Download as pdf or txt
You might also like
- TLE Hairdressing Grade 8 - 9Document25 pagesTLE Hairdressing Grade 8 - 9Roswlle50% (2)
- Doc-20240131-Wa0 240131 224112Document4 pagesDoc-20240131-Wa0 240131 22411222alhumidi2020No ratings yet
- BJA 2015 Via Aerea DificilDocument22 pagesBJA 2015 Via Aerea DificilAna Paula BoscatoNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsAnaMariaBustamanteNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsJhonatan LadinoNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsSans AndreasNo ratings yet
- Article ContentDocument10 pagesArticle ContentRicardo Muñoz PérezNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsrezaNo ratings yet
- Dif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsDocument22 pagesDif Ficult Airway Society 2015 Guidelines For Management of Unanticipated Dif Ficult Intubation in AdultsYael NepoNo ratings yet
- Vía Aerea DificilDocument22 pagesVía Aerea Dificilcoyotito961No ratings yet
- 10 1016@j Breast 2020 04 006Document9 pages10 1016@j Breast 2020 04 006Alberto AlexandruNo ratings yet
- Guía 2019 de Intubación y Extubación Francesa 2019Document7 pagesGuía 2019 de Intubación y Extubación Francesa 2019Rafael Edgar Aguilar Bandala ChaparrinNo ratings yet
- Weaning Francesas AICM 2019Document7 pagesWeaning Francesas AICM 2019Ana Miryam Pérez ZavalaNo ratings yet
- A Care Bundle Approach For Prevention of Ventilator-AssociatedDocument7 pagesA Care Bundle Approach For Prevention of Ventilator-AssociatedRestu Kusuma NingtyasNo ratings yet
- Knowledge and Practice Towards Care and MaintenancDocument7 pagesKnowledge and Practice Towards Care and MaintenancyunishaNo ratings yet
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- DN - Guidelines Related To Intravenous TherapyDocument10 pagesDN - Guidelines Related To Intravenous TherapyJoy Ce VeralloNo ratings yet
- Transport of The Critically Ill Patient PDFDocument4 pagesTransport of The Critically Ill Patient PDFaksinuNo ratings yet
- 10 1111@nin 12390Document14 pages10 1111@nin 12390YLA KATRINA BONILLANo ratings yet
- PDF - Hair Removal 2011Document7 pagesPDF - Hair Removal 2011Andira AzzahraNo ratings yet
- Jurnal 4Document8 pagesJurnal 4Adek AhmadNo ratings yet
- Teaching Plan Template - CareBundlesDocument9 pagesTeaching Plan Template - CareBundlesCris GalendezNo ratings yet
- 2021 Article 1347Document6 pages2021 Article 1347Rocio Ayaque AguirreNo ratings yet
- CVC Acceso 2020Document36 pagesCVC Acceso 2020Jose David Flores PérezNo ratings yet
- CVC AnesthesiaDocument36 pagesCVC AnesthesianadiaNo ratings yet
- Dolivet 2020Document6 pagesDolivet 2020Jasper RaelisonNo ratings yet
- HSR2 5 E649Document9 pagesHSR2 5 E649Samsul BahriNo ratings yet
- UIA 38 Safety PACUDocument5 pagesUIA 38 Safety PACUMelissa CadenaNo ratings yet
- Checklists - MultipleDocument6 pagesChecklists - MultipleDewi Ratna SariNo ratings yet
- Modifierad Clavien DindoDocument7 pagesModifierad Clavien DindoJonas LeoNo ratings yet
- ICU Burns GuidelineDocument24 pagesICU Burns GuidelineJonas BlaineNo ratings yet
- Chatterjee, 2022Document2 pagesChatterjee, 2022KatiusciaNo ratings yet
- Central or Peripheral Catheters For Initial Venous Access of ICU Patients: A Randomized Controlled TrialDocument8 pagesCentral or Peripheral Catheters For Initial Venous Access of ICU Patients: A Randomized Controlled TrialAndrés Fuica de la VegaNo ratings yet
- Anesthesia and Sedation Outside ofDocument9 pagesAnesthesia and Sedation Outside ofPutriRahayuMoidadyNo ratings yet
- Psu Nov 2020 - 1Document32 pagesPsu Nov 2020 - 1saphena parvaNo ratings yet
- Fluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconDocument12 pagesFluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconEllys Macías PeraltaNo ratings yet
- Tubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterDocument11 pagesTubes, Lines, and Drains Basics: Harmacy Ompetency Ssessment EnterJeremy HamptonNo ratings yet
- Principles of Monitoring Postoperative Patients PDFDocument3 pagesPrinciples of Monitoring Postoperative Patients PDFPaulo CesarNo ratings yet
- Algorythme Airway Difficile 2015 (DAS)Document22 pagesAlgorythme Airway Difficile 2015 (DAS)Cedric VaillesNo ratings yet
- Physiotherapy and Weaning From Prolonged Mechanical VentilationDocument9 pagesPhysiotherapy and Weaning From Prolonged Mechanical VentilationdanielNo ratings yet
- Raynak 2020Document17 pagesRaynak 2020javier rosales ortegaNo ratings yet
- 5 - General Considerations of Anesthesia and Management of The Difficult AirwayDocument27 pages5 - General Considerations of Anesthesia and Management of The Difficult AirwayMauricio Ruiz MoralesNo ratings yet
- Practice Guidelines For Central Venous Access 2020 An Updated Report by The American Society of Anesthesiologists Task Force On Central Venous Access PDFDocument36 pagesPractice Guidelines For Central Venous Access 2020 An Updated Report by The American Society of Anesthesiologists Task Force On Central Venous Access PDFDaniel Castro VeintimillaNo ratings yet
- Insertion Mangement Peripheral IVCannulaDocument20 pagesInsertion Mangement Peripheral IVCannulaAadil AadilNo ratings yet
- Level 1.5 Care BJHMDocument3 pagesLevel 1.5 Care BJHMhkw8g5snyxNo ratings yet
- Departmental Experience and Lessons Learned With Accelerated Introduction of Telemedicine During The COVID-19 CrisisDocument8 pagesDepartmental Experience and Lessons Learned With Accelerated Introduction of Telemedicine During The COVID-19 Crisistresy kalawaNo ratings yet
- Device Selection: Nancy L. Moureau and Evan AlexandrouDocument19 pagesDevice Selection: Nancy L. Moureau and Evan AlexandrouCarmen T OrtizNo ratings yet
- Multimodal PDFDocument11 pagesMultimodal PDFCarlos CahuayaNo ratings yet
- A Care Bundle For Pressure Ulcer Treatment inDocument8 pagesA Care Bundle For Pressure Ulcer Treatment inSuryo Prasetyo AjiNo ratings yet
- 6887 25815 1 PB PDFDocument7 pages6887 25815 1 PB PDFmochkurniawanNo ratings yet
- Risks of COVID-19 For Surgical Cancer Patients The Importance of The Informed Consent ProcessDocument3 pagesRisks of COVID-19 For Surgical Cancer Patients The Importance of The Informed Consent ProcessPablo Marques ReisNo ratings yet
- .A Retrosp Stu On The Long-Term Placem of Peripher Inse Central...Document6 pages.A Retrosp Stu On The Long-Term Placem of Peripher Inse Central...Ane MartinezNo ratings yet
- Journal of Taibah University Medical SciencesDocument9 pagesJournal of Taibah University Medical SciencesrobertoNo ratings yet
- Y. AL HashmiDocument11 pagesY. AL HashmiAzam alausyNo ratings yet
- Trauma Assessment Initial Trauma AssessmentDocument5 pagesTrauma Assessment Initial Trauma AssessmentzulfahNo ratings yet
- 2022 Respiron Ressecao Pulmonar Revisao Com MetanaliseDocument8 pages2022 Respiron Ressecao Pulmonar Revisao Com MetanaliseFrederico GarciaNo ratings yet
- A Systematic Review of Perioperative Clinical PracDocument10 pagesA Systematic Review of Perioperative Clinical PracBhavani VuppuNo ratings yet
- Idsa CapDocument46 pagesIdsa Capwalit ukhri mukrininNo ratings yet
- Chest Drains GuidanceDocument14 pagesChest Drains Guidancenob2011nobNo ratings yet
- IDSA Guideline PDFDocument80 pagesIDSA Guideline PDFArifHidayatNo ratings yet
- Doc-20240131-Wa0 240131 223939Document6 pagesDoc-20240131-Wa0 240131 22393922alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 223908Document5 pagesDoc-20240131-Wa0 240131 22390822alhumidi2020No ratings yet
- Wa0001.Document2 pagesWa0001.22alhumidi2020No ratings yet
- Gf7Khw4DSIS YocOA6iEcQ Word Parts Lecture Supplement Common RootsDocument1 pageGf7Khw4DSIS YocOA6iEcQ Word Parts Lecture Supplement Common Roots22alhumidi2020No ratings yet
- Priya Sharma A CorrectedDocument1 pagePriya Sharma A Corrected22alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 223819Document5 pagesDoc-20240131-Wa0 240131 22381922alhumidi2020No ratings yet
- Wa0008.Document1 pageWa0008.22alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 224157Document4 pagesDoc-20240131-Wa0 240131 22415722alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 223853Document5 pagesDoc-20240131-Wa0 240131 22385322alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 225101Document2 pagesDoc-20240131-Wa0 240131 22510122alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 224338Document3 pagesDoc-20240131-Wa0 240131 22433822alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 224425Document6 pagesDoc-20240131-Wa0 240131 22442522alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 225013Document2 pagesDoc-20240131-Wa0 240131 22501322alhumidi2020No ratings yet
- Doc-20240131-Wa0 240131 224810Document3 pagesDoc-20240131-Wa0 240131 22481022alhumidi2020No ratings yet
- Technogym Cat Skillrow Multi 20170522 UkDocument32 pagesTechnogym Cat Skillrow Multi 20170522 UkjoasNo ratings yet
- Id AssignmentDocument4 pagesId AssignmentAmutuhaire JudithNo ratings yet
- Minutes of 22,23,24 PRC - 1Document124 pagesMinutes of 22,23,24 PRC - 1M.Saleem100% (1)
- COVID ADVISORY NO. 25 - GUIDELINES ON THE REPATRIATION OF LOCALLY STRANDED INDIVIDUALS LSIs and Returning Overseas Filipinos ROFsDocument9 pagesCOVID ADVISORY NO. 25 - GUIDELINES ON THE REPATRIATION OF LOCALLY STRANDED INDIVIDUALS LSIs and Returning Overseas Filipinos ROFsAngelito CortunaNo ratings yet
- The Contours of Positive Human HealthDocument29 pagesThe Contours of Positive Human HealthSalvadorNo ratings yet
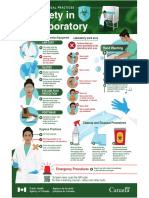
- Biosafety in The LaboratoryDocument1 pageBiosafety in The LaboratoryALFARO CHAT CARMINA ROSARIONo ratings yet
- Wordbank 15 Hospitals YoutubeDocument2 pagesWordbank 15 Hospitals YoutubeLIDYANo ratings yet
- Bone Tumors Radiology AssistanceDocument208 pagesBone Tumors Radiology Assistancemahmood khalifaNo ratings yet
- Annotated Bibliography MindfulnessDocument14 pagesAnnotated Bibliography Mindfulnessapi-255289819No ratings yet
- Homeroom Guidance: Quarter 3 - Module 14: The Responsible MeDocument13 pagesHomeroom Guidance: Quarter 3 - Module 14: The Responsible MeYOUR GUIDANCE COUNSELOR78% (23)
- Food Answers Food Answers: 8aa/8 8aa/8Document6 pagesFood Answers Food Answers: 8aa/8 8aa/8Helen100% (1)
- 2018 - Prevention and Treatment of Opioid Misuse and Addiction A ReviewDocument9 pages2018 - Prevention and Treatment of Opioid Misuse and Addiction A ReviewÂngela MarreiroNo ratings yet
- Nursing Services Manual, Aiims New Delhi - 25!2!21Document91 pagesNursing Services Manual, Aiims New Delhi - 25!2!21praveenjenaNo ratings yet
- Bartholin Gland Diseases 2Document13 pagesBartholin Gland Diseases 2gabriella azaliaNo ratings yet
- Young Star - One Pager - Version 1.4 - September 2021Document1 pageYoung Star - One Pager - Version 1.4 - September 2021ShihbNo ratings yet
- Wound Healing Activity of Ipomoea Batatas Tubers (Sweet Potato)Document14 pagesWound Healing Activity of Ipomoea Batatas Tubers (Sweet Potato)anggita ningratNo ratings yet
- 5 Step CultureSAFE CycleDocument1 page5 Step CultureSAFE CycleKhuda BukshNo ratings yet
- Icds N AayDocument8 pagesIcds N AayMeghan PaulNo ratings yet
- Comparison of Stainless Steel and Titanium Alloy Orthodontic Miniscrew Implants - A Mechanical and Histologic AnalysisDocument9 pagesComparison of Stainless Steel and Titanium Alloy Orthodontic Miniscrew Implants - A Mechanical and Histologic AnalysisDiego Andres Hincapie HerreraNo ratings yet
- Yours Uk 12 March 2023Document126 pagesYours Uk 12 March 2023turricanNo ratings yet
- Strength and Health 1937 09Document53 pagesStrength and Health 1937 09Vítor Faria Soares FerreiraNo ratings yet
- Development and Sensory Quality of Rice Base Candy Supplemented With Mushroom and Walnut FlourDocument6 pagesDevelopment and Sensory Quality of Rice Base Candy Supplemented With Mushroom and Walnut FlourInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Royal Free London NHS Foundation Trust: Nhs Standard Application FormDocument16 pagesRoyal Free London NHS Foundation Trust: Nhs Standard Application FormMatthew DalisayNo ratings yet
- Addiction: What Is Drug Dependence?Document3 pagesAddiction: What Is Drug Dependence?BRIDGETTE CANDACE FLORIDANo ratings yet
- Personal Values Questionnaire: InstructionsDocument6 pagesPersonal Values Questionnaire: InstructionsJust MeNo ratings yet
- Celiac Disease Management Through Gluten-Free DietsDocument13 pagesCeliac Disease Management Through Gluten-Free DietsbabaloseNo ratings yet
- Case Based 1 - Week 9Document3 pagesCase Based 1 - Week 9DharaNo ratings yet
- Chicago Tribune-26AprDocument37 pagesChicago Tribune-26AprvnaliniNo ratings yet
- Meat Technology 1Document30 pagesMeat Technology 1Rameen ShahidNo ratings yet