Download as pdf or txt
You might also like
- The ESC Textbook of Sports CardiologyDocument478 pagesThe ESC Textbook of Sports CardiologyIBFiS100% (1)
- K Sembulingam Essentials of Medical Physiology 6th 105 PDFDocument11 pagesK Sembulingam Essentials of Medical Physiology 6th 105 PDFBlerta Deari100% (3)
- Cardiac Cycle by Bala GoyalDocument14 pagesCardiac Cycle by Bala Goyaltee su lingNo ratings yet
- Cardiac CycleDocument35 pagesCardiac CycleEnuga Applegate100% (1)
- Study FastDocument49 pagesStudy FastmbbsporalekhaNo ratings yet
- PC Cardiac CycleDocument29 pagesPC Cardiac CycleSebontu HasenNo ratings yet
- Cardiac Cycle: DR Rida Ajmal KhanDocument29 pagesCardiac Cycle: DR Rida Ajmal KhanMooma fatimaNo ratings yet
- Cardiovascular SystemDocument50 pagesCardiovascular Systemkintan kamila100% (1)
- Lecture On Cardiac Cycle by DR RoomiDocument43 pagesLecture On Cardiac Cycle by DR RoomiMudassar Roomi100% (2)
- CARDIAC CYCLE - Part I PDFDocument55 pagesCARDIAC CYCLE - Part I PDFChirag Dagar100% (1)
- The Cardiac CycleDocument19 pagesThe Cardiac CycleRebi NesroNo ratings yet
- Physiology Shet #7&8Document12 pagesPhysiology Shet #7&8Rawan Abu HammourNo ratings yet
- 4,5-Cardiac Cycle 1&2Document31 pages4,5-Cardiac Cycle 1&2Aqeel Raza HessamNo ratings yet
- Cardiac CycleDocument13 pagesCardiac Cyclekaursukhmanvir0921No ratings yet
- Cardiac Cycle NotesDocument20 pagesCardiac Cycle NotesKelly Yeow100% (3)
- 5 Cardiac Cycle & Heart SoundsDocument32 pages5 Cardiac Cycle & Heart SoundsDisha SuvarnaNo ratings yet
- Cardiovascular PhysiologyDocument88 pagesCardiovascular Physiologykhorrami4No ratings yet
- DR Najeeb Cardiac CycleDocument5 pagesDR Najeeb Cardiac Cycleعلي. احمد100% (1)
- Cardiac Cycle by Dr. RoomiDocument71 pagesCardiac Cycle by Dr. RoomiMudassar Roomi100% (3)
- Cardiac CycleDocument30 pagesCardiac CycleCarrine Liew100% (2)
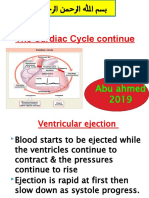
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 pagesThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 pagesThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- The Cardiac Cycle: Dr. Abdalla Adam AbdallaDocument15 pagesThe Cardiac Cycle: Dr. Abdalla Adam AbdallaNimisha BalakrishnanNo ratings yet
- The Cardiac Cycle: Dr. Abdalla Adam AbdallaDocument15 pagesThe Cardiac Cycle: Dr. Abdalla Adam AbdallaNimisha BalakrishnanNo ratings yet
- Cardiac Cycle: DR Rakesh JainDocument97 pagesCardiac Cycle: DR Rakesh JainKemoy FrancisNo ratings yet
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Document21 pagesCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNo ratings yet
- Heart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument33 pagesHeart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraXeniel AlastairNo ratings yet
- Cardiac CycleDocument9 pagesCardiac Cycle502-s21-027No ratings yet
- Cardiac Cycle: Dr. Arun Goel Associate Professor Department of PhysiologyDocument27 pagesCardiac Cycle: Dr. Arun Goel Associate Professor Department of PhysiologyThird Year B PharmNo ratings yet
- Cardiac CycleDocument14 pagesCardiac CyclenidhiNo ratings yet
- Cardiac CycleDocument7 pagesCardiac Cycletewogbadeomobuwajo005No ratings yet
- Cardiovascular Physiology: October 25, 2010Document51 pagesCardiovascular Physiology: October 25, 2010VinuPrakashJ.No ratings yet
- Cardiac Cycle - DR Rakesh JainDocument97 pagesCardiac Cycle - DR Rakesh JainEmmieNo ratings yet
- Assign MNTDocument13 pagesAssign MNTADITYAROOP PATHAKNo ratings yet
- The Sequence of Events That Occur in The Heart During Cardiac CycleDocument13 pagesThe Sequence of Events That Occur in The Heart During Cardiac CycleADITYAROOP PATHAKNo ratings yet
- Cardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHDocument56 pagesCardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHRamakrishnanNo ratings yet
- Cardiac CycleDocument36 pagesCardiac Cycleanushkav443No ratings yet
- Cardiac CycleDocument18 pagesCardiac CycleKundan GuptaNo ratings yet
- Cardiac Cycle: Electrical and Mechanical Events That Occur in TheDocument25 pagesCardiac Cycle: Electrical and Mechanical Events That Occur in The28g8jcfcqfNo ratings yet
- Oral PathologyDocument23 pagesOral PathologyRuba AbbassNo ratings yet
- Cardiac CycleDocument24 pagesCardiac CycleKiran KhurshidNo ratings yet
- Physiology of CardiovascularDocument74 pagesPhysiology of CardiovascularStevan SalosaNo ratings yet
- Electrical Conduction in The HeartDocument35 pagesElectrical Conduction in The HeartNormasnizam Mohd NoorNo ratings yet
- Cardiac Cycle FinalDocument37 pagesCardiac Cycle Finalindra_jeet2009No ratings yet
- Physiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Document62 pagesPhysiology: Zhao Chun-ling (赵春玲) Email: Phone:18683073667Akshay ChaudharyNo ratings yet
- Cardiac Cycle Physiology-18!12!2018Document70 pagesCardiac Cycle Physiology-18!12!2018kolyagolpreetikNo ratings yet
- Lecture-5 Cardiac CycleDocument28 pagesLecture-5 Cardiac Cyclettalhalatif99No ratings yet
- Prof DR Najneen AkhterDocument62 pagesProf DR Najneen Akhterislamamirul0487No ratings yet
- Circulatory SystemDocument304 pagesCirculatory Systemyapyihao2100% (1)
- Cvs PPT 2) BpehssDocument35 pagesCvs PPT 2) BpehssAmbreen GhafoorNo ratings yet
- DR Rahimah Zakaria Dept of PhysiologyDocument31 pagesDR Rahimah Zakaria Dept of PhysiologyChokJunHoongNo ratings yet
- Cardiovascular PhysiologyDocument55 pagesCardiovascular Physiologys8f2dmzdvjNo ratings yet
- Acute Severe Chest Pain: Presented By: Arwa H. Al-OnayzanDocument11 pagesAcute Severe Chest Pain: Presented By: Arwa H. Al-OnayzanShampa SenNo ratings yet
- Acuteseverechestpain 171218172053 PDFDocument11 pagesAcuteseverechestpain 171218172053 PDFShampa SenNo ratings yet
- Cardiac CycleDocument30 pagesCardiac CycleAdel100% (1)
- K - 12 Heart As A Pump (Fisiologi)Document36 pagesK - 12 Heart As A Pump (Fisiologi)missirenaNo ratings yet
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- Cardiovascular Physiology: Lawrence A. Olatunji ReaderDocument46 pagesCardiovascular Physiology: Lawrence A. Olatunji ReaderMaryam Ogunade0% (1)
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- KP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Document68 pagesKP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Try MutiaraNo ratings yet
- NGCM 112 Course OutlineDocument7 pagesNGCM 112 Course OutlineAYTONA, JAMAICA F.No ratings yet
- DiastologiaDocument10 pagesDiastologiaReinaldo Pacheco VásquezNo ratings yet
- Week 2 - Ms1 Course Task - Cu 2-RoveroDocument2 pagesWeek 2 - Ms1 Course Task - Cu 2-RoveroJohnmarkLorenzanaRoveroNo ratings yet
- 2024-CPAP May Promote An Endothelial Inflammatory Milieu inDocument12 pages2024-CPAP May Promote An Endothelial Inflammatory Milieu inKelly RochaNo ratings yet
- Acute Myocardial InfarctionDocument42 pagesAcute Myocardial InfarctionAzra BalochNo ratings yet
- Angina Set #8Document26 pagesAngina Set #8Zaid Al-KadhimiNo ratings yet
- Esc Vs Aha Severe ASDocument17 pagesEsc Vs Aha Severe ASYogi AndrewNo ratings yet
- Tif31Document41 pagesTif31HCX dghhqNo ratings yet
- Arrhythmia in Emergency 111Document21 pagesArrhythmia in Emergency 111Iyas JehadNo ratings yet
- Articulo - Theory and Desicion MakingDocument5 pagesArticulo - Theory and Desicion MakingJaNe RNNo ratings yet
- Koran Pasien PJT LT4 2 Feb 2023Document9 pagesKoran Pasien PJT LT4 2 Feb 2023maspul lamuruprintNo ratings yet
- Luis Fernando Pava MolanoDocument5 pagesLuis Fernando Pava MolanoVallejo Romo Alberto CristianNo ratings yet
- Echo Screening: Dr. Dilip JainDocument1 pageEcho Screening: Dr. Dilip JainPriyansh TanejaNo ratings yet
- Preoperative Cardiac Risk AssessmentDocument16 pagesPreoperative Cardiac Risk Assessmentkrysmelis MateoNo ratings yet
- Report V-Damage Analysis - Cardiovascular 15-44 - V3Document22 pagesReport V-Damage Analysis - Cardiovascular 15-44 - V3Zerohedge Janitor100% (1)
- Heart Rate, Life Expectancy and The Cardiovascular System: Therapeutic ConsiderationsDocument14 pagesHeart Rate, Life Expectancy and The Cardiovascular System: Therapeutic ConsiderationsTapan Kumar RoyNo ratings yet
- Medical Surgical NursingDocument16 pagesMedical Surgical NursingMelvin TarkporNo ratings yet
- Ekg InterpretationDocument26 pagesEkg Interpretationpaulzilicous.artNo ratings yet
- Multiple Small Feedings of The Mind: CardiologyDocument26 pagesMultiple Small Feedings of The Mind: CardiologyJuan Pablo Muñoz CastellónNo ratings yet
- ECG Cheat Sheet: Atrial Fibrillation. Treatment?Document2 pagesECG Cheat Sheet: Atrial Fibrillation. Treatment?nreena aslamNo ratings yet
- Elizabeth M. Cherry and Flavio H. FentonDocument9 pagesElizabeth M. Cherry and Flavio H. FentonMaram RanadeepNo ratings yet
- Role of Transesophageal Echocardiography (Tee) in Cardiac SurgeryDocument35 pagesRole of Transesophageal Echocardiography (Tee) in Cardiac SurgeryIJAR JOURNALNo ratings yet
- CT 2Document16 pagesCT 2TGB LEGENDNo ratings yet
- EPSSDocument3 pagesEPSSRavin DebieNo ratings yet
- 01 Cir 22 3 385Document20 pages01 Cir 22 3 385Diana AndreeaNo ratings yet
- Meus Paces Instructions - CVSDocument4 pagesMeus Paces Instructions - CVSMahmud DipuNo ratings yet
- Nursing Care Plans For Activity IntoleranceDocument3 pagesNursing Care Plans For Activity Intoleranceravenshadow100% (2)
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- Medical Surgical Nursing - Cardiovascular System DisordersDocument11 pagesMedical Surgical Nursing - Cardiovascular System DisordersSofia LiNo ratings yet