Download as pdf or txt
You might also like
- Fundamentals of Nursing Transes 1Document4 pagesFundamentals of Nursing Transes 1Louise Torres88% (8)
- Managing Urological Disorders in Multiple Sclerosis Patients: A Review of Available and Emerging TherapiesDocument9 pagesManaging Urological Disorders in Multiple Sclerosis Patients: A Review of Available and Emerging TherapiesRiccardo BientinesiNo ratings yet
- A Nationwide Epidemiological Study of Testicular Torsion in KoreaDocument4 pagesA Nationwide Epidemiological Study of Testicular Torsion in KoreaOttofianus Hewick KalangiNo ratings yet
- Perk Emi HanDocument11 pagesPerk Emi Handewi murdahNo ratings yet
- Akin Pelu FinalDocument7 pagesAkin Pelu FinalIdaamsiyatiNo ratings yet
- Faktor Risiko Hemoroid Korea NatureDocument9 pagesFaktor Risiko Hemoroid Korea NatureRatu AstridNo ratings yet
- Park 2013Document5 pagesPark 2013Soraia Rosa CoelhoNo ratings yet
- Burden, Pattern, Associated Factors and Impact On Quality of Life of Dermatological Disorders Among The Elderly in Ilala Municipality, Dar Es Salaam A Cross-Sectional StudyDocument10 pagesBurden, Pattern, Associated Factors and Impact On Quality of Life of Dermatological Disorders Among The Elderly in Ilala Municipality, Dar Es Salaam A Cross-Sectional StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Veterinary Journal: Craig I. Johnson, David J. Argyle, Dylan N. ClementsDocument10 pagesThe Veterinary Journal: Craig I. Johnson, David J. Argyle, Dylan N. ClementsMarNo ratings yet
- Prevalence of Functional Disability in Activities of Daily LivingDocument5 pagesPrevalence of Functional Disability in Activities of Daily LivingCarla PoletNo ratings yet
- Jamaophthalmology Kim 2021 Oi 200115 1618442148.38745Document7 pagesJamaophthalmology Kim 2021 Oi 200115 1618442148.38745Angelika Student1109No ratings yet
- Age and Sex Specific Reference Intervals For Blood Urea Nitrogen in Chinese General PopulationDocument7 pagesAge and Sex Specific Reference Intervals For Blood Urea Nitrogen in Chinese General PopulationVarna AmaliaNo ratings yet
- Nature AUS FLUS Deep Learning s41598-021-99622-0Document9 pagesNature AUS FLUS Deep Learning s41598-021-99622-0Mariana UsatiiNo ratings yet
- Ultrasound in The Etiological Assessment of Male Infertility: About 300 Cases at The Fertilia Medical Clinic in BamakoDocument5 pagesUltrasound in The Etiological Assessment of Male Infertility: About 300 Cases at The Fertilia Medical Clinic in BamakoIJAR JOURNALNo ratings yet
- InkontinentiaDocument6 pagesInkontinentiamahresyaNo ratings yet
- Candra Harmindasatya, Lenny Violetta Rosy SetiawatiDocument11 pagesCandra Harmindasatya, Lenny Violetta Rosy SetiawatiDr.gendjutNo ratings yet
- Vorland 1985Document7 pagesVorland 1985Angga RananggaNo ratings yet
- Faktor Risiko Terjadinya Osteoporosis Pada Wanita Menopause: Renidayati, Clara, SunardiDocument6 pagesFaktor Risiko Terjadinya Osteoporosis Pada Wanita Menopause: Renidayati, Clara, SunardiNoldin SirumpaNo ratings yet
- Article SLEintheelderly Rheumatol Int 2012Document6 pagesArticle SLEintheelderly Rheumatol Int 2012Jacqueline Vanessa Miranda SanabriaNo ratings yet
- Fendo 13 983180Document13 pagesFendo 13 983180Bekalu EndaleNo ratings yet
- Zumrutbas 2014Document7 pagesZumrutbas 2014drilaydacayNo ratings yet
- Deep Learning Model For Tongue Cancer Diagnosis UsDocument10 pagesDeep Learning Model For Tongue Cancer Diagnosis UsDaniel PancuNo ratings yet
- Anaemiaand Plasmodiasisamongchildrenbelowfiveyearsattending OPDat IshakaDocument13 pagesAnaemiaand Plasmodiasisamongchildrenbelowfiveyearsattending OPDat IshakaKIU PUBLICATION AND EXTENSIONNo ratings yet
- Rotator Cuff Tear - Prevalence of Symptomatic and Asymptomatic RCT in General PopulationDocument5 pagesRotator Cuff Tear - Prevalence of Symptomatic and Asymptomatic RCT in General Populationdimiz77No ratings yet
- Song 2013Document5 pagesSong 2013VioNo ratings yet
- Socio-Demographic Issues and Health-Related Quality of Life Among Inmates of A Correctional Center in Southwest NigeriaDocument5 pagesSocio-Demographic Issues and Health-Related Quality of Life Among Inmates of A Correctional Center in Southwest NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- ItaliaDocument6 pagesItaliaBandac AlexandraNo ratings yet
- Mine 1Document55 pagesMine 1emeNo ratings yet
- 2 Prevalence of Sarcopenia in Multi EthnicsDocument10 pages2 Prevalence of Sarcopenia in Multi EthnicsdavidtuanandartuaNo ratings yet
- The Abcs of Voiding Cystourethrography: Pictorial EssayDocument18 pagesThe Abcs of Voiding Cystourethrography: Pictorial EssayDaniel Mamani CruzNo ratings yet
- Demographic Profile, Clinical and Analysis of Osteoarthritis Patients in SurabayaDocument6 pagesDemographic Profile, Clinical and Analysis of Osteoarthritis Patients in SurabayaummuNo ratings yet
- 2019 INuJ. What Is The Effect of Body Mass Index On Subjective Outcome Following Vaginal Hysterectomy For ProlapseDocument9 pages2019 INuJ. What Is The Effect of Body Mass Index On Subjective Outcome Following Vaginal Hysterectomy For ProlapseJoseTeodomiroQuispeRicciNo ratings yet
- Fneur 13 853054Document8 pagesFneur 13 853054RAFAEL BRITONo ratings yet
- Quality of Life of Pediatric and Adult Individuals With Osteogenesis Imperfecta: A Meta-AnalysisDocument20 pagesQuality of Life of Pediatric and Adult Individuals With Osteogenesis Imperfecta: A Meta-AnalysisTimothy supitNo ratings yet
- Variations in Canthal Index of The IsokoDocument4 pagesVariations in Canthal Index of The IsokoHamza AkçayNo ratings yet
- Comorbidities and Risk Factors Associated With Insomnia in The Elderly PopulationDocument9 pagesComorbidities and Risk Factors Associated With Insomnia in The Elderly PopulationKhairunnisa Ayu KresnandaNo ratings yet
- Publication Prevalence of Anaemia2Document6 pagesPublication Prevalence of Anaemia2Samuel AdefemiNo ratings yet
- SCRIPTA SCORE Scientific Medical Journal Vol 2 No 1 OnlineDocument73 pagesSCRIPTA SCORE Scientific Medical Journal Vol 2 No 1 Online292Vien HardiyantiNo ratings yet
- GurbuzDocument8 pagesGurbuzDedi SaputraNo ratings yet
- 1 s2.0 S2468501118300129 MainDocument12 pages1 s2.0 S2468501118300129 MainBen DresimNo ratings yet
- KJFM 34 281Document8 pagesKJFM 34 281Dian AuliaNo ratings yet
- Article+0202 368 379Document12 pagesArticle+0202 368 379Muhammad Alif Nur FaizinNo ratings yet
- Characteristics of Leprosy Patients in Jakarta: Artikel PenelitianDocument5 pagesCharacteristics of Leprosy Patients in Jakarta: Artikel Penelitiandydy_7193No ratings yet
- Bmjopen 2023 077268Document11 pagesBmjopen 2023 077268Noella CHATUENo ratings yet
- Blood Research and DisordersDocument5 pagesBlood Research and Disordersdr_joe23No ratings yet
- Prevalence and Predictors of Geriatric Depression in Community-Dwelling ElderlyDocument9 pagesPrevalence and Predictors of Geriatric Depression in Community-Dwelling ElderlyArockia Berlin SoniaNo ratings yet
- Prevalence and Risk Factors For Lumbar Spondylosis and Its Association With Low Back Pain Among Rural Korean ResidentsDocument8 pagesPrevalence and Risk Factors For Lumbar Spondylosis and Its Association With Low Back Pain Among Rural Korean Residentsrizky septiNo ratings yet
- Membranous Nephropathy and Carbamazepine.20Document2 pagesMembranous Nephropathy and Carbamazepine.20muradchy321No ratings yet
- Prevalence of Erectile Dysfunction in Urology Consultation: A Prospective StudyDocument6 pagesPrevalence of Erectile Dysfunction in Urology Consultation: A Prospective StudyIJAR JOURNALNo ratings yet
- Factors of Independent of Activities of Daily Living Among Osteoarthritis ElderlyDocument7 pagesFactors of Independent of Activities of Daily Living Among Osteoarthritis ElderlyIJPHSNo ratings yet
- A Study On Surgical Management of Undescended TestDocument6 pagesA Study On Surgical Management of Undescended TestAhmed teroNo ratings yet
- EndometriosisDocument13 pagesEndometriosisDian NovitaNo ratings yet
- Menopause, Hormone Treatment and Urinary Incontinence at MidlifeDocument5 pagesMenopause, Hormone Treatment and Urinary Incontinence at MidlifeherryNo ratings yet
- Juvenile Granulosa Cell Tumor of The Testis PrenatDocument4 pagesJuvenile Granulosa Cell Tumor of The Testis PrenatPuspita MahardikaNo ratings yet
- 4 Jemds PDFDocument15 pages4 Jemds PDFMaría José Díaz RojasNo ratings yet
- (1479683X - European Journal of Endocrinology) Prevalence and Natural History of Adrenal IncidentalomasDocument13 pages(1479683X - European Journal of Endocrinology) Prevalence and Natural History of Adrenal IncidentalomasClaudiaNo ratings yet
- Jurnal Internasional Asuhan Keperawatan Gerontik Dengan DiareDocument13 pagesJurnal Internasional Asuhan Keperawatan Gerontik Dengan Diarefandhik setyawanNo ratings yet
- Endometriosis Pathogenesis, Clinical Impact and Management: Volume 9: Frontiers in Gynecological EndocrinologyFrom EverandEndometriosis Pathogenesis, Clinical Impact and Management: Volume 9: Frontiers in Gynecological EndocrinologyNo ratings yet
- Atlas of Inflammatory Bowel DiseasesFrom EverandAtlas of Inflammatory Bowel DiseasesWon Ho KimNo ratings yet
- Clinical Genetics and Genomics of AgingFrom EverandClinical Genetics and Genomics of AgingJuan Carlos Gomez-VerjanNo ratings yet
- NCM - 109 RLE Worksheet No. 4 Common Diagnostics - Laboratory and Nursing Procedures Related To Renal and Reproductive DisordersDocument10 pagesNCM - 109 RLE Worksheet No. 4 Common Diagnostics - Laboratory and Nursing Procedures Related To Renal and Reproductive DisorderskdfhjfhfNo ratings yet
- Bagian Kedua Tes Bahasa Inggris (Nomor 121 S.D. 180) Structure and Written ExpressionDocument5 pagesBagian Kedua Tes Bahasa Inggris (Nomor 121 S.D. 180) Structure and Written ExpressionFredy Allan SusantoNo ratings yet
- Elimination Pattern and Values-Beliefs PatternDocument2 pagesElimination Pattern and Values-Beliefs PatternYana DugayNo ratings yet
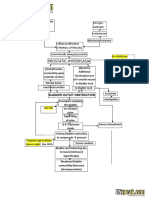
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDocument2 pagesBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailNo ratings yet
- Spinningbabies Daily Pelvic Floor ExercisesDocument1 pageSpinningbabies Daily Pelvic Floor ExercisesFederica FarfallaNo ratings yet
- Elimination Needs 04Document52 pagesElimination Needs 04Kishore RathoreNo ratings yet
- Comprehensive and Brief Icf Core Sets For Spinal Cord InjuryDocument14 pagesComprehensive and Brief Icf Core Sets For Spinal Cord InjuryAziz Ikhsan AshariNo ratings yet
- Corn SilkDocument1 pageCorn Silkwillyagung4557No ratings yet
- Bladder TrainingDocument3 pagesBladder TrainingJihan AisyNo ratings yet
- EvaluationDocument2 pagesEvaluationcarlos perez0% (1)
- Urinary Catheter: IndwellingDocument3 pagesUrinary Catheter: IndwellingKevinNo ratings yet
- Demo 2Document6 pagesDemo 2Justine VillaflorNo ratings yet
- Urinalysis: Dark Red, Cloudy Urine, PH: 7.0 SpecificDocument2 pagesUrinalysis: Dark Red, Cloudy Urine, PH: 7.0 SpecifichelloaNo ratings yet
- KistokelDocument4 pagesKistokelIntan PermataNo ratings yet
- Homeopathic Remedies For Kidney Stones - HompathDocument5 pagesHomeopathic Remedies For Kidney Stones - HompathBGNo ratings yet
- Students Individual Teaching PlanDocument2 pagesStudents Individual Teaching PlanNOEL YRIGONNo ratings yet
- EXAM 1 - Medical-Surgical Nursing Review Flashcards - QuizletDocument2 pagesEXAM 1 - Medical-Surgical Nursing Review Flashcards - QuizletErikaNo ratings yet
- Complicações Observadas em Cães e Gatos Com Doenças NeurológicasDocument13 pagesComplicações Observadas em Cães e Gatos Com Doenças NeurológicasDIEGO HENRIQUE DE MORAES TRIDICONo ratings yet
- Bowel IncontinenceDocument10 pagesBowel Incontinenceibrahim 12No ratings yet
- Persistent Cloaca Persistence of The ChallengeDocument7 pagesPersistent Cloaca Persistence of The ChallengekaremiaNo ratings yet
- UR Guidelines For Clinical Care Pathway 17.05.18Document31 pagesUR Guidelines For Clinical Care Pathway 17.05.18basamma kumbarNo ratings yet
- Uti Treatment PlanDocument3 pagesUti Treatment PlanbeatriceNo ratings yet
- Republic of The Philippines: (Formerly Naval State University)Document1 pageRepublic of The Philippines: (Formerly Naval State University)Maia Saivi OmegaNo ratings yet
- EliminationDocument128 pagesEliminationhailye mitikeNo ratings yet
- Vaginal Prolapse: by DR MutevheDocument32 pagesVaginal Prolapse: by DR MutevhedanielNo ratings yet
- Referat UtiDocument20 pagesReferat UtiYeni Rosa SitohangNo ratings yet
- Bbraun - Urimed-Vision-BrochureDocument2 pagesBbraun - Urimed-Vision-BrochureCampaign MediaNo ratings yet
- Urinary Catheterization ProcdureDocument9 pagesUrinary Catheterization ProcdureAkshata BansodeNo ratings yet
- Kidney Dissection Lab: EvaluationDocument4 pagesKidney Dissection Lab: EvaluationmauvegamNo ratings yet