Download as pdf or txt
You might also like
- Practical PeriodonticsDocument314 pagesPractical PeriodonticsRazvan Ungureanu100% (1)
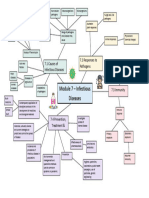
- Module 7 Mind Map BiologyDocument1 pageModule 7 Mind Map BiologyAltSpace TimeNo ratings yet
- Case 16 QuestionsDocument10 pagesCase 16 Questionsapi-532124328No ratings yet
- 4 Adrenal Incidentalomas Review ArticleDocument8 pages4 Adrenal Incidentalomas Review ArticleNguyen Trung TinNo ratings yet
- Standards For Diagnostic RadiologyDocument25 pagesStandards For Diagnostic Radiologymohadese EstajiNo ratings yet
- Euro J of Neurology - 2017 - Ferro - European Stroke Organization Guideline For The Diagnosis and Treatment of CerebralDocument11 pagesEuro J of Neurology - 2017 - Ferro - European Stroke Organization Guideline For The Diagnosis and Treatment of CerebralIvan MihailovicNo ratings yet
- Advantages of Antisense TherapyDocument5 pagesAdvantages of Antisense TherapyRita BhattaNo ratings yet
- Cancer de Prostata Metastasico Sensible y Resistente A La Castracion CANADADocument9 pagesCancer de Prostata Metastasico Sensible y Resistente A La Castracion CANADAurozerpaNo ratings yet
- 24 S Sinha IndiaDocument36 pages24 S Sinha IndiaJadKNo ratings yet
- Role of Nanotech in Cancer TreatmentDocument26 pagesRole of Nanotech in Cancer TreatmentYashi VermaNo ratings yet
- Testicular Cancer JUDocument10 pagesTesticular Cancer JUkarla QuinteroNo ratings yet
- OsteoarthritisDocument82 pagesOsteoarthritisWidi AtmokoNo ratings yet
- Cholangiocarcinoma: The Right Clinical Information, Right Where It's NeededDocument40 pagesCholangiocarcinoma: The Right Clinical Information, Right Where It's NeededHan KethyanethNo ratings yet
- 508 - MAPPP 2017 Presentation-Final 5-12-17Document73 pages508 - MAPPP 2017 Presentation-Final 5-12-17Joanne HoNo ratings yet
- Management of Single Brain Metastasis: A Practice GuidelineDocument13 pagesManagement of Single Brain Metastasis: A Practice GuidelineAndreea IduNo ratings yet
- The Evolution of Radionanotargeting towards Clinical Precision Oncology: A Festschrift in Honor of Kalevi KairemoFrom EverandThe Evolution of Radionanotargeting towards Clinical Precision Oncology: A Festschrift in Honor of Kalevi KairemoNo ratings yet
- Tumor Staging of Endocervical Adenocarcinoma .8Document10 pagesTumor Staging of Endocervical Adenocarcinoma .8elisasitohangNo ratings yet
- Breast Cancer Practice Essentials, Background, AnatomyDocument1 pageBreast Cancer Practice Essentials, Background, AnatomyLim ZXNo ratings yet
- Biomarkers Into The Primary Prostate BiopsyDocument6 pagesBiomarkers Into The Primary Prostate BiopsyCarlos Esteban Gutiérrez CastrejonNo ratings yet
- Fphar 13 750507Document32 pagesFphar 13 750507Lên DươngNo ratings yet
- Mottet2016 PDFDocument12 pagesMottet2016 PDFdipawelloiNo ratings yet
- 1 s2.0 S0167814022044991 MainDocument9 pages1 s2.0 S0167814022044991 MainFeras OskanNo ratings yet
- 2023 10 20 23297314v2 FullDocument99 pages2023 10 20 23297314v2 FullpyjirbfmpektdpprtmNo ratings yet
- Radosevich JA, Aydogan B. Precision Medicine in Oncology. 1st EdDocument282 pagesRadosevich JA, Aydogan B. Precision Medicine in Oncology. 1st EdIhsan NurhadiNo ratings yet
- CA de Ovario GuidelinesDocument14 pagesCA de Ovario GuidelinesNancy Montes ArteagaNo ratings yet
- SNMMI Procedure Standard-EANM Practice Guideline For SSTR PET - Imaging Neuroendocrine TumorsDocument7 pagesSNMMI Procedure Standard-EANM Practice Guideline For SSTR PET - Imaging Neuroendocrine TumorsdynachNo ratings yet
- 1-IsRS Technical Guidelines For StereotacticDocument12 pages1-IsRS Technical Guidelines For Stereotactictaharount.amel20No ratings yet
- 2010 Full Manual ACR ContrastVersion7Document85 pages2010 Full Manual ACR ContrastVersion7Abi SlonimNo ratings yet
- 2022 Biomarkers Metastatic Breast Cancer SlidesDocument29 pages2022 Biomarkers Metastatic Breast Cancer Slideseniale ajonebaNo ratings yet
- Corporate Profile 2021NABLDocument27 pagesCorporate Profile 2021NABLSuraj ChauguleNo ratings yet
- In Vitro and in Vivo Study of The Effect of Osteogenic Pulsed Electromagnetic Fields On Breast and Lung Cancer CellsDocument13 pagesIn Vitro and in Vivo Study of The Effect of Osteogenic Pulsed Electromagnetic Fields On Breast and Lung Cancer CellsVictorNo ratings yet
- Advances in The Field of Nanooncology: Review Open AccessDocument11 pagesAdvances in The Field of Nanooncology: Review Open AccessscrabzNo ratings yet
- Antiemesis, Version 2.2017: NCCN Guidelines InsightsDocument11 pagesAntiemesis, Version 2.2017: NCCN Guidelines Insightswisnu tribagusNo ratings yet
- Biomarker Discovery ThesisDocument7 pagesBiomarker Discovery Thesiskrystalgreenglendale100% (1)
- Impact of Cold Somatostatin Analog Administration On Somatostatin Receptor ImagingDocument7 pagesImpact of Cold Somatostatin Analog Administration On Somatostatin Receptor ImagingUvi Cancino RamosNo ratings yet
- Introduction To Medical TechnologyDocument6 pagesIntroduction To Medical TechnologyMara OcampoNo ratings yet
- White and Pharoahs Oral Radiology Principles Interpretation 8th Edition Ebook PDF VersionDocument62 pagesWhite and Pharoahs Oral Radiology Principles Interpretation 8th Edition Ebook PDF Versionashley.cole177100% (34)
- Clinicopathological and Immunological Profiles of Prostate Adenocarcinoma and Neuroendocrine Prostate CancerDocument9 pagesClinicopathological and Immunological Profiles of Prostate Adenocarcinoma and Neuroendocrine Prostate Cancerفرجني موغNo ratings yet
- European Society of Endocrinology Clinical Practice Guidelines For The Management of Aggressive Pituitary Tumours and CarcinomasDocument24 pagesEuropean Society of Endocrinology Clinical Practice Guidelines For The Management of Aggressive Pituitary Tumours and Carcinomas11-MH-HU-JULIANA VIVAS VEGANo ratings yet
- s00259 022 05780 2Document19 pagess00259 022 05780 2Ionuț RusNo ratings yet
- Clinical Applications of Nuclear Medicine Targeted TherapyFrom EverandClinical Applications of Nuclear Medicine Targeted TherapyEmilio BombardieriNo ratings yet
- CA A Cancer J Clinicians - 2024 - Chauhan - Critical Updates in Neuroendocrine Tumors Version 9 American Joint CommitteeDocument9 pagesCA A Cancer J Clinicians - 2024 - Chauhan - Critical Updates in Neuroendocrine Tumors Version 9 American Joint Committeeguadalupe.cabrera.mdNo ratings yet
- Fmmed 01 749283Document11 pagesFmmed 01 749283Snow wanNo ratings yet
- Prostate Cancer Screening With Prostate-Specific Antigen (PSA) Test A Systematic Review and Meta-AnalysisDocument29 pagesProstate Cancer Screening With Prostate-Specific Antigen (PSA) Test A Systematic Review and Meta-AnalysisLysol CristalNo ratings yet
- Mammaprint™ A Comprehensive ReviewDocument18 pagesMammaprint™ A Comprehensive ReviewAndersson SaenzNo ratings yet
- Reco Prostate 2020 2022Document116 pagesReco Prostate 2020 2022Thomas Husson100% (1)
- Prostate CancerDocument30 pagesProstate CancerMetal GearNo ratings yet
- Ncm106 Course OutlineDocument2 pagesNcm106 Course OutlineRS BuenavistaNo ratings yet
- Diagnosing Gastric Cancer Using A Tri-AlgorithmDocument6 pagesDiagnosing Gastric Cancer Using A Tri-AlgorithmInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Thyroid Cancer Care Collaborative: A Computerized Clinical Decision Support System For Management of Thyroid NodulesDocument22 pagesThyroid Cancer Care Collaborative: A Computerized Clinical Decision Support System For Management of Thyroid NodulesJoko WowNo ratings yet
- J Eururo 2020 09 046Document20 pagesJ Eururo 2020 09 046Ivor Wiguna Hartanto WilopoNo ratings yet
- Jppres18.392 6.6.433Document16 pagesJppres18.392 6.6.433Benjamin Medina RangelNo ratings yet
- BreastCancerUpdate 1222 Lores FINALDocument24 pagesBreastCancerUpdate 1222 Lores FINALEmilio AssisNo ratings yet
- Reproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesDocument28 pagesReproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesFandoNo ratings yet
- Company ProfileDocument18 pagesCompany Profileabobaker solimanNo ratings yet
- A Practical Guide To Prostate Cancer Diagnosis and ManagementDocument11 pagesA Practical Guide To Prostate Cancer Diagnosis and ManagementAli TalalNo ratings yet
- Current Perioperative Management of Pheochromocytomas: Rashmi Ramachandran, Vimi RewariDocument7 pagesCurrent Perioperative Management of Pheochromocytomas: Rashmi Ramachandran, Vimi RewariIdhularfitraNo ratings yet
- Surgery: SciencedirectDocument7 pagesSurgery: SciencedirectAriska Nur FitrianaNo ratings yet
- Pain Management After Surgical Tonsillectomy: Is There A Favorable Analgesic?Document6 pagesPain Management After Surgical Tonsillectomy: Is There A Favorable Analgesic?Vladimir PutinNo ratings yet
- Cancers 14 03845Document15 pagesCancers 14 03845regigaby02No ratings yet
- Jppres18.392 6.6.433Document16 pagesJppres18.392 6.6.433Wilfredo Arango CallañaupaNo ratings yet
- Physiology, Gag Reflex - StatPearls - NCBI BookshelfDocument1 pagePhysiology, Gag Reflex - StatPearls - NCBI BookshelfVienna TulauanNo ratings yet
- Neuroanatomy, Spinal Cord Myotatic Reflex - StatPearls - NCBI Bookshelf 2Document1 pageNeuroanatomy, Spinal Cord Myotatic Reflex - StatPearls - NCBI Bookshelf 2Vienna TulauanNo ratings yet
- Katz 1Document16 pagesKatz 1Vienna TulauanNo ratings yet
- Different Types of Microscope and UsesDocument3 pagesDifferent Types of Microscope and UsesVienna TulauanNo ratings yet
- Unit 1 - Week (1) - Comprehensive Assessment: Intended Learning Outcomes (Week 1-ILO)Document28 pagesUnit 1 - Week (1) - Comprehensive Assessment: Intended Learning Outcomes (Week 1-ILO)John Van Dave TaturoNo ratings yet
- TiroideDocument10 pagesTiroideRosália CoutadaNo ratings yet
- Composition 1 S2 2020 FinalDocument46 pagesComposition 1 S2 2020 Finalelhoussaine.nahime00No ratings yet
- Fast Food Should Be BannedDocument2 pagesFast Food Should Be BannedHarrinson AlgarinNo ratings yet
- What Is Sleep Myoclonus, Twitching Jerks, or Movements?Document11 pagesWhat Is Sleep Myoclonus, Twitching Jerks, or Movements?do leeNo ratings yet
- 9201 Mark Scheme Paper2 International Gcse Biology Jun22Document21 pages9201 Mark Scheme Paper2 International Gcse Biology Jun22asdf0% (1)
- Cvboard - Study Strong PlannerDocument45 pagesCvboard - Study Strong PlannerZaina TNo ratings yet
- Prevalence and Risk Factors Associated With StrokeDocument9 pagesPrevalence and Risk Factors Associated With Strokeeduardo neiraNo ratings yet
- Standard Hostels - Ijhs-9-3-249Document8 pagesStandard Hostels - Ijhs-9-3-249BSL-2No ratings yet
- The Key Role of Micronutrients: Alan ShenkinDocument13 pagesThe Key Role of Micronutrients: Alan ShenkinTiara LioNo ratings yet
- Safety and Immunogenicity of A Heterologous Boost With A Recombinant VaccineDocument35 pagesSafety and Immunogenicity of A Heterologous Boost With A Recombinant VaccineAristegui NoticiasNo ratings yet
- Secretory Diarrheas: The Pathophysiology ofDocument14 pagesSecretory Diarrheas: The Pathophysiology ofRegia Verent MNo ratings yet
- Alopecia Areata in Covid 19 Case ReportDocument2 pagesAlopecia Areata in Covid 19 Case ReportAnti TjahyaNo ratings yet
- Neurotoxicology: Mona Hersi, Brittany Irvine, Pallavi Gupta, James Gomes, Nicholas Birkett, Daniel KrewskiDocument45 pagesNeurotoxicology: Mona Hersi, Brittany Irvine, Pallavi Gupta, James Gomes, Nicholas Birkett, Daniel KrewskiMAYRA PAZNo ratings yet
- Exercise For Fitness: (Shs-Videolecture-1 & 2 Week)Document18 pagesExercise For Fitness: (Shs-Videolecture-1 & 2 Week)Mark Joshua MandaniNo ratings yet
- Assessment of Kidney Function in ChildrenDocument19 pagesAssessment of Kidney Function in Childrenlinamaria.pedNo ratings yet
- Nutritional Problems in IndiaDocument87 pagesNutritional Problems in Indiagrace williamNo ratings yet
- AtorvastatinDocument2 pagesAtorvastatinJasmin T LarizaNo ratings yet
- Cardiogenic ShockDocument9 pagesCardiogenic Shockrio kharismaNo ratings yet
- I. Crossword Puzzle: Use The Provided Clues To Fill Out The Puzzle. (10 Items X 2 Points)Document2 pagesI. Crossword Puzzle: Use The Provided Clues To Fill Out The Puzzle. (10 Items X 2 Points)Kristel BoralNo ratings yet
- Dental Management of Handicapped ChildrenDocument18 pagesDental Management of Handicapped ChildrenDrBhawna AroraNo ratings yet
- Plagiarism Checker X Originality Report: Similarity Found: 14%Document17 pagesPlagiarism Checker X Originality Report: Similarity Found: 14%Bella Dama ShintaNo ratings yet
- Truth and Healing Commission On Indian Boarding School Policies in The United States ActDocument37 pagesTruth and Healing Commission On Indian Boarding School Policies in The United States Actjen_benderyNo ratings yet
- Nursing Care of Patients With Cardiac ProblemsDocument127 pagesNursing Care of Patients With Cardiac Problemssarah morleyNo ratings yet
- Investigatory Project (Natural Mosquito Repellent) Free Essay ExampleDocument7 pagesInvestigatory Project (Natural Mosquito Repellent) Free Essay ExampleAaliyah Marie AbaoNo ratings yet
- Chromo Blas To MycosisDocument10 pagesChromo Blas To MycosisElina GNo ratings yet
- 1 Semester: Anti-Migraine Agents Are Used To Treat Migraine HeadachesDocument26 pages1 Semester: Anti-Migraine Agents Are Used To Treat Migraine HeadachesMARY BERNADETTE EGANANo ratings yet