Download as pdf or txt
You might also like
- Bact211 Answer Key Long ExamDocument1 pageBact211 Answer Key Long ExamKristine PangahinNo ratings yet
- CHAPTER 19sexually Transmitted Infection 1Document50 pagesCHAPTER 19sexually Transmitted Infection 1Nick Martin RequejoNo ratings yet
- TreponemaDocument13 pagesTreponemaقاسم اليوسفيNo ratings yet
- Syphilis: Michelle LinardiDocument20 pagesSyphilis: Michelle Linardimichelle95No ratings yet
- Mti Notes Stds-1Document24 pagesMti Notes Stds-1Mahmoud KhelfaNo ratings yet
- Syphilislecturepp 180719075049Document32 pagesSyphilislecturepp 180719075049abdellatifNo ratings yet
- Syphilislecturepp 180719075049Document32 pagesSyphilislecturepp 180719075049EndaleNo ratings yet
- Sexually Transmitted InfectionsDocument11 pagesSexually Transmitted InfectionsDaniella TupasNo ratings yet
- Lecture - 9Document24 pagesLecture - 9ASADULLAH AL GALIBNo ratings yet
- Syphilis: Dr. Sachin PatelDocument36 pagesSyphilis: Dr. Sachin PatelAakash PrajapatiNo ratings yet
- Syphilislecturepp 180719075049Document30 pagesSyphilislecturepp 180719075049EndaleNo ratings yet
- Sexually Transmitted Diseases (STD'S)Document34 pagesSexually Transmitted Diseases (STD'S)Sajid NadafNo ratings yet
- Lection 8 SyphilisDocument39 pagesLection 8 SyphilisAtawna AtefNo ratings yet
- Syphillis, Herpes, Hepatitis, and HPV: Symptoms, Diagnosis, and TreatmentDocument43 pagesSyphillis, Herpes, Hepatitis, and HPV: Symptoms, Diagnosis, and TreatmentsgolbariNo ratings yet
- Reproductive MicroDocument55 pagesReproductive MicroThimira WaidyasekaraNo ratings yet
- Torch: Jessica Santoso Moderator: Dr. Maimun ZA, M.Kes, SP - PKDocument79 pagesTorch: Jessica Santoso Moderator: Dr. Maimun ZA, M.Kes, SP - PKTommy KristantoNo ratings yet
- Chlamydia by Rosemary C. AgboDocument24 pagesChlamydia by Rosemary C. AgboRosemaryNo ratings yet
- SyphilisDocument39 pagesSyphilisEINSTEIN2D100% (2)
- It 38 Microbiology in Obgyn 24Document146 pagesIt 38 Microbiology in Obgyn 24dhjekwkwNo ratings yet
- UP PGH 2019 Interns Review 2 Gyne InfectionsDocument39 pagesUP PGH 2019 Interns Review 2 Gyne InfectionsTrisNo ratings yet
- Sexually Transmitte D Infections: Keeshia Anna Zerrudo Clinical Clerk Iloilo Doctors' Hospital Inc. August 18, 2020Document117 pagesSexually Transmitte D Infections: Keeshia Anna Zerrudo Clinical Clerk Iloilo Doctors' Hospital Inc. August 18, 2020Angela SaldajenoNo ratings yet
- Final Infectious Pe - 1-EditDocument59 pagesFinal Infectious Pe - 1-EditAhmad SobihNo ratings yet
- Sexually Transmitted DiseasesDocument120 pagesSexually Transmitted DiseasesGliza Jane100% (4)
- Rep 1Document50 pagesRep 1bbbbbvvvvv1No ratings yet
- Syphilis PDFDocument32 pagesSyphilis PDFAiswarya MishraNo ratings yet
- Genera:: Treponema & BorreiliaDocument25 pagesGenera:: Treponema & BorreiliaKhalifa Sifaw Ghenghesh100% (1)
- Agent: Defining Characteristics Clinical Diseases Laboratory Diagnosis Treatment SpirochetesDocument6 pagesAgent: Defining Characteristics Clinical Diseases Laboratory Diagnosis Treatment SpirochetesEd Daniel DavisNo ratings yet
- STT-Module 4Document68 pagesSTT-Module 4Abu Rizwana Adem ManNo ratings yet
- Sexually Transmitted Infections and PregnancyDocument19 pagesSexually Transmitted Infections and PregnancyBeyins TiuNo ratings yet
- Sexual Transmitted InfectionsDocument44 pagesSexual Transmitted InfectionsDeshielanny AlagumolyNo ratings yet
- 04 SU Male Genital Lesions BrimhallDocument93 pages04 SU Male Genital Lesions BrimhallMark AkaphotNo ratings yet
- Chapter 3 Syphilis Serology DZ 2010Document75 pagesChapter 3 Syphilis Serology DZ 2010Anduamlak TeferaNo ratings yet
- SYPHILISDocument6 pagesSYPHILISKhristine Dyanne San JoaquinNo ratings yet
- Gonorrhea and SyphilisDocument55 pagesGonorrhea and Syphilisjoshy221196No ratings yet
- Spirochetes: Dr.T.V.Rao MDDocument99 pagesSpirochetes: Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- 2 - SyphilisDocument24 pages2 - SyphilisCaila LimNo ratings yet
- Other Genital Infections Herpes Simplex:: Clinical FeaturesDocument5 pagesOther Genital Infections Herpes Simplex:: Clinical FeaturesNashat SaadiNo ratings yet
- Tests in SyphilisDocument9 pagesTests in SyphilisaditiNo ratings yet
- Syphilis in ChildrenDocument16 pagesSyphilis in ChildrenFatmi Eka PutriNo ratings yet
- 8.sti 2Document44 pages8.sti 2Mahrukh SiddiquiNo ratings yet
- Final Infectious Pe - 1Document49 pagesFinal Infectious Pe - 1Ahmad SobihNo ratings yet
- Sexually Transmitted DiseasesDocument19 pagesSexually Transmitted DiseasesAhmed HajiNo ratings yet
- Family Spirochaetaceae and Leptospiraceae-1Document29 pagesFamily Spirochaetaceae and Leptospiraceae-1temesgensemahegn55No ratings yet
- Common Sexually Transmitted Diseases (STDS) and Hiv-Infected WomenDocument41 pagesCommon Sexually Transmitted Diseases (STDS) and Hiv-Infected WomenHarly DavidsonNo ratings yet
- Sexually Transmitted Infections 19-21Document4 pagesSexually Transmitted Infections 19-21Ashar AhmadNo ratings yet
- SpirochaetesDocument14 pagesSpirochaetesCaroline NgabuNo ratings yet
- STD Summary PresentationDocument52 pagesSTD Summary PresentationMike AndersenNo ratings yet
- Ocular Syphilis 2Document19 pagesOcular Syphilis 2henok birukNo ratings yet
- Rapid Plasma Reagin SyphilisDocument24 pagesRapid Plasma Reagin SyphilisVia Gail CanlasNo ratings yet
- Torch: Diana Khoirun Nida - 1710211042Document34 pagesTorch: Diana Khoirun Nida - 1710211042Diana Khoirun NidaNo ratings yet
- Sexually Transmitted InfectionDocument11 pagesSexually Transmitted Infectionmark OrpillaNo ratings yet
- SYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Document15 pagesSYPHILIS (103 To 108) PPT - PPTX - 20230906 - 161225 - 0000Aaditya GadhviNo ratings yet
- Sexually Transmitted Disease STDDocument47 pagesSexually Transmitted Disease STDSurya DoleyNo ratings yet
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini67% (6)
- Treponema PallidumDocument25 pagesTreponema Pallidumlaiba raoNo ratings yet
- STD - SyphilisDocument14 pagesSTD - SyphilisAnshuli SinghalNo ratings yet
- Could It Be An STI?: DR Neelam DoshiDocument67 pagesCould It Be An STI?: DR Neelam Doshijoee ahmedNo ratings yet
- Serology of Bacteria, Viruses and ParasitesDocument128 pagesSerology of Bacteria, Viruses and Parasitesreginarosesalazar0127No ratings yet
- Communicable DiseasesDocument6 pagesCommunicable DiseasesLory LynNo ratings yet
- Chapter 44 STIDocument5 pagesChapter 44 STIRebeccaNo ratings yet
- US Nursery Pigs M. Hyo PRDC Case Study (Roberts, 2011)Document4 pagesUS Nursery Pigs M. Hyo PRDC Case Study (Roberts, 2011)nick224No ratings yet
- Resolution On Virus SuperspreadersDocument2 pagesResolution On Virus SuperspreadersBARANGAY MOLINO IINo ratings yet
- Project On Sexually Transmitted Disease by Pawan PatelDocument30 pagesProject On Sexually Transmitted Disease by Pawan PatelPawan Patel100% (1)
- VivaDiag SARS-CoV-2 Ag Rapid Test Brochure (En) PDFDocument1 pageVivaDiag SARS-CoV-2 Ag Rapid Test Brochure (En) PDFBPG ServiceNo ratings yet
- Concept PaperDocument1 pageConcept PaperBrent FabialaNo ratings yet
- Signs and SymptomsDocument7 pagesSigns and SymptomsJV DeeNo ratings yet
- ChikungunyaDocument19 pagesChikungunyaapi-388689708No ratings yet
- Everything You Need To Know About The Coronavirus Vaccines: Uday Kode-WRA 101 - Section 084Document9 pagesEverything You Need To Know About The Coronavirus Vaccines: Uday Kode-WRA 101 - Section 084UdayNo ratings yet
- Kaviyarasan Visitor PassDocument7 pagesKaviyarasan Visitor PassTRISTAR TEKZONENo ratings yet
- TB CPG Map by DR Syafiq SalhadiDocument1 pageTB CPG Map by DR Syafiq SalhadirebeccaNo ratings yet
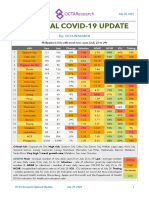
- National COVID-19 Update by Octa Research On July 30, 2021Document2 pagesNational COVID-19 Update by Octa Research On July 30, 2021RapplerNo ratings yet
- Karakteristik Penderita Abses Submandibular Di Departemen THT-KL Rsup Sanglah DenpasarDocument6 pagesKarakteristik Penderita Abses Submandibular Di Departemen THT-KL Rsup Sanglah DenpasarEndy Garret BongartzNo ratings yet
- Caliciviridae: Aby Elijah BernardinoDocument26 pagesCaliciviridae: Aby Elijah BernardinoabybrrNo ratings yet
- 3 Nobivac KC Primary Course With Option v.L4Document1 page3 Nobivac KC Primary Course With Option v.L4Vety PutriNo ratings yet
- African Sleeping Sickness Data PresentationDocument10 pagesAfrican Sleeping Sickness Data PresentationDuncan DaoNo ratings yet
- Holistic Care of People Living With HIV/AIDS by DR A.K. Gupta, DSACSDocument36 pagesHolistic Care of People Living With HIV/AIDS by DR A.K. Gupta, DSACSdr.a.k.gupta6924100% (1)
- Algoritma Tes HIVDocument31 pagesAlgoritma Tes HIVyurdiansyahNo ratings yet
- Robert Kennedy, JR.: "The Government Has Been Trying For AlmostDocument3 pagesRobert Kennedy, JR.: "The Government Has Been Trying For AlmostjayjonbeachNo ratings yet
- Eng10 - Q1 - W4 Comparison and Contrast Compare and Contrast The Contents of The Materials Viewed With OutsideDocument27 pagesEng10 - Q1 - W4 Comparison and Contrast Compare and Contrast The Contents of The Materials Viewed With OutsideJonalyn MempinNo ratings yet
- Measles (Script) Scenario: News Casting Cast: Jamila Tahil - News AnchorDocument2 pagesMeasles (Script) Scenario: News Casting Cast: Jamila Tahil - News AnchorAhmed-Adhiem Bahjin KamlianNo ratings yet
- Vaginitis BartolinitisDocument28 pagesVaginitis Bartolinitisfani kurniaNo ratings yet
- Malaria PathogenesisDocument39 pagesMalaria PathogenesisRasyiqa TharifaNo ratings yet
- 2015 Abwarie Target PlanDocument55 pages2015 Abwarie Target PlanDaniel HaileNo ratings yet
- Sequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDocument2 pagesSequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDonnaNo ratings yet
- Y2S2 Mosquitoes - RumalaDocument45 pagesY2S2 Mosquitoes - RumalamicroperadeniyaNo ratings yet
- Part IIDocument15 pagesPart IIIan LapidezNo ratings yet
- Brugia MalayiDocument12 pagesBrugia Malayimuga restunaeshaNo ratings yet
- Daftar PustakaDocument4 pagesDaftar PustakaNurulNo ratings yet
- AcyclovirDocument9 pagesAcyclovirAnia DołomisiewiczNo ratings yet