo ratings yet
- XProtect Expert Product SheetDocument2 pagesXProtect Expert Product SheetKrishna GhimireNo ratings yet
- BTX - Parts Manual 834H Vol II Feb 2010Document871 pagesBTX - Parts Manual 834H Vol II Feb 2010maneul zambranoNo ratings yet
- Cost Justifying HRIS InvestmentsDocument19 pagesCost Justifying HRIS InvestmentsJessierene ManceraNo ratings yet
- Pregnancy-Related Pelvic Girdle Pain: Second Stage of LabourDocument4 pagesPregnancy-Related Pelvic Girdle Pain: Second Stage of LabourSravan Ganji100% (1)
- 3 2 A UnitconversionDocument6 pages3 2 A Unitconversionapi-312626334No ratings yet
- Yealink Phone UserGuide PDFDocument2 pagesYealink Phone UserGuide PDFEric SmithNo ratings yet
- Human Resources Management in 2020.Document11 pagesHuman Resources Management in 2020.DheerajNo ratings yet
- 3GPP TS 22.278Document51 pages3GPP TS 22.278bhushan7408No ratings yet