Download as pdf or txt
You might also like
- Mandela Washington Fellowship EssaysDocument3 pagesMandela Washington Fellowship EssaysNasiru Deen94% (16)
- (DOH HPB) PA6 Playbook 2021 - Key Assistance For Developing Adolescents (KADA) NetworkDocument71 pages(DOH HPB) PA6 Playbook 2021 - Key Assistance For Developing Adolescents (KADA) NetworkrkNo ratings yet
- DOH Family PlanningDocument39 pagesDOH Family PlanningSarte Rachelle AnneNo ratings yet
- Adolescent Health & Youth Development - Role of SKDocument28 pagesAdolescent Health & Youth Development - Role of SKJh UlzNo ratings yet
- 1.2B Safe Motherhood Program & Women's Health PDFDocument11 pages1.2B Safe Motherhood Program & Women's Health PDFStephen Pilar PortilloNo ratings yet
- Research Report IvaDocument30 pagesResearch Report Ivakayovu lawrenceNo ratings yet
- Bullying PreventionDocument8 pagesBullying Preventionellado.jab.cgcNo ratings yet
- MM Seminar InternasionalDocument21 pagesMM Seminar InternasionalPrinses JihanaNo ratings yet
- AHYDProgram PopComDocument65 pagesAHYDProgram PopComjune ortiz100% (1)
- DOH H P P: Ealth Rom Ot Ion RogramsDocument4 pagesDOH H P P: Ealth Rom Ot Ion RogramsBrandon BragatNo ratings yet
- Republic of The Philippines 2Document7 pagesRepublic of The Philippines 2Zairene Kyle Moralde HagutinNo ratings yet
- Abante KabataanDocument19 pagesAbante KabataanofficeofskmallaboNo ratings yet
- Introduction To Community PediatricsDocument24 pagesIntroduction To Community PediatricsAlex perrieNo ratings yet
- Reaction Paper On AdvocacyDocument5 pagesReaction Paper On Advocacyapi-32495846150% (6)
- Reproductive Health: 4.1 R H - P SDocument10 pagesReproductive Health: 4.1 R H - P SMamataMaharanaNo ratings yet
- Reproductive Health: 4.1 R H - P SDocument10 pagesReproductive Health: 4.1 R H - P SVikram SkNo ratings yet
- What Is Child ProtectionDocument2 pagesWhat Is Child ProtectionFaizan AhmadNo ratings yet
- wha77-advocacy-messagingDocument3 pageswha77-advocacy-messagingPrince Elie KOUAKOUNo ratings yet
- Family Welfare ServicesDocument20 pagesFamily Welfare Servicesbemina ja100% (2)
- Parental CareDocument2 pagesParental Care0-benk-0No ratings yet
- FP 2020 and Young People: Government of India's CommitmentDocument2 pagesFP 2020 and Young People: Government of India's CommitmentSiddharth MohantyNo ratings yet
- Adolescent Sexual and Reproductive Healt PDFDocument9 pagesAdolescent Sexual and Reproductive Healt PDFKHAIRUNISA RAHMANIANo ratings yet
- Philippine Reproductive Health BillDocument4 pagesPhilippine Reproductive Health BillDr. Liza Manalo100% (11)
- Support:: The Spreading of The Reproductive Health EducationDocument34 pagesSupport:: The Spreading of The Reproductive Health EducationSavannah KhrisNo ratings yet
- Child Welfare Policies and Programs in IndiaDocument5 pagesChild Welfare Policies and Programs in IndiaArkaprava BhowmikNo ratings yet
- Reproductive Health Policy: First DraftDocument17 pagesReproductive Health Policy: First DraftFoster K KaundaNo ratings yet
- Lennel Tobol EMTECH CONCEPT PAPERDocument10 pagesLennel Tobol EMTECH CONCEPT PAPERCarrel KuunNo ratings yet
- Business DevelopemntDocument17 pagesBusiness Developemntayan ghoshNo ratings yet
- NOTES - Group 1 DOH PROGRAMSDocument18 pagesNOTES - Group 1 DOH PROGRAMSPatrisha Bianca Paige BadillesNo ratings yet
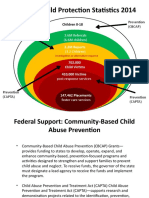
- National Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)Document14 pagesNational Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)MarryRose Dela Torre FerrancoNo ratings yet
- Implementing Mechanism For EO 141 Presentation For NGAs - Asof15July 1 2Document35 pagesImplementing Mechanism For EO 141 Presentation For NGAs - Asof15July 1 2Reyan ArintoNo ratings yet
- Department of Health ProgramsDocument49 pagesDepartment of Health ProgramsKylie Golindang100% (1)
- Strategic Framework - Adol HealthDocument29 pagesStrategic Framework - Adol HealthShardin Labawan-Juen,RNNo ratings yet
- Programmes and POLICIES-CHILDREN - GJDocument120 pagesProgrammes and POLICIES-CHILDREN - GJRobin RajuNo ratings yet
- Teen Pregnancy Speech - SVDocument4 pagesTeen Pregnancy Speech - SVScribdTranslationsNo ratings yet
- Menu of Programs Services and Interventions FinalDocument19 pagesMenu of Programs Services and Interventions FinalRon RealinNo ratings yet
- Ra 10354Document22 pagesRa 10354Alni Dorothy Alfa EmphasisNo ratings yet
- Introduction To Reproductive Health, Medical StudentsDocument25 pagesIntroduction To Reproductive Health, Medical StudentsEli Zza KoiralaNo ratings yet
- Cordero, VLM - Community Bodies Dealing With The Child WelfareDocument20 pagesCordero, VLM - Community Bodies Dealing With The Child WelfareAlfred AtalinNo ratings yet
- Global Health Issue: Kesehatan Ibu Dan AnakDocument67 pagesGlobal Health Issue: Kesehatan Ibu Dan AnakEra ZanaNo ratings yet
- Family PlanningDocument113 pagesFamily PlanningKailash NagarNo ratings yet
- Prevention of Teen PregnancyDocument14 pagesPrevention of Teen PregnancyjanineNo ratings yet
- Child Development Programme in Singapore 1988 To 2007: Mmed (Paed), Fams, FRCPCHDocument13 pagesChild Development Programme in Singapore 1988 To 2007: Mmed (Paed), Fams, FRCPCHKevin FongNo ratings yet
- Instructiona Design .1Document12 pagesInstructiona Design .1virgo paigeNo ratings yet
- Alphatemplate ThesisDocument32 pagesAlphatemplate ThesisAizelle MangawitNo ratings yet
- CUAMM - 2 Child Safeguarding Policy - Dec. 2019Document8 pagesCUAMM - 2 Child Safeguarding Policy - Dec. 2019Angela BologanNo ratings yet
- Pursuing Equality in The Midst of Disparity: Health and Well-Being of Children With DisabilitiesDocument21 pagesPursuing Equality in The Midst of Disparity: Health and Well-Being of Children With DisabilitiesfericNo ratings yet
- Research Proposal TemplateDocument25 pagesResearch Proposal Templateruth caina castilloNo ratings yet
- Early Childhood Development - UNICEF Vision For Every ChildDocument32 pagesEarly Childhood Development - UNICEF Vision For Every ChildYakubu Abdul sommedNo ratings yet
- Preventing Child Abuse and NeglectDocument4 pagesPreventing Child Abuse and NeglectLee GaylordNo ratings yet
- (BSN2-2) CHN Lec - Lesson No.3Document5 pages(BSN2-2) CHN Lec - Lesson No.3Abish Julienne PecundoNo ratings yet
- ArhDocument13 pagesArhMargarita Banhan-allagaoNo ratings yet
- National Health Policy For ChildrenDocument10 pagesNational Health Policy For ChildrenPriya100% (2)
- Africa VAC and Care Report Single PageDocument76 pagesAfrica VAC and Care Report Single PagesofiabloemNo ratings yet
- TraumaDocument30 pagesTraumaq.ne1997No ratings yet
- © Ncert Not To Be Republished: Reproductive HealthDocument10 pages© Ncert Not To Be Republished: Reproductive HealthlipidusNo ratings yet
- Open The Door To SafetyDocument11 pagesOpen The Door To SafetySheena Marie M. TarleNo ratings yet
- Reproductive Health: 4.1 R H - P SDocument10 pagesReproductive Health: 4.1 R H - P SShashank ShekharNo ratings yet
- JFHJHJDDocument7 pagesJFHJHJDJerra LynNo ratings yet
- Child Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsFrom EverandChild Sexual Abuse: Current Evidence, Clinical Practice, and Policy DirectionsNo ratings yet
- Recent Literature Review On Teenage PregnancyDocument5 pagesRecent Literature Review On Teenage Pregnancyafmzvaeeowzqyv100% (1)
- Teenage Pregnancy: Please Go Over The Spacing and Format of The Title PageDocument10 pagesTeenage Pregnancy: Please Go Over The Spacing and Format of The Title Pageanthony ken jimenezNo ratings yet
- Literature ReviewDocument8 pagesLiterature Reviewapi-547519009No ratings yet
- Dissertation Questions On Teenage PregnancyDocument7 pagesDissertation Questions On Teenage PregnancyPayToDoMyPaperBatonRouge100% (1)
- Chapter 1 Pr2Document9 pagesChapter 1 Pr2Shanelle CruzNo ratings yet
- Teen Pregnancies Feature WritingDocument1 pageTeen Pregnancies Feature WritingMcMasterPro GeniusNo ratings yet
- Developmental Psychology Prelim and Finals Reviewer - CompressDocument31 pagesDevelopmental Psychology Prelim and Finals Reviewer - CompressGlory Mae ProllesNo ratings yet
- Sample Abyip 2021 With Project DesignsDocument71 pagesSample Abyip 2021 With Project DesignsTreasurer DJLANo ratings yet
- Front Page 1-5Document5 pagesFront Page 1-5Cigrid Justine GutierrezNo ratings yet
- Premarital SexDocument1 pagePremarital SexMarianne Daphne Guevarra0% (1)
- Speech Project HaswadiDocument4 pagesSpeech Project HaswadifahmiNo ratings yet
- Communication Plan (Djalene Toledo)Document9 pagesCommunication Plan (Djalene Toledo)Djalene ToledoNo ratings yet
- Sexeducation PDFDocument35 pagesSexeducation PDFCosmin-abel CegaNo ratings yet
- Background of The StudyDocument3 pagesBackground of The StudyKeena Joy Awisan - Pinas87% (23)
- Filipino Teen PregnancyDocument25 pagesFilipino Teen PregnancyAngel Cruz100% (1)
- ISSUE: Child Marriage As A Way Out of Poverty in Some Religions and Culture in TheDocument2 pagesISSUE: Child Marriage As A Way Out of Poverty in Some Religions and Culture in TheIm Still StudyingNo ratings yet
- Performance Task in HealthDocument9 pagesPerformance Task in HealthJoshua Emmanuel LedesmaNo ratings yet
- Platinum Gazette 10 Feb 2012Document12 pagesPlatinum Gazette 10 Feb 2012Anonymous w8NEyXNo ratings yet
- Caparoso (Awareness) ResearchDocument33 pagesCaparoso (Awareness) ResearchEdwardJohnG.CalubIINo ratings yet
- Research Paper EARLY PREGNANCYDocument11 pagesResearch Paper EARLY PREGNANCYMaria Concepcion TuvillaNo ratings yet
- The Only Exception: Teenage Pregnancy in The Philippines: January 2018Document29 pagesThe Only Exception: Teenage Pregnancy in The Philippines: January 2018Abby YambaoNo ratings yet
- Chapter 4.4 Teenage Pregnancy (Autosaved)Document78 pagesChapter 4.4 Teenage Pregnancy (Autosaved)Garry MartinezNo ratings yet
- English 8 Q3 Module 3Document31 pagesEnglish 8 Q3 Module 3ringoNo ratings yet
- Research EssayDocument7 pagesResearch Essayapi-537816179No ratings yet
- Psychology and Education: A Multidisciplinary Journal: 10.5281/zenodo.8093804 28Document21 pagesPsychology and Education: A Multidisciplinary Journal: 10.5281/zenodo.8093804 28Psychology and Education: A Multidisciplinary JournalNo ratings yet
- Peer Pressure: The Causes of Teenage Pregnancy in The PhilippinesDocument3 pagesPeer Pressure: The Causes of Teenage Pregnancy in The PhilippinesSamantha Cheska100% (1)
- A N D Icpd + H Ealth and Rights and Eastern Europe N TDocument152 pagesA N D Icpd + H Ealth and Rights and Eastern Europe N TKate MessNo ratings yet
- MAPEH (Health) : Quarter 1 - Module 6: Teenage Issues and Concerns: Pre-Marital Sex and Teenage PregnancyDocument11 pagesMAPEH (Health) : Quarter 1 - Module 6: Teenage Issues and Concerns: Pre-Marital Sex and Teenage PregnancyAlbert Ian Casuga100% (1)