Download as pdf or txt
You might also like
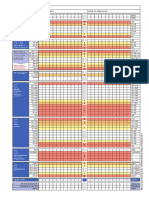
- NEWS2 Chart 3 - NEWS Observation Chart - 0 PDFDocument1 pageNEWS2 Chart 3 - NEWS Observation Chart - 0 PDFFlouria Stefanny SimatupangNo ratings yet
- Colangitis Esclerosante Secundaria 2013Document9 pagesColangitis Esclerosante Secundaria 2013Lili AlcarazNo ratings yet
- Rcem Learning FRCEM PRIMARY Paper 3 PDFDocument8 pagesRcem Learning FRCEM PRIMARY Paper 3 PDFsamee0% (2)
- Left-Sided Portal Hypertension: A Clinical Challenge: Hipertensão Portal Esquerda: Um Desafio ClínicoDocument3 pagesLeft-Sided Portal Hypertension: A Clinical Challenge: Hipertensão Portal Esquerda: Um Desafio ClínicomichaelqurtisNo ratings yet
- Emphysematous and Xanthogranulomatous Pyelonephritis: Rare DiagnosisDocument3 pagesEmphysematous and Xanthogranulomatous Pyelonephritis: Rare DiagnosisckingpacNo ratings yet
- An Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystDocument3 pagesAn Unusual Case of Polycythemia Vera With A Complication of Pancreatic PseudocystAgus PrimaNo ratings yet
- 1 s2.0 S0268960X08000787 Main PDFDocument7 pages1 s2.0 S0268960X08000787 Main PDFmohamedhazemelfollNo ratings yet
- Amoebic Liver Abscess: Clinical MedicineDocument5 pagesAmoebic Liver Abscess: Clinical MedicineAizat KamalNo ratings yet
- Angio Displa SiaDocument4 pagesAngio Displa SiaBelaFawziaNo ratings yet
- Solitary Rectal UlcerDocument8 pagesSolitary Rectal UlcerAnca DimitriuNo ratings yet
- Sonographic Pattrens PDFDocument5 pagesSonographic Pattrens PDFmmdadnanNo ratings yet
- AIDS CholangiopathyDocument7 pagesAIDS CholangiopathyedwincliffordNo ratings yet
- Letters To The Editor: Membranous Glomerulonephritis in A Patient With SyphilisDocument2 pagesLetters To The Editor: Membranous Glomerulonephritis in A Patient With SyphilisBetty Romero BarriosNo ratings yet
- ArtigoDocument1 pageArtigovania cardosoNo ratings yet
- 1271 HSP .FullDocument8 pages1271 HSP .FulldonkeyendutNo ratings yet
- Gallbladder PolypDocument28 pagesGallbladder PolypChristian LoyolaNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- Glomerular Disease in ChildrenDocument8 pagesGlomerular Disease in ChildrenMuti IlmarifaNo ratings yet
- Pyogenic Liver AbscessDocument10 pagesPyogenic Liver AbscessErnesto Sebastian GarcíaNo ratings yet
- Mallory Weiss Syndrome - StatPearls - NCBI BookshelfDocument9 pagesMallory Weiss Syndrome - StatPearls - NCBI BookshelfDaniela EstradaNo ratings yet
- EsplenomegaliaDocument24 pagesEsplenomegaliaJhonatan Efraín López CarbajalNo ratings yet
- Renal Disease in TuberculosisDocument10 pagesRenal Disease in TuberculosismiguelNo ratings yet
- Help Pedsurgeryafrica81Document7 pagesHelp Pedsurgeryafrica81tikaauliaNo ratings yet
- 10 11648 J CRJ 20200802 14Document3 pages10 11648 J CRJ 20200802 14Marj MendezNo ratings yet
- Kidney 360 2020 MicrohematuriaDocument7 pagesKidney 360 2020 MicrohematuriaRichardNo ratings yet
- Biliary AtresiaDocument13 pagesBiliary AtresiaGündüz AğayevNo ratings yet
- Biliary CirrhosisDocument11 pagesBiliary CirrhosisradistryaNo ratings yet
- Cirrosis Biliar PrimariaDocument10 pagesCirrosis Biliar PrimariaGerardo CorreaNo ratings yet
- HSP WorkupDocument6 pagesHSP WorkupGiovanni SudargoNo ratings yet
- A Clinical View of Simple and Complex Renal CystsDocument3 pagesA Clinical View of Simple and Complex Renal CystsfernandonefNo ratings yet
- 1 s2.0 S187591812300034XDocument16 pages1 s2.0 S187591812300034Xhiếu caoNo ratings yet
- Abdominal ImagingDocument16 pagesAbdominal Imagingfrancu60No ratings yet
- Pancreatitits GallstonesDocument24 pagesPancreatitits Gallstonesheyiy20669No ratings yet
- Clinical Approach To Isolated Splenomegaly: M M, P M, R KDocument5 pagesClinical Approach To Isolated Splenomegaly: M M, P M, R KNida HanifaNo ratings yet
- Clinical Approach To Isolated Splenomegaly: M M, P M, R KDocument5 pagesClinical Approach To Isolated Splenomegaly: M M, P M, R KlilisNo ratings yet
- Acute Suppurative Cholangitis: Edward Chock, M.D., Bruce Wolfe, M.D., and Nathaniel Matolo, M.DDocument8 pagesAcute Suppurative Cholangitis: Edward Chock, M.D., Bruce Wolfe, M.D., and Nathaniel Matolo, M.DAhmad Harissul IbadNo ratings yet
- Incidence of Gallstone Disease and Complications (DANIEL MONSTED)Document9 pagesIncidence of Gallstone Disease and Complications (DANIEL MONSTED)abraham suarezNo ratings yet
- Cirrhosis of LiverDocument6 pagesCirrhosis of LiverBlackHAT GAMINGNo ratings yet
- Renal Path Lecture 3Document43 pagesRenal Path Lecture 3Sundar RamanathanNo ratings yet
- Clinico - Hematological Analysis of Pancytopenia: A Bone Marrow StudyDocument6 pagesClinico - Hematological Analysis of Pancytopenia: A Bone Marrow StudySrinath M VNo ratings yet
- Gastro Colopatia HTPDocument18 pagesGastro Colopatia HTPHernan Del CarpioNo ratings yet
- Pyogenic Liver AbscessDocument5 pagesPyogenic Liver AbscessPatcharaporn Fern KlongklaewNo ratings yet
- Torbenson 2018Document16 pagesTorbenson 2018Itzas SaLNo ratings yet
- Biliary Atresia: A Multidisciplinary Approach To Diagnosis and ManagementDocument15 pagesBiliary Atresia: A Multidisciplinary Approach To Diagnosis and ManagementAnne Lorraine BringasNo ratings yet
- 260-Article Text-875-1-10-20220728Document4 pages260-Article Text-875-1-10-20220728hasan andrianNo ratings yet
- Involucro Renal en Enf ReumatoideaDocument16 pagesInvolucro Renal en Enf ReumatoideaRodas LisNo ratings yet
- The (Fixed) Urinary Sediment, A Simple and Useful Diagnostic Hematuria - CellfixDocument6 pagesThe (Fixed) Urinary Sediment, A Simple and Useful Diagnostic Hematuria - CellfixTatiane FernandesNo ratings yet
- JGH 13174Document9 pagesJGH 13174samudraandiNo ratings yet
- Case Report: Streptococcus AnginosusDocument4 pagesCase Report: Streptococcus AnginosusIesanu MaraNo ratings yet
- Left SidedDocument3 pagesLeft SidedElisabeth ZzMick GtNo ratings yet
- Frequency of Hypersplenism in Chronic Liver Disease Patients Presenting With PancytopeniaDocument3 pagesFrequency of Hypersplenism in Chronic Liver Disease Patients Presenting With Pancytopeniaamal johnsonNo ratings yet
- Evaluation of Gross Hematuria: Cynthia G. Pan, MDDocument12 pagesEvaluation of Gross Hematuria: Cynthia G. Pan, MDRajarshi KumarNo ratings yet
- HematuriaDocument42 pagesHematuriaWasim R. IssaNo ratings yet
- Dysplasia & Multicystic KidneyDocument8 pagesDysplasia & Multicystic KidneyShintia MalindaNo ratings yet
- Dyson2018 1Document13 pagesDyson2018 1ManuelEduardoSanchezSotoNo ratings yet
- Cureus 0014 00000022733Document6 pagesCureus 0014 00000022733Dede IskandarNo ratings yet
- Thrombotic Microangiopathy, Hemolytic Uremic Syndrome, and Thrombotic Thrombocytopenic PurpuraDocument16 pagesThrombotic Microangiopathy, Hemolytic Uremic Syndrome, and Thrombotic Thrombocytopenic PurpuraDavidAlbertoMedinaMedinaNo ratings yet
- Prevalence of Anaemia in Decompensated Chronic Liver DiseaseDocument5 pagesPrevalence of Anaemia in Decompensated Chronic Liver DiseaseElang SudewaNo ratings yet
- Jessica Reid-Adam: Department of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NYDocument3 pagesJessica Reid-Adam: Department of Pediatrics, Icahn School of Medicine at Mount Sinai, New York, NYAnastasia Widha SylvianiNo ratings yet
- 8584-Article Text-31293-1-10-20110913Document5 pages8584-Article Text-31293-1-10-20110913Maksudur Rahman ShawonNo ratings yet
- Calciphylaxis Controversies in Pathogenesis, DiagDocument11 pagesCalciphylaxis Controversies in Pathogenesis, DiagJosh Jimenez RochaNo ratings yet
- YAMAMOTO 2016Document18 pagesYAMAMOTO 2016Bruno MoraesNo ratings yet
- Birkenfield 2014Document11 pagesBirkenfield 2014Bruno MoraesNo ratings yet
- Barsoum 2004Document13 pagesBarsoum 2004Bruno MoraesNo ratings yet
- Anandacoomarasamy 2007Document12 pagesAnandacoomarasamy 2007Bruno MoraesNo ratings yet
- CH 1Document31 pagesCH 1mustafa 1No ratings yet
- Hyponatremia in Tuberculous MeningitisDocument11 pagesHyponatremia in Tuberculous MeningitisBelinda Putri agustiaNo ratings yet
- Transport and Circulation in Plants and AnimalsDocument17 pagesTransport and Circulation in Plants and AnimalsTekomiNo ratings yet
- Miscellaneous: Eye, Ear, Skin, Pulmonary, Anti-Inflammatories & CancersDocument19 pagesMiscellaneous: Eye, Ear, Skin, Pulmonary, Anti-Inflammatories & CancersAbobakr AlobeidNo ratings yet
- Teaching Plan First Semester A.Y. 2020-2021: Indang, Cavite WWW - Cvsu.edu - PHDocument2 pagesTeaching Plan First Semester A.Y. 2020-2021: Indang, Cavite WWW - Cvsu.edu - PHYanis Emmanuelle LimNo ratings yet
- PHIL331 Exercise 3Document3 pagesPHIL331 Exercise 3Vishal P SubramaniamNo ratings yet
- Micro Teaching On Colitis: School of Nursing Science and Research Sharda UniversityDocument21 pagesMicro Teaching On Colitis: School of Nursing Science and Research Sharda UniversityPooja SahuNo ratings yet
- Downsyndrome 230411172734 b6391831Document32 pagesDownsyndrome 230411172734 b6391831dattamanasmita90No ratings yet
- Videbeck CH 1 Foundations of Psych Mental HealthDocument2 pagesVidebeck CH 1 Foundations of Psych Mental HealthFrank sweet IINo ratings yet
- Nle Practice Test CDocument12 pagesNle Practice Test CAr-jay JubaneNo ratings yet
- CHN Q&aDocument14 pagesCHN Q&aMonchikitowNo ratings yet
- Skills Math WorksheetDocument4 pagesSkills Math WorksheetBrennan MaguireNo ratings yet
- CHEST Journal - Single Article Antithrombotic Therapy For VTE Disease Antithrombotic Therapy For VTEDocument76 pagesCHEST Journal - Single Article Antithrombotic Therapy For VTE Disease Antithrombotic Therapy For VTEA. RaufNo ratings yet
- Best Practice in Therapeutic Drug MonitoringDocument6 pagesBest Practice in Therapeutic Drug MonitoringAnonymous hF5zAdvwCCNo ratings yet
- Family Nursing Care PlanDocument1 pageFamily Nursing Care PlanBhaby Che AserdnaNo ratings yet
- Medical AbbreviationsDocument5 pagesMedical AbbreviationsJumar RanasNo ratings yet
- Crisis InterventionDocument33 pagesCrisis Interventionaqsa randhawaNo ratings yet
- Republic Act - Intro To RTDocument8 pagesRepublic Act - Intro To RTRaniel SilimNo ratings yet
- Diabetes MellitusDocument26 pagesDiabetes MellitusPratiwi Lilapraba100% (2)
- Gynecologic Emergencies: Farhad Takhti M.D. Senior Consultant Landesklinikum Neunkirchen AustriaDocument52 pagesGynecologic Emergencies: Farhad Takhti M.D. Senior Consultant Landesklinikum Neunkirchen Austriamadmax500No ratings yet
- Anna Ostaszewska - Scientific Researches On Christian PsychotherapyDocument23 pagesAnna Ostaszewska - Scientific Researches On Christian Psychotherapysad1410No ratings yet
- PainDocument90 pagesPainmikErlh100% (4)
- HA Integument ChecklistDocument10 pagesHA Integument ChecklistMa Joanna Elizabeth S. PizarroNo ratings yet
- Management of Severe Peri Operative Bleeding .2Document79 pagesManagement of Severe Peri Operative Bleeding .2RobertaNo ratings yet
- Microsoft Word - Endodontic - MishapsDocument20 pagesMicrosoft Word - Endodontic - MishapsShufeiNo ratings yet
- Consent Advice Laparoscopic Tubal OcclusionDocument2 pagesConsent Advice Laparoscopic Tubal OcclusionKathJamesNo ratings yet
- 5 Hemolytic AnemiaDocument72 pages5 Hemolytic Anemiacoosa liquorsNo ratings yet
- Orofacial PainDocument7 pagesOrofacial PainAkram AlsharaeeNo ratings yet