Download as pdf or txt
You might also like
- On-Bottom Stability AnalysisDocument42 pagesOn-Bottom Stability AnalysisYoungtae Kim67% (3)
- CANON D450d, MF4300 Series Service ManualDocument182 pagesCANON D450d, MF4300 Series Service ManualJeepseadoo100% (2)
- Depression in Multiple Sclerosis PDFDocument11 pagesDepression in Multiple Sclerosis PDFalejandro bustamanteNo ratings yet
- Marcos NovakDocument21 pagesMarcos NovakArunagiri Kongu-UsecNo ratings yet
- Depression During The Menopausal Transition:: An Update On Epidemiology and Biological TreatmentsDocument6 pagesDepression During The Menopausal Transition:: An Update On Epidemiology and Biological TreatmentsTina MultazamiNo ratings yet
- Menstrual Cycle Effects On Psychological Symptoms in Women (2015)Document8 pagesMenstrual Cycle Effects On Psychological Symptoms in Women (2015)maria paula brenesNo ratings yet
- Articulo PsychoDocument8 pagesArticulo PsychoLaura AlfaroNo ratings yet
- Keller Et Al., 2012Document15 pagesKeller Et Al., 2012Dan SpitaruNo ratings yet
- Appi Ajp 2010 09050627Document8 pagesAppi Ajp 2010 09050627FebniNo ratings yet
- The Dexamethasone Suppression Test and Suicide Prediction: William Coryell, M.D. Michael Schlesser, M.DDocument6 pagesThe Dexamethasone Suppression Test and Suicide Prediction: William Coryell, M.D. Michael Schlesser, M.DAyu Annisa CharantiaNo ratings yet
- Rachel Yehuda Cortisol PTSD Policía BomberosDocument14 pagesRachel Yehuda Cortisol PTSD Policía BomberosPaulo GermanottaNo ratings yet
- A Meta-Analysis of Risk Factors For Post-Traumatic Stress Disorder (PTSD) in Adults and Children After EarthquakesDocument20 pagesA Meta-Analysis of Risk Factors For Post-Traumatic Stress Disorder (PTSD) in Adults and Children After EarthquakesHanifah NLNo ratings yet
- Depressive Symptoms After Breast Cancer Surgery Relationships With Global, Cancer-Related, and Life Event StressGOLDEN Y ANDERSENDocument12 pagesDepressive Symptoms After Breast Cancer Surgery Relationships With Global, Cancer-Related, and Life Event StressGOLDEN Y ANDERSENMary Belen Barria VillarroelNo ratings yet
- Antidepressant-Associated Chronic Irritable Dysphoria (ACID) in STEP-BD PatientsDocument6 pagesAntidepressant-Associated Chronic Irritable Dysphoria (ACID) in STEP-BD Patientseduardobar2000No ratings yet
- Research Article: Stresses and Disability in Depression Across GenderDocument9 pagesResearch Article: Stresses and Disability in Depression Across GenderWaleed RehmanNo ratings yet
- 19 Buttner2013 Article ExaminationOfPremenstrualSymptDocument7 pages19 Buttner2013 Article ExaminationOfPremenstrualSymptraja yasminNo ratings yet
- Otto 2004Document10 pagesOtto 2004Nurul Muqarribah Pratiwi IshaqNo ratings yet
- Bornheimer 2018Document9 pagesBornheimer 2018observacionfray23No ratings yet
- Discrimination, Perceived Control, and Psychological Health Among African Americans With HypertensionDocument11 pagesDiscrimination, Perceived Control, and Psychological Health Among African Americans With HypertensionBasriah IchankucingNo ratings yet
- Posttraumatic Psychopathology and The Pace of The Epigenetic Clock: A Longitudinal InvestigationDocument14 pagesPosttraumatic Psychopathology and The Pace of The Epigenetic Clock: A Longitudinal InvestigationzainNo ratings yet
- Marital Status and Risk For Late LifeDocument13 pagesMarital Status and Risk For Late LifeHargo PsyNo ratings yet
- Anxiety Disorders in WomenDocument52 pagesAnxiety Disorders in WomenZakkiyatus Zainiyah100% (1)
- Childhood Trauma and Basal Cortisol in People With Personality Disorders - ElsevierDocument4 pagesChildhood Trauma and Basal Cortisol in People With Personality Disorders - ElsevierGeander G. BachetiNo ratings yet
- Paul K. Maciejewski, Holly G. Prigerson and Carolyn M. Mazure Paul K. Maciejewski, Holly G. Prigerson and Carolyn M. MazureDocument6 pagesPaul K. Maciejewski, Holly G. Prigerson and Carolyn M. Mazure Paul K. Maciejewski, Holly G. Prigerson and Carolyn M. MazureMayra SouzaNo ratings yet
- Regular Articles: Causal Relationship Between Stressful Life Events and The Onset of Major DepressionDocument5 pagesRegular Articles: Causal Relationship Between Stressful Life Events and The Onset of Major DepressionTonytomazziNo ratings yet
- Kuehner 2016Document13 pagesKuehner 2016Claudio Angulo100% (1)
- Research Articles: Childhood Adversity and Vulnerability To Mood and Anxiety DisordersDocument7 pagesResearch Articles: Childhood Adversity and Vulnerability To Mood and Anxiety DisordersMifta 'hera' Khaerati IINo ratings yet
- Beesdo Baum2012Document15 pagesBeesdo Baum2012akzarajuwanaparastiaraNo ratings yet
- Romans 2012Document24 pagesRomans 2012Jeanne TorresNo ratings yet
- Menopause PDFDocument7 pagesMenopause PDFDenisa IonașcuNo ratings yet
- The Prevalence of Women Selected Rural Groups PMDDDocument12 pagesThe Prevalence of Women Selected Rural Groups PMDDRebecaNo ratings yet
- Brief Report: Trauma and Posttraumatic Stress Disorder in Treatment-Resistant Obsessive-Compulsive DisorderDocument3 pagesBrief Report: Trauma and Posttraumatic Stress Disorder in Treatment-Resistant Obsessive-Compulsive DisorderJuan Alberto GonzálezNo ratings yet
- Mood Disorders After TBIDocument17 pagesMood Disorders After TBIJaun CarrilloNo ratings yet
- Prevalen of DDocument8 pagesPrevalen of DĐỗ Văn ĐứcNo ratings yet
- Broadhead 1983Document17 pagesBroadhead 1983Laura ReyNo ratings yet
- Papers: Association Between Stressful Life Events and Exacerbation in Multiple Sclerosis: A Meta-AnalysisDocument5 pagesPapers: Association Between Stressful Life Events and Exacerbation in Multiple Sclerosis: A Meta-AnalysisALINENo ratings yet
- Prevalence of Psychiatric Disorders in Infertile Women and Men Undergoing in Vitro Fertilization TreatmentDocument8 pagesPrevalence of Psychiatric Disorders in Infertile Women and Men Undergoing in Vitro Fertilization TreatmentMaria Galia Elias QuirogaNo ratings yet
- Health Services Determinants of TheDocument6 pagesHealth Services Determinants of Theisra habibillahNo ratings yet
- Journal 2Document8 pagesJournal 2Ryan Drake RomeroNo ratings yet
- Enfermedad Autoinmune y DepresiónDocument13 pagesEnfermedad Autoinmune y Depresiónmaria cristina aravenaNo ratings yet
- Literature Review of PTSDDocument4 pagesLiterature Review of PTSDfvhj1y00100% (1)
- Biomarcadores en Suicidio 2020Document32 pagesBiomarcadores en Suicidio 2020siralkNo ratings yet
- Body Dissatisfaction and Mental HealthDocument9 pagesBody Dissatisfaction and Mental HealthBammy SiriratNo ratings yet
- Lamoureux Lamarche2017Document10 pagesLamoureux Lamarche2017Emanuel Santana OliveiraNo ratings yet
- 1 Prevalence and Psychosocial Factors of Anxiety andDocument11 pages1 Prevalence and Psychosocial Factors of Anxiety andNOOR SYAFAWATI HANUN MOHD SOBRINo ratings yet
- Prospective Study of Posttraumatic Stress Disorder and Depression Following TraumaDocument9 pagesProspective Study of Posttraumatic Stress Disorder and Depression Following TraumaSharon AdeleNo ratings yet
- Insomnia and Mental Health in College Students: Daniel J. TaylorDocument11 pagesInsomnia and Mental Health in College Students: Daniel J. TaylorAlfino SyahputraNo ratings yet
- A Systematic Review of The Mortality of DepressionDocument12 pagesA Systematic Review of The Mortality of Depressionadri90No ratings yet
- YBOCS AdultiDocument7 pagesYBOCS AdultiFabi kNo ratings yet
- McGrath, 2017Document16 pagesMcGrath, 2017Zeynep ÖzmeydanNo ratings yet
- Subthreshold Posttraumatic Stress Disord PDFDocument10 pagesSubthreshold Posttraumatic Stress Disord PDFJørgen CarlsenNo ratings yet
- Scales For ProdromeDocument15 pagesScales For Prodromedrkadiyala2No ratings yet
- Journal of Psychiatric Research: Niki Antypa, Marco Antonioli, Alessandro SerrettiDocument9 pagesJournal of Psychiatric Research: Niki Antypa, Marco Antonioli, Alessandro SerrettiDanielle DaniNo ratings yet
- Society of Behavioral MedicineDocument118 pagesSociety of Behavioral Medicineguroo_nanak0% (1)
- สัมนาาาDocument7 pagesสัมนาาาBook AmornwadeeNo ratings yet
- Posttraumatic Stress Disorder and Adherence To Medications in Survivors of Strokes and Transient Ischemic AttacksDocument7 pagesPosttraumatic Stress Disorder and Adherence To Medications in Survivors of Strokes and Transient Ischemic AttacksNicky Adi SaputraNo ratings yet
- Improving Our Understanding of Posttraumatic Trajectories: CommentaryDocument2 pagesImproving Our Understanding of Posttraumatic Trajectories: Commentaryericaduran4824No ratings yet
- Cg-Morbidity AjpDocument9 pagesCg-Morbidity AjpOfitamNo ratings yet
- AbortoDocument6 pagesAbortoS bmNo ratings yet
- Evaluation of Expressive Writing For Postpartum HealthDocument13 pagesEvaluation of Expressive Writing For Postpartum HealthIntan YNo ratings yet
- Guided Discontinuation Versus Maintenance Treatment in Remitted Firstepisode Psychosis Relapse Rates and Functional OutcomeDocument2 pagesGuided Discontinuation Versus Maintenance Treatment in Remitted Firstepisode Psychosis Relapse Rates and Functional Outcomewen zhangNo ratings yet
- Sexual Orientation and Psychodynamic Psychotherapy: Sexual Science and Clinical PracticeFrom EverandSexual Orientation and Psychodynamic Psychotherapy: Sexual Science and Clinical PracticeRating: 2 out of 5 stars2/5 (2)
- Clinical Handbook of Bereavement and Grief ReactionsFrom EverandClinical Handbook of Bereavement and Grief ReactionsEric BuiNo ratings yet
- CE023 LABORATORY MANUAL 2nd RevisionDocument72 pagesCE023 LABORATORY MANUAL 2nd RevisionernestNo ratings yet
- HydraulicsDocument190 pagesHydraulicsMathurathipan Rajendraseelan89% (9)
- Neko Bookmark: Designed by Jo NakashimaDocument4 pagesNeko Bookmark: Designed by Jo NakashimaEzra BlatzNo ratings yet
- KEW4105 ManualDocument19 pagesKEW4105 ManualYasuko Maulina ShigenoNo ratings yet
- Prof. S. Raman Sankaranarayanan (SRS), Assistant Professor, MMEDocument35 pagesProf. S. Raman Sankaranarayanan (SRS), Assistant Professor, MMESanjeev SahuNo ratings yet
- 3 Mundlak Cavallo y Domenech 1990Document25 pages3 Mundlak Cavallo y Domenech 1990Candela Vazquez FernándezNo ratings yet
- Media & Entertainment Collection BrochureDocument1 pageMedia & Entertainment Collection BrochureJulian Kene MbakweNo ratings yet
- Njex6300g (Sa) 11102003Document128 pagesNjex6300g (Sa) 11102003Marco A VelascoNo ratings yet
- AS-B Specification Sheet - SmartStruxure SolutionDocument12 pagesAS-B Specification Sheet - SmartStruxure SolutionOs ShNo ratings yet
- Types of SpeakersDocument5 pagesTypes of SpeakersDavid PeterNo ratings yet
- Quality: A. Quality: A Management PhilosophyDocument12 pagesQuality: A. Quality: A Management PhilosophyBehbehlynnNo ratings yet
- Friction Factor CalculationsDocument2 pagesFriction Factor CalculationsHu Hin AngNo ratings yet
- Automation 2 Topic 1: Design A Simple Process Control SystemDocument12 pagesAutomation 2 Topic 1: Design A Simple Process Control SystemChriscarl De LimaNo ratings yet
- Accurex, Model XXEW-10.0 Wall-Mounted Canopy Exhaust Hood Performance ReportDocument23 pagesAccurex, Model XXEW-10.0 Wall-Mounted Canopy Exhaust Hood Performance ReportProingmeca CANo ratings yet
- Eegame LogcatDocument42 pagesEegame LogcatKelvin AlexanderNo ratings yet
- Loci and Construction: NameDocument8 pagesLoci and Construction: Namecarolinethami13No ratings yet
- Rutland 914i Manual EDocument36 pagesRutland 914i Manual Egregoire de BrichambautNo ratings yet
- Datastage Errors and ResolutionDocument10 pagesDatastage Errors and Resolutionnithinmamidala999No ratings yet
- Designing Scenarios - Rebecca Wirfs-Brock PDFDocument8 pagesDesigning Scenarios - Rebecca Wirfs-Brock PDFAn Tran100% (1)
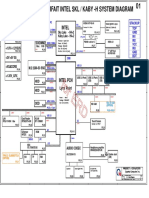
- Power Pavilion Parfait Intel SKL / Kaby - H System DiagramDocument52 pagesPower Pavilion Parfait Intel SKL / Kaby - H System DiagramAbnesis NesisNo ratings yet
- Waves: Laq'S (8 Marks)Document9 pagesWaves: Laq'S (8 Marks)Mohd ShahbazNo ratings yet
- Unsteady Thermotopography in Non-Destructive Testing: January 1976Document6 pagesUnsteady Thermotopography in Non-Destructive Testing: January 1976Ciprian LupuNo ratings yet
- Structural and Hydrological Design of Permeable PavementsDocument20 pagesStructural and Hydrological Design of Permeable Pavementssach1116No ratings yet
- Statistics Lesson Plan ImprovisedDocument7 pagesStatistics Lesson Plan ImprovisedShafiqah IsmailNo ratings yet
- Ge1x01 Engineering Graphics PDFDocument39 pagesGe1x01 Engineering Graphics PDFosmanNo ratings yet
- (Cambridge IISc Series) A. K. Nandakumaran, P. S. Datti - Partial Differential Equations - Classical Theory With A Modern Touch (Cambridge IISc Series) - Cambridge University Press (2020)Document377 pages(Cambridge IISc Series) A. K. Nandakumaran, P. S. Datti - Partial Differential Equations - Classical Theory With A Modern Touch (Cambridge IISc Series) - Cambridge University Press (2020)Rahul DevarakondaNo ratings yet