Download as pdf or txt
You might also like
- 00 Full Lewd Handbook (WIP)Document72 pages00 Full Lewd Handbook (WIP)Kacper Andrzejak50% (4)
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Electronic Fetal MonitoringDocument4 pagesElectronic Fetal MonitoringMauZungNo ratings yet
- The PartographDocument45 pagesThe PartographKimsha ConcepcionNo ratings yet
- Abnormal Cardiotohography in NewbornDocument37 pagesAbnormal Cardiotohography in NewbornAdityaRahaneNo ratings yet
- FETAL HEART TRACES 2.0 - CorrDocument9 pagesFETAL HEART TRACES 2.0 - CorrPatricia SmitNo ratings yet
- Cardiotopography (CTG)Document35 pagesCardiotopography (CTG)Jovian LutfiNo ratings yet
- CTG, Retensi UrineDocument51 pagesCTG, Retensi UrineMeriza ZulfaNo ratings yet
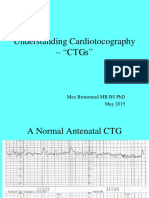
- Understanding Cardiotocography - "CTGS": Max Brinsmead MB Bs PHD May 2015Document29 pagesUnderstanding Cardiotocography - "CTGS": Max Brinsmead MB Bs PHD May 2015Irina NeamtuNo ratings yet
- Interpretation of Abnormal CTG Pattern - 2Document17 pagesInterpretation of Abnormal CTG Pattern - 2Jaspreet Kaur100% (1)
- Antenatal AssessmentDocument84 pagesAntenatal AssessmentRitbano AhmedNo ratings yet
- Intrapartum AssesmentDocument71 pagesIntrapartum AssesmentHusain ChherawalaNo ratings yet
- Ante Partum and Intra Partum Fetal MonitoringDocument63 pagesAnte Partum and Intra Partum Fetal MonitoringasdfNo ratings yet
- PartogramDocument30 pagesPartogramMuwanga faizoNo ratings yet
- Fetal SurveillanceDocument5 pagesFetal SurveillanceĶHwola ƏľsHokryNo ratings yet
- Abnormal Cardiotocography - "CTG"Document47 pagesAbnormal Cardiotocography - "CTG"Ahmad Mustaqim SulaimanNo ratings yet
- Fetal Monitoring: Dr. Anjoo Agarwal Professor Dept of Obs & Gyn KGMU, LucknowDocument30 pagesFetal Monitoring: Dr. Anjoo Agarwal Professor Dept of Obs & Gyn KGMU, LucknowMay MardiahNo ratings yet
- Intrapartum Fetal MonitoringDocument31 pagesIntrapartum Fetal Monitoringvk4bftgg2kNo ratings yet
- 2 Obg Seminar at NST J Inal (1) SSTDocument19 pages2 Obg Seminar at NST J Inal (1) SSTAmritaNo ratings yet
- Google - CTG InterpretationDocument43 pagesGoogle - CTG InterpretationOANo ratings yet
- Labor Assisted DeliveriesDocument8 pagesLabor Assisted Deliveriesnena marie evalaroza100% (1)
- OSCE OB - PDF Version 1Document15 pagesOSCE OB - PDF Version 1FNaF is love FNaF is lifeNo ratings yet
- Fetal Monitoring Orientation Day-1Document50 pagesFetal Monitoring Orientation Day-1Scott CalfeeNo ratings yet
- 01 胎兒監視器判讀及處置Document29 pages01 胎兒監視器判讀及處置金富力士No ratings yet
- Instruments and Medications in Labour Room & OtDocument40 pagesInstruments and Medications in Labour Room & OtIsaac TanNo ratings yet
- How To Read A CTGDocument31 pagesHow To Read A CTGAbdullah As'ad100% (1)
- NOTESsDocument5 pagesNOTESsAhmed Mohammed omarNo ratings yet
- Fetal Monitoring CTGDocument28 pagesFetal Monitoring CTGChuah Wei HongNo ratings yet
- Intrapartum Fetal AssessmentDocument52 pagesIntrapartum Fetal AssessmentAditya TejabaswaraNo ratings yet
- Partograph BoDocument60 pagesPartograph BoRendy Adhitya PratamaNo ratings yet
- CTG - Interpret With CareDocument55 pagesCTG - Interpret With CareKeeranmayeeishraNo ratings yet
- PartoghraphDocument60 pagesPartoghraphharley dela cruzNo ratings yet
- Uterine Hyperstimulation, Management of - ABMU Maternity Guideline 2018Document7 pagesUterine Hyperstimulation, Management of - ABMU Maternity Guideline 2018Chintya MarcellinNo ratings yet
- Partograph 160220134320Document43 pagesPartograph 160220134320amrutha pkNo ratings yet
- Partogram and CTG Reading Skills PDFDocument52 pagesPartogram and CTG Reading Skills PDFnurul nabillaNo ratings yet
- Partogram and CTG Reading Skills PDFDocument52 pagesPartogram and CTG Reading Skills PDFnurul nabillaNo ratings yet
- CTG ReportingDocument89 pagesCTG ReportingKevin Marcial AralarNo ratings yet
- 26 - Efm (CTG)Document25 pages26 - Efm (CTG)Abdelrahman ElsaadawiNo ratings yet
- Case Study 29-APHDocument31 pagesCase Study 29-APHZarul Naim Mohd TamiziNo ratings yet
- CTG Interpretation CmeDocument32 pagesCTG Interpretation CmeNurshawina KamaludinNo ratings yet
- Normal Delivery: Divisi Fetomaternal Departemen Obgin Fk-Usu/Rs. HamDocument83 pagesNormal Delivery: Divisi Fetomaternal Departemen Obgin Fk-Usu/Rs. HamenriNo ratings yet
- Normal Vs Abnormal Labour 2023Document52 pagesNormal Vs Abnormal Labour 2023Rohan Prem NairNo ratings yet
- 1835 FHR MonitoringDocument47 pages1835 FHR MonitoringjackNo ratings yet
- Partograph NextDocument50 pagesPartograph NextPrag GK Subedi0% (1)
- 2023 Labdiagnostic Proceduresm101Document60 pages2023 Labdiagnostic Proceduresm101Alezandra LabusNo ratings yet
- Fetal Distress Case DiscussionDocument55 pagesFetal Distress Case DiscussionHafsah G.No ratings yet
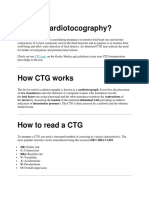
- What Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and UterineDocument18 pagesWhat Is Cardiotocography?: Cardiotocography (CTG) Is Used During Pregnancy To Monitor Fetal Heart Rate and Uterineمحمداحمد محمدنور ابايزيدNo ratings yet
- Antepartum-testing-1Document55 pagesAntepartum-testing-1kirton ricoNo ratings yet
- Chapter 14Document5 pagesChapter 14Kelly HeartsillNo ratings yet
- Nonstress TestDocument2 pagesNonstress TestMuskan rajNo ratings yet
- ObsNGyn - Abnormal Uterine Bleeding AtfDocument9 pagesObsNGyn - Abnormal Uterine Bleeding AtfarongeremewNo ratings yet
- Intrapartum Fetal Monitoring: Dalal AljarrahDocument44 pagesIntrapartum Fetal Monitoring: Dalal Aljarrahhacker ammerNo ratings yet
- Cardio To C OgraphyDocument6 pagesCardio To C OgraphyChinedu H. DuruNo ratings yet
- Antepartum Fetal SurveillanceDocument74 pagesAntepartum Fetal Surveillanceachala sahaiNo ratings yet
- Case 16Document3 pagesCase 16010527anwNo ratings yet
- Fetal SurvillanceDocument26 pagesFetal SurvillanceBetelhem EjiguNo ratings yet
- Assessment of Fetal WellbeingDocument24 pagesAssessment of Fetal WellbeingMukesh ThakurNo ratings yet
- CTGDocument21 pagesCTGAditya SahidNo ratings yet
- Abnormal Midwifery: by Gladys M. BSN, KRCHNDocument352 pagesAbnormal Midwifery: by Gladys M. BSN, KRCHNMercy KeruboNo ratings yet
- Government College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-IDocument6 pagesGovernment College of Nursing Jodhpur (Raj.) : Procedure On-Cordiotocography Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (1)
- Abnormal Midwifery1 1Document352 pagesAbnormal Midwifery1 1Mary AndrewNo ratings yet
- Anemia in PregnancyDocument22 pagesAnemia in Pregnancyosman nur100% (1)
- Jimma - BE Acceptance Letter 2022Document1 pageJimma - BE Acceptance Letter 2022osman nurNo ratings yet
- NUTRITIONDocument2 pagesNUTRITIONosman nurNo ratings yet
- 4 - PancreasDocument13 pages4 - Pancreasosman nurNo ratings yet
- Preeclampsia and EclampsiaDocument7 pagesPreeclampsia and Eclampsiaosman nurNo ratings yet
- Female Reproductive System Guided NotesDocument2 pagesFemale Reproductive System Guided NotesKevin HorneNo ratings yet
- Bibliography of AbortionDocument10 pagesBibliography of AbortioncherubrockNo ratings yet
- Alona Nutrition Across The LifespanDocument12 pagesAlona Nutrition Across The LifespanArmySapphireNo ratings yet
- PNC Case ProformaDocument7 pagesPNC Case ProformaKrishan38No ratings yet
- Adults, Elderly and Children Over 1 YearDocument7 pagesAdults, Elderly and Children Over 1 YeardindaikaputriNo ratings yet
- Contraception Chart SexualityDocument8 pagesContraception Chart SexualityRNStudent1No ratings yet
- Delivery Nursing Care PlanDocument6 pagesDelivery Nursing Care PlanKayelyn-Rose CombateNo ratings yet
- Jurnal DysmenorrheaDocument10 pagesJurnal Dysmenorrheaanisah tri agustiniNo ratings yet
- Abortion Full EssayDocument6 pagesAbortion Full EssayAlexander AndersonNo ratings yet
- Cognitive Behavioral Therapy For Perinatal Anxiety: A Randomized Controlled TrialDocument10 pagesCognitive Behavioral Therapy For Perinatal Anxiety: A Randomized Controlled TrialYenie YenNo ratings yet
- 026 - Protecting The Life and Health of Unborn ChildrenDocument18 pages026 - Protecting The Life and Health of Unborn ChildrenShakshi MehtaNo ratings yet
- Brittany Carter Final EnglishDocument11 pagesBrittany Carter Final Englishapi-582411411No ratings yet
- UnboundDocument1 pageUnboundMark Jefferson LunaNo ratings yet
- Culture Based Beliefs and Practices On Pregnancy and Childbirth Among Sorsoguenos Philippines PDFDocument11 pagesCulture Based Beliefs and Practices On Pregnancy and Childbirth Among Sorsoguenos Philippines PDFRazaCreciaLastrillaMenesesNo ratings yet
- SCIENCE Role of Hormone in Female and Male Reproductive SystemDocument8 pagesSCIENCE Role of Hormone in Female and Male Reproductive SystemJasmineNo ratings yet
- Human Sexuality PDFDocument215 pagesHuman Sexuality PDFPiruz Mollazadeh100% (2)
- The Endocrine GlandsDocument3 pagesThe Endocrine GlandsAshtua MandixNo ratings yet
- Nutrition (Micronutrients) in Child Growth and Development: A Systematic Review On Current Evidence, Recommendations and Opportunities For Further ResearchDocument15 pagesNutrition (Micronutrients) in Child Growth and Development: A Systematic Review On Current Evidence, Recommendations and Opportunities For Further ResearchRiley RilanNo ratings yet
- Assessment of Thyroid FunctionDocument7 pagesAssessment of Thyroid FunctionDewi Paramita YuniarahmiNo ratings yet
- Consent Checklist For Players.Document1 pageConsent Checklist For Players.Tiny DragonGirlNo ratings yet
- Chandrakant Development Friendly Wel Baby ClinicDocument4 pagesChandrakant Development Friendly Wel Baby Clinicapi-228136529No ratings yet
- 16 Reproduction Notes Igcse BiologyDocument29 pages16 Reproduction Notes Igcse Biologyasmatullahmohammed2No ratings yet
- WHO - Health Adolescents in VNDocument12 pagesWHO - Health Adolescents in VNNguyen Vu DoanNo ratings yet
- Understanding The SelfDocument13 pagesUnderstanding The SelfJillian NoreenNo ratings yet
- Debre Markos University Collage of Health ScienceDocument10 pagesDebre Markos University Collage of Health Sciencemengistu AddisNo ratings yet
- Law and Eco Final DraftDocument20 pagesLaw and Eco Final DraftlaishramjasonNo ratings yet
- FetalcirculationDocument32 pagesFetalcirculationannu panchalNo ratings yet
- Activity 1.1. Go OnlineDocument2 pagesActivity 1.1. Go OnlineToledo Cristine JadeNo ratings yet