Download as pdf or txt
You might also like
- Avoiding Common Errors in The Emergency Department-801-1002Document200 pagesAvoiding Common Errors in The Emergency Department-801-1002Hernando CastrillónNo ratings yet
- Va Inspector Report 3Document100 pagesVa Inspector Report 3Jeff MorrisNo ratings yet
- Empty Sella SyndromeDocument21 pagesEmpty Sella SyndromeMohamed TarekNo ratings yet
- Cornell A 2003Document13 pagesCornell A 2003dnazaryNo ratings yet
- Cerebral Venous ThrombosisDocument15 pagesCerebral Venous ThrombosisValentina RobuNo ratings yet
- Abses Serebri2 PDFDocument22 pagesAbses Serebri2 PDFRagillia Irena FebriNo ratings yet
- Hydrocephalus in Canine and Feline PatientsDocument4 pagesHydrocephalus in Canine and Feline PatientsWeiwei CierraNo ratings yet
- Craniosynostosis in Growing Children 2016Document7 pagesCraniosynostosis in Growing Children 2016Miguel AcunaNo ratings yet
- Davis 2003Document9 pagesDavis 2003Apotik ApotekNo ratings yet
- Treatment of Hydrocephalus: Mere Survival Is Not EnoughDocument7 pagesTreatment of Hydrocephalus: Mere Survival Is Not EnoughdnazaryNo ratings yet
- 125-Article Text-375-1-10-20180214 PDFDocument5 pages125-Article Text-375-1-10-20180214 PDFsivadeavNo ratings yet
- 2021 - Apnea Central Del Sueño @ishikawaDocument13 pages2021 - Apnea Central Del Sueño @ishikawaJorge Toshio Yazawa ChaconNo ratings yet
- Cerebral Venous Sinus ThrombosisDocument11 pagesCerebral Venous Sinus ThrombosisdjcafNo ratings yet
- Calcific Neurocysticercosis and EpileptogenesisDocument7 pagesCalcific Neurocysticercosis and EpileptogenesiskreizztelNo ratings yet
- Obstructive Sleep Apnea Syndrome: Diagnosis and Management: A B S T R A C TDocument13 pagesObstructive Sleep Apnea Syndrome: Diagnosis and Management: A B S T R A C Tsafwand90No ratings yet
- Hydrocephalus FsDocument16 pagesHydrocephalus FsYos AkbarNo ratings yet
- Legg Calve Perthes PDFDocument14 pagesLegg Calve Perthes PDFEalsa CTNo ratings yet
- Cerebral Venous ThrombosisDocument19 pagesCerebral Venous ThrombosisgresiaNo ratings yet
- SWS 1 PDFDocument6 pagesSWS 1 PDFdzhzrnNo ratings yet
- Congestion Pelvica 2020Document6 pagesCongestion Pelvica 2020Cristian RodríguezNo ratings yet
- CSCR MedscapeDocument13 pagesCSCR MedscapeFelix Valerian HalimNo ratings yet
- Apik Case of The Month 09-2012Document9 pagesApik Case of The Month 09-2012Naily Nuzulur RohmahNo ratings yet
- Case Pres - HydrocephalusDocument26 pagesCase Pres - HydrocephalusJack Bisarra Sanchez100% (1)
- Hydrocephalus 2Document14 pagesHydrocephalus 2ashley11No ratings yet
- 121 Anaesthesia For VP Shunt InsertionDocument8 pages121 Anaesthesia For VP Shunt InsertionMohammed ElSayedNo ratings yet
- Accepted Manuscript: SeizureDocument21 pagesAccepted Manuscript: SeizureAhmad Harissul IbadNo ratings yet
- Central Serous Chorioretinopathy Induced by Work Stress (BACA UMUM)Document15 pagesCentral Serous Chorioretinopathy Induced by Work Stress (BACA UMUM)Vincent Rooroh0% (1)
- Clinical Features, Diagnosis, and Treatment of Neonatal EncephalopathyDocument15 pagesClinical Features, Diagnosis, and Treatment of Neonatal EncephalopathyAlvaro SagredoNo ratings yet
- Hydrocephalus & ShuntsDocument9 pagesHydrocephalus & ShuntsVaseem ZamairNo ratings yet
- Antenatal Diagnosis ofDocument6 pagesAntenatal Diagnosis ofnskhldNo ratings yet
- Hydro Cep Hal UsDocument5 pagesHydro Cep Hal UsEka Putra PrayogaNo ratings yet
- SC Compression, Neurol Clinics, 2-03Document20 pagesSC Compression, Neurol Clinics, 2-03Jaime H. Soto LugoNo ratings yet
- Now You See It, Case ReportDocument6 pagesNow You See It, Case ReportPhilip McNelsonNo ratings yet
- Intracranial Arachnoid Cysts - Do They Impair Mental Functions?Document8 pagesIntracranial Arachnoid Cysts - Do They Impair Mental Functions?CYNTHIA TORRES GONZALEZNo ratings yet
- Euro J of Neurology - 2002 - Scolding - The Recognition Diagnosis and Management of Cerebral Vasculitis A European SurveyDocument5 pagesEuro J of Neurology - 2002 - Scolding - The Recognition Diagnosis and Management of Cerebral Vasculitis A European SurveyAlin CiubotaruNo ratings yet
- Cauda Equina Syndrome: A Simple Entity With Lot of Enigma!: EditorialDocument3 pagesCauda Equina Syndrome: A Simple Entity With Lot of Enigma!: EditorialsalikaabrarNo ratings yet
- Fast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaFrom EverandFast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaNo ratings yet
- Ocular Auscultation: A ReviewDocument5 pagesOcular Auscultation: A ReviewMihnea GamanNo ratings yet
- Traumatic CSF LeaksDocument17 pagesTraumatic CSF LeaksNada AhmedNo ratings yet
- Hydrocephalus Lesson Plan NewDocument18 pagesHydrocephalus Lesson Plan NewUday Kumar100% (2)
- 1 s2.0 S1548559521000331 MainDocument10 pages1 s2.0 S1548559521000331 MainAchrafNo ratings yet
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- EXPOSEEDocument9 pagesEXPOSEEMind BlowerNo ratings yet
- HYDROCEPHALUSDocument47 pagesHYDROCEPHALUSMichelle DuNo ratings yet
- SAHOS y AnestesiaDocument10 pagesSAHOS y AnestesiaEzequielNo ratings yet
- 3.the Efficient Dizziness History and ExamDocument12 pages3.the Efficient Dizziness History and ExamCribea AdmNo ratings yet
- A 19-Year-Old Man With Sickle Cell Disease Presenting With Spinal Infarction: A Case ReportDocument6 pagesA 19-Year-Old Man With Sickle Cell Disease Presenting With Spinal Infarction: A Case ReportJabber PaudacNo ratings yet
- Review of The Treatment & Management of Hydrocephalus: Jacqueline Groat, Pharmd CandidateDocument9 pagesReview of The Treatment & Management of Hydrocephalus: Jacqueline Groat, Pharmd CandidateAsif KhanNo ratings yet
- Berg Sneider 2008Document18 pagesBerg Sneider 2008dnazaryNo ratings yet
- Pulmonary Fibrosis in Sytemic Sclerosis Diagnosis and ManagementDocument5 pagesPulmonary Fibrosis in Sytemic Sclerosis Diagnosis and ManagementAnthoNo ratings yet
- Carotid SinusDocument20 pagesCarotid SinusPratyush PrateekNo ratings yet
- Cauda Equina SyndromeDocument35 pagesCauda Equina SyndromeVamsi MohanNo ratings yet
- Bahan Hidrosefalus2Document17 pagesBahan Hidrosefalus2Arry Wijaya LieNo ratings yet
- Cervical SpondylosisDocument15 pagesCervical Spondylosistaru_airiqu5741No ratings yet
- Cerebral PalsyDocument10 pagesCerebral PalsytipharethtNo ratings yet
- Basic NewerDocument9 pagesBasic Newerblack smithNo ratings yet
- State of The Art: Epidemiology of Obstructive Sleep ApneaDocument23 pagesState of The Art: Epidemiology of Obstructive Sleep ApneaMelly NoviaNo ratings yet
- Cauda Equina Syndrome: LSUHSC Neuroscience Student ClerkshipDocument32 pagesCauda Equina Syndrome: LSUHSC Neuroscience Student ClerkshipraraNo ratings yet
- Cardiorenal Syndrome in Heart FailureFrom EverandCardiorenal Syndrome in Heart FailureW. H. Wilson TangNo ratings yet
- 259 605 1 PBDocument8 pages259 605 1 PBn2763288No ratings yet
- Pre-Pregnancy Menstrual Cycle Regularity and Length and The Risk of Gestational Diabetes Mellitus: Prospective Cohort StudyDocument10 pagesPre-Pregnancy Menstrual Cycle Regularity and Length and The Risk of Gestational Diabetes Mellitus: Prospective Cohort Studyn2763288No ratings yet
- Cochrane: LibraryDocument15 pagesCochrane: Libraryn2763288No ratings yet
- A Brief Summary of Current Evidence of Studies Regarding The Preventive and Therapeutic Effects of Isoflavones and SoyfoodsDocument2 pagesA Brief Summary of Current Evidence of Studies Regarding The Preventive and Therapeutic Effects of Isoflavones and Soyfoodsn2763288No ratings yet
- Recurrent Implantation Failure-Update Overview OnDocument19 pagesRecurrent Implantation Failure-Update Overview Onn2763288100% (1)
- Ldac 007Document11 pagesLdac 007n2763288No ratings yet
- Vaginal Birth After SCDocument5 pagesVaginal Birth After SCn2763288No ratings yet
- E031193 FullDocument9 pagesE031193 Fulln2763288No ratings yet
- Did9z3ct0k0krfmeql0m Signature Poli 180218060814Document23 pagesDid9z3ct0k0krfmeql0m Signature Poli 180218060814n2763288No ratings yet
- Heinzelmann Schwarz2018Document7 pagesHeinzelmann Schwarz2018n2763288No ratings yet
- FulltextDocument12 pagesFulltextn2763288No ratings yet
- Clinical Endocrinology - 2021 - Barber - Obesity and Polycystic Ovary SyndromeDocument11 pagesClinical Endocrinology - 2021 - Barber - Obesity and Polycystic Ovary Syndromen2763288No ratings yet
- 1267555706Document40 pages1267555706n2763288No ratings yet
- Pengaruh Pemberian Aromaterapi Jahe Terh 2Document7 pagesPengaruh Pemberian Aromaterapi Jahe Terh 2Lastri Khairin100% (1)
- Table of Comparison On Cardiopulmonary Resuscitation For Adul1Document1 pageTable of Comparison On Cardiopulmonary Resuscitation For Adul1Luigi GeduqueNo ratings yet
- Diaphragm Lecture 1Document2 pagesDiaphragm Lecture 1Unspe XiNo ratings yet
- Cadiovascular DiseasesDocument12 pagesCadiovascular Diseasestam meiNo ratings yet
- Craniocerebral TraumaDocument64 pagesCraniocerebral TraumaBentoys StreetNo ratings yet
- Blood Test and Normal RangeDocument40 pagesBlood Test and Normal Rangeethirukumaran50% (2)
- What Is Cardiac AblationDocument2 pagesWhat Is Cardiac AblationShay Patrick CormacNo ratings yet
- National Guideline For Dengue 2018 PDFDocument96 pagesNational Guideline For Dengue 2018 PDFTapash GopeNo ratings yet
- Science 4 Quarter 2 MELC - Based Summative Test #1Document12 pagesScience 4 Quarter 2 MELC - Based Summative Test #1Marie Jaja Tan Roa100% (1)
- Nursing Care PlanDocument2 pagesNursing Care Plankarla joy sta teresaNo ratings yet
- Pemenant Family PlanningDocument6 pagesPemenant Family PlanningKrini TandelNo ratings yet
- Microbiological Quality of Bottled Drinking W A T E R in The Uae and The Effect of Storage at Different TemperaturesDocument5 pagesMicrobiological Quality of Bottled Drinking W A T E R in The Uae and The Effect of Storage at Different TemperaturesUSMANNo ratings yet
- Jover Reflection PaperDocument2 pagesJover Reflection PaperGwen Myles JoverNo ratings yet
- FIIIIIINAAAAALLLLLLDocument132 pagesFIIIIIINAAAAALLLLLLJohn Remy HerbitoNo ratings yet
- Peripheral Arterial Disease: MBCHB Mres MSC Mrcs Afhea PHDDocument6 pagesPeripheral Arterial Disease: MBCHB Mres MSC Mrcs Afhea PHDNelly ElizabethNo ratings yet
- NCP Cord Prolapse Frias Ea Lissandra CDocument2 pagesNCP Cord Prolapse Frias Ea Lissandra CFatima Medriza Duran0% (1)
- Pharmacology - Technology TrendsDocument2 pagesPharmacology - Technology TrendsGiselleNo ratings yet
- Leann Li ResumeDocument2 pagesLeann Li Resumeapi-660140781No ratings yet
- 18 LeybovicDocument8 pages18 LeybovicAlvaro galilea nerinNo ratings yet
- 34 Journal of Periodontology - 2018 - H Mmerle - The Etiology of Hard and Soft Tissue Deficiencies at Dental Implants ADocument13 pages34 Journal of Periodontology - 2018 - H Mmerle - The Etiology of Hard and Soft Tissue Deficiencies at Dental Implants AMax Flores RuizNo ratings yet
- WHO 2018 Health at A Glance Mortality Asia Pac Region OctoberDocument3 pagesWHO 2018 Health at A Glance Mortality Asia Pac Region Octoberbiko97jcjNo ratings yet
- Augmentin Tablet Pi Ipi13 SiDocument11 pagesAugmentin Tablet Pi Ipi13 Siاسد راجNo ratings yet
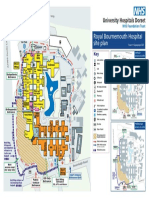
- Royal Bournemouth Hospital Site Plan: A338 Wessex Wa yDocument1 pageRoyal Bournemouth Hospital Site Plan: A338 Wessex Wa ydolar buhaNo ratings yet
- Duke University Department of Medicine Annual Report 2013Document21 pagesDuke University Department of Medicine Annual Report 2013Duke Department of MedicineNo ratings yet
- Transcranial Doppler Ultrasound Examination For Adults and ChildrenDocument12 pagesTranscranial Doppler Ultrasound Examination For Adults and ChildrenJuan José Ruiz CastilloNo ratings yet
- Written - Notes General Survey Vitals Pain 2Document1 pageWritten - Notes General Survey Vitals Pain 2Sheryl LaffertyNo ratings yet
- Clinically Diagnosed Postoperative Venous Thromboembolism in A NeurosurgeryDocument7 pagesClinically Diagnosed Postoperative Venous Thromboembolism in A Neurosurgerydonira73No ratings yet
- Hepatitis A Virus - HAV: DiagnosisDocument6 pagesHepatitis A Virus - HAV: DiagnosisnurmaliarizkyNo ratings yet
- Drug StudyDocument2 pagesDrug StudyAubrey Unique EvangelistaNo ratings yet