Download as pdf or txt
You might also like
- Pharmacokinetics: A Refresher: Curtis L. Smith, Pharm.D., FCCP, BCPSDocument36 pagesPharmacokinetics: A Refresher: Curtis L. Smith, Pharm.D., FCCP, BCPSSyahrul Tuba Al Fatih100% (1)
- Telemetry-Intermediate Care Skills ChecklistDocument4 pagesTelemetry-Intermediate Care Skills ChecklistnorthweststaffingNo ratings yet
- Food Allergy Immunotherapy - Oral Immunotherapy andDocument10 pagesFood Allergy Immunotherapy - Oral Immunotherapy anda1765874No ratings yet
- Check Unit 555 November Immunology V3 PDFDocument25 pagesCheck Unit 555 November Immunology V3 PDFdragon66No ratings yet
- Alergia AlimentariaDocument18 pagesAlergia AlimentariaLUIS PARRANo ratings yet
- Abses PayudaraDocument18 pagesAbses Payudaragastro fkikunibNo ratings yet
- New Schatz2018 OldDocument44 pagesNew Schatz2018 Oldabhijeet abhijeetNo ratings yet
- Immunotherapy - What Lies BeyondDocument8 pagesImmunotherapy - What Lies BeyondSagar Das ChoudhuryNo ratings yet
- The Efficacy and Safety of Oral Immunotherapy For Food Allergies in Preschool-Aged ChildrenDocument10 pagesThe Efficacy and Safety of Oral Immunotherapy For Food Allergies in Preschool-Aged ChildrenIJAR JOURNALNo ratings yet
- Evidence That Food Proteins in Vaccines Cause The Development of Food Allergies and Its Implications For Vaccine Policy 2329 6631 1000137Document3 pagesEvidence That Food Proteins in Vaccines Cause The Development of Food Allergies and Its Implications For Vaccine Policy 2329 6631 1000137Engkiong GoNo ratings yet
- 1 s2.0 S002234762100977XDocument8 pages1 s2.0 S002234762100977XCarlos Luis Sarango ParralesNo ratings yet
- Adverse Reactions To Vaccines: Practice ParameterDocument14 pagesAdverse Reactions To Vaccines: Practice ParameterBrîndușa PetruțescuNo ratings yet
- Oral Tolerance, Food Allergy, and Immunotherapy: Implications For Future TreatmentDocument7 pagesOral Tolerance, Food Allergy, and Immunotherapy: Implications For Future TreatmentrigaNo ratings yet
- Nurmatov Et Al-2012-Cochrane Database of Systematic ReviewsDocument4 pagesNurmatov Et Al-2012-Cochrane Database of Systematic ReviewsfiskaderishaNo ratings yet
- Probiotics For The Prevention of Allergy A Systematic ReviewDocument10 pagesProbiotics For The Prevention of Allergy A Systematic ReviewadhyNo ratings yet
- Study of Food Allergy On Spanish Population: and M. PérezDocument9 pagesStudy of Food Allergy On Spanish Population: and M. PérezCrhistian Toribio DionicioNo ratings yet
- 2011 NIAIDSponsored 2010 Guidelines For Managing Food Allergy Applications in The Pediatric PopulationDocument13 pages2011 NIAIDSponsored 2010 Guidelines For Managing Food Allergy Applications in The Pediatric PopulationLily ChandraNo ratings yet
- Alergia e Anestesia COA2011Document6 pagesAlergia e Anestesia COA2011Maisa RibeiroNo ratings yet
- Prognostic Factors For Treatment Failure in Acute Otitis MediaDocument10 pagesPrognostic Factors For Treatment Failure in Acute Otitis MediaNaufal NanditaNo ratings yet
- HHS Public Access: Food Allergy: Immune Mechanisms, Diagnosis and ImmunotherapyDocument43 pagesHHS Public Access: Food Allergy: Immune Mechanisms, Diagnosis and ImmunotherapyLeonardo AzevedoNo ratings yet
- Case PresentationDocument12 pagesCase PresentationFrengky PrasetyaNo ratings yet
- Antibiotic Allergy in Pediatrics: A B A, B, C, D, e FDocument17 pagesAntibiotic Allergy in Pediatrics: A B A, B, C, D, e FВалерия НикитинаNo ratings yet
- Preclinik Safety StudiesDocument7 pagesPreclinik Safety StudiesLyn CitraNo ratings yet
- Schatz 2018Document44 pagesSchatz 2018abhijeet abhijeetNo ratings yet
- JURNAL READINGnejmoa1007174Document11 pagesJURNAL READINGnejmoa1007174Sukma WinahyuNo ratings yet
- New Schatz2018Document44 pagesNew Schatz2018abhijeet abhijeetNo ratings yet
- 1 s2.0 S0091674916306182 MainDocument9 pages1 s2.0 S0091674916306182 MainWahyu Ika WardhaniNo ratings yet
- 1 s2.0 S2213219817307420 MainDocument13 pages1 s2.0 S2213219817307420 MainJauza Raudhatul JannahNo ratings yet
- Alergia PrevencionDocument26 pagesAlergia PrevencionValeria Olarte ManjarresNo ratings yet
- Allergy - 2014 - Muraro - EAACI Food Allergy and Anaphylaxis Guidelines Diagnosis and Management of Food AllergyDocument18 pagesAllergy - 2014 - Muraro - EAACI Food Allergy and Anaphylaxis Guidelines Diagnosis and Management of Food AllergyCatherinavcuNo ratings yet
- High-Dose Versus Standard-Dose Amoxicillin/ Clavulanate For Clinically-Diagnosed Acute Bacterial Sinusitis: A Randomized Clinical TrialDocument15 pagesHigh-Dose Versus Standard-Dose Amoxicillin/ Clavulanate For Clinically-Diagnosed Acute Bacterial Sinusitis: A Randomized Clinical TrialHendra EfendiNo ratings yet
- Journal of The American Academy of Pediatrics, Valuing Reduced Antibiotic Use For OMADocument7 pagesJournal of The American Academy of Pediatrics, Valuing Reduced Antibiotic Use For OMARaymond PNo ratings yet
- Togias 2017Document16 pagesTogias 2017Jessica LópezNo ratings yet
- Food AlergyDocument11 pagesFood AlergyAhmad HafizyNo ratings yet
- Jurnal Reading AMRDocument49 pagesJurnal Reading AMRLoudry Amsal EGNo ratings yet
- JournalDocument10 pagesJournalRhea SaglesNo ratings yet
- HHS Public Access: Antibiotic AllergyDocument32 pagesHHS Public Access: Antibiotic AllergyInanda DamantiaNo ratings yet
- A Consensus Approach To The Primary Prevention 2021Document26 pagesA Consensus Approach To The Primary Prevention 2021Pam Travezani MiyazakiNo ratings yet
- GARGANO 2021 Food Allergy and Intolerance A Narrative Review OnDocument35 pagesGARGANO 2021 Food Allergy and Intolerance A Narrative Review OnCristiane HermesNo ratings yet
- For Sept-Aug Food AllergiesDocument15 pagesFor Sept-Aug Food AllergiesJakeJohengenNo ratings yet
- Antibiotik Rasional Pada Demam TifoidDocument35 pagesAntibiotik Rasional Pada Demam TifoidSelvi SulistianingsihNo ratings yet
- Dangerous Liaisons Bacteria Antimicrobial Therapies and Allergic DiseasesDocument16 pagesDangerous Liaisons Bacteria Antimicrobial Therapies and Allergic DiseasesValeria GamboaNo ratings yet
- Sublingual ImmunotherapyDocument4 pagesSublingual ImmunotherapyAnonymous eZqDZbObRiNo ratings yet
- Andosan™-An Anti-Allergic and Anti-Inflammatory Ingredient Prepared From Agaricus Blazei MushroomDocument11 pagesAndosan™-An Anti-Allergic and Anti-Inflammatory Ingredient Prepared From Agaricus Blazei MushroomMartinaNo ratings yet
- Jama Shenoy 2019 RV 180010Document12 pagesJama Shenoy 2019 RV 180010GustavoCalderinNo ratings yet
- Cernadas-2013-Pediatric Allergy and ImmunologyDocument7 pagesCernadas-2013-Pediatric Allergy and ImmunologyMoisés PonceNo ratings yet
- REFERAT Anak TasiaDocument15 pagesREFERAT Anak TasiaAnastasia PasaribuNo ratings yet
- Jurnal Alergi KacangDocument12 pagesJurnal Alergi Kacangvirginia putri karinaNo ratings yet
- Lemone/Burke/Bauldoff/Gubrud, Medical-Surgical Nursing 6Th Edition Test BankDocument43 pagesLemone/Burke/Bauldoff/Gubrud, Medical-Surgical Nursing 6Th Edition Test Banknurse homeNo ratings yet
- Alergias y MicrobiotaDocument12 pagesAlergias y MicrobiotaVictoria LopezNo ratings yet
- Swine Disease TreatementDocument12 pagesSwine Disease TreatementM NNo ratings yet
- Contoh UTBK SoshumDocument6 pagesContoh UTBK SoshumsalshabilaNo ratings yet
- Probiotics in Late Infancy Reduce The Incidence of Eczema: A Randomized Controlled TrialDocument6 pagesProbiotics in Late Infancy Reduce The Incidence of Eczema: A Randomized Controlled TrialarditaNo ratings yet
- Mullin 2010Document9 pagesMullin 2010Alfred AlfredNo ratings yet
- 10 36516-Jocass 1246401-2933495Document5 pages10 36516-Jocass 1246401-2933495yyyyx842No ratings yet
- Risk Multipliers For Severe Food Anaphylaxis: JournalDocument6 pagesRisk Multipliers For Severe Food Anaphylaxis: JournalAngga Aryo LukmantoNo ratings yet
- 1 s2.0 S1939455122000631 MainDocument25 pages1 s2.0 S1939455122000631 MainWilliam Rolando Miranda ZamoraNo ratings yet
- Impétigo Revisión SistemáticaDocument21 pagesImpétigo Revisión SistemáticaDanielNo ratings yet
- A Network-Based Approach For Identifying Suitable Biomarkers For Oral Immunotherapy of Food AllergyDocument11 pagesA Network-Based Approach For Identifying Suitable Biomarkers For Oral Immunotherapy of Food AllergyTalhaTariqNo ratings yet
- Kontou 2017Document5 pagesKontou 2017María Cristina RomanoNo ratings yet
- Sublingual Immunotherapy For Peanut Allergy: A Randomized, Double-Blind, Placebo-Controlled Multicenter TrialDocument16 pagesSublingual Immunotherapy For Peanut Allergy: A Randomized, Double-Blind, Placebo-Controlled Multicenter TrialSzakacs AlexandruNo ratings yet
- Pediatric Food Allergy: A Clinical GuideFrom EverandPediatric Food Allergy: A Clinical GuideRuchi S. GuptaNo ratings yet
- Lecture 11 Sedative-Hypnotic and Anti-Anxiety AgentsDocument32 pagesLecture 11 Sedative-Hypnotic and Anti-Anxiety AgentsHafsa ShakilNo ratings yet
- Biopsia Endoscopica Guiada Por UsDocument12 pagesBiopsia Endoscopica Guiada Por UsDavidNo ratings yet
- Half Life & BioavailabilityDocument12 pagesHalf Life & Bioavailabilitydavid5king-3119No ratings yet
- Week 9 Lecture 1 Brachytherapy Radiation Protection1Document41 pagesWeek 9 Lecture 1 Brachytherapy Radiation Protection1Mark RoldanNo ratings yet
- Adhd MedicationsDocument2 pagesAdhd MedicationsSupreet Singh MalhiNo ratings yet
- Pharmacogenomics DDI and DDGIDocument39 pagesPharmacogenomics DDI and DDGIMarfu'ah Mar'ahNo ratings yet
- Module No. 1 Administration of MedicationDocument7 pagesModule No. 1 Administration of Medicationerica nclsNo ratings yet
- Anti Diabetic DrugsDocument54 pagesAnti Diabetic Drugsmanj99No ratings yet
- Weight Loss - The Formoline L112 Advantages: Lipid Adsorbent ToDocument2 pagesWeight Loss - The Formoline L112 Advantages: Lipid Adsorbent ToALMUBARAKMSNo ratings yet
- CV of Khrisna Joy AutencioDocument3 pagesCV of Khrisna Joy AutenciokhrisnaNo ratings yet
- Linfoma de Hodgkin: Enfermedad en Relapso/RecaídaDocument31 pagesLinfoma de Hodgkin: Enfermedad en Relapso/RecaídaDANIEL JAIR ENRIQUEZ VERANo ratings yet
- Drugs MaltaDocument564 pagesDrugs MaltaHesbon Momanyi100% (1)
- Chapter 15 Vocab AP PsychDocument2 pagesChapter 15 Vocab AP PsychTylerNo ratings yet
- Katzung End of Chapter Questions-ModifiedDocument110 pagesKatzung End of Chapter Questions-ModifiedLicensed to Heal0% (1)
- Consent For Diagnostic And/or Therapeutic ParacentesisDocument2 pagesConsent For Diagnostic And/or Therapeutic ParacentesisnaveenNo ratings yet
- 93 M Deatials PDFDocument5 pages93 M Deatials PDFRatna RoesardhyatiNo ratings yet
- Stok Barang Saat Ini: Nama Barang Saldo Barang GD HNA Total QtyDocument33 pagesStok Barang Saat Ini: Nama Barang Saldo Barang GD HNA Total Qtyfitra dewiNo ratings yet
- SE JAN 21 For Sir LouieDocument15 pagesSE JAN 21 For Sir LouieEdna Uneta RoblesNo ratings yet
- US Transdermal Patch Market Outlook 2020Document11 pagesUS Transdermal Patch Market Outlook 2020Neeraj ChawlaNo ratings yet
- Paket APP, HERNIA Dan WIDE (Ada Harga Per Tindakan)Document54 pagesPaket APP, HERNIA Dan WIDE (Ada Harga Per Tindakan)Bagus TriagungNo ratings yet
- PNF Manual For Primary Healthcare PDFDocument317 pagesPNF Manual For Primary Healthcare PDFtej0331No ratings yet
- Perhitungan Dosis Resep A, B, C, DDocument9 pagesPerhitungan Dosis Resep A, B, C, Drindy tika lestariNo ratings yet
- Drug Education Gr.1Document8 pagesDrug Education Gr.1Hennie Ziah CalceñaNo ratings yet
- Daftar Obat-Obatan Yang Dibutuhkan: Forumen Tetes TelingaDocument3 pagesDaftar Obat-Obatan Yang Dibutuhkan: Forumen Tetes TelingaPutu 'yayuk' Widyani WiradiraniNo ratings yet
- Glossary of Common Industry AbbreviationsDocument7 pagesGlossary of Common Industry AbbreviationsVarun KhannaNo ratings yet
- About Psychiatric Drugs Side-EffectsDocument60 pagesAbout Psychiatric Drugs Side-EffectsKarthikeyan Sudarsana BabuNo ratings yet
- My Published Paper 6, AnesthesiaDocument5 pagesMy Published Paper 6, Anesthesiamir sahirNo ratings yet
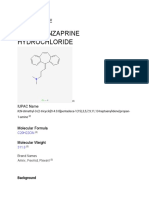
- Cyclobenzaprine Hydrochloride: Drug ProfileDocument13 pagesCyclobenzaprine Hydrochloride: Drug ProfileShruti ThakurNo ratings yet