Download as pdf or txt
You might also like
- NCM 116 - Git (Module 5)Document15 pagesNCM 116 - Git (Module 5)Meryville Jacildo100% (1)
- Gastrointestinal System Disorders - MedSurg NursingDocument56 pagesGastrointestinal System Disorders - MedSurg NursingJermaine S. TeodoroNo ratings yet
- The Digestive SystemDocument26 pagesThe Digestive SystemJasmin RubioNo ratings yet
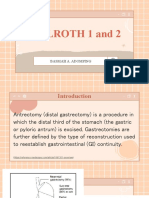
- Billroth 1 and 2: Basmah A. AdompingDocument31 pagesBillroth 1 and 2: Basmah A. AdompingBasmah A. AdompingNo ratings yet
- Types of EnemaDocument6 pagesTypes of EnemaOmprakash Saini100% (2)
- Unit 9 Notes - Digestive SystemDocument68 pagesUnit 9 Notes - Digestive Systemshrilpatel2001No ratings yet
- Anaphy FinalsDocument20 pagesAnaphy FinalsHazel Anne Dela CruzNo ratings yet
- 9 GitDocument81 pages9 GitAbdurahman Tainy100% (1)
- ANAPHY DigestiveDocument20 pagesANAPHY DigestiveStefanie SantillaNo ratings yet
- The Digestive SystemDocument1 pageThe Digestive SystemAlexa VeraNo ratings yet
- Anat 25 GItract EDocument10 pagesAnat 25 GItract EAnonymous H0JCjweaQANo ratings yet
- Digestive SystemDocument114 pagesDigestive SystemAj MirandaNo ratings yet
- The Gastric Phase of The Integrated Response To A MealDocument12 pagesThe Gastric Phase of The Integrated Response To A MealpuchioNo ratings yet
- Large Intestine.: © L N - A & P II (A. I) D P1 8Document8 pagesLarge Intestine.: © L N - A & P II (A. I) D P1 8Naveen EldoseNo ratings yet
- RT 204 Prefinal TransesDocument22 pagesRT 204 Prefinal TransesLouise0% (1)
- Digestive System 2022-23Document28 pagesDigestive System 2022-23Fady Fady100% (1)
- Outline: Relative Measurements of Alimentary TractsDocument9 pagesOutline: Relative Measurements of Alimentary TractsProfessor GhoulNo ratings yet
- MetabolismDocument3 pagesMetabolismElsie CarbonNo ratings yet
- Physiology of DigestionDocument14 pagesPhysiology of DigestionMalti SharmaNo ratings yet
- Digestive System NotesDocument7 pagesDigestive System NotesasiyeskierNo ratings yet
- Abdul MananDocument2 pagesAbdul MananscribdNo ratings yet
- Anatomy and PhysiologyDocument13 pagesAnatomy and PhysiologyUday Kumar100% (1)
- Gastro 4Document537 pagesGastro 4Andrei ManeaNo ratings yet
- Gastrointestinal System: Page 1 of 4Document4 pagesGastrointestinal System: Page 1 of 4Shivani SriramNo ratings yet
- Digestion & AbsorptionDocument13 pagesDigestion & AbsorptionU Than HanNo ratings yet
- Digestive SystemDocument2 pagesDigestive SystemRashid DayaoNo ratings yet
- Bio 241 Katz-Keenan Unit 5 - Chapter 17: Digestive System Learning Outcomes: 17.1 General Characteristics of The Digestive SystemDocument33 pagesBio 241 Katz-Keenan Unit 5 - Chapter 17: Digestive System Learning Outcomes: 17.1 General Characteristics of The Digestive SystemBree OGLETREENo ratings yet
- Topic 6. Digestive SystemDocument27 pagesTopic 6. Digestive SystemNicolas EstradaNo ratings yet
- Study Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesDocument10 pagesStudy Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesKc Cabanilla LizardoNo ratings yet
- Gastrointestinal Tract 2: The Structure and Function of The StomachDocument5 pagesGastrointestinal Tract 2: The Structure and Function of The Stomachvanessa wijayaNo ratings yet
- Week 7Document7 pagesWeek 7Darylle Hannah De GuzmanNo ratings yet
- 12 DigestiveDocument5 pages12 DigestiveDaniellaRuth Cajurao CanalesNo ratings yet
- Chap - 05 - LIFE PROCESSESS - Holozoic Nutrition - Compressed - CompressedDocument5 pagesChap - 05 - LIFE PROCESSESS - Holozoic Nutrition - Compressed - Compressedsujatalam1921No ratings yet
- C - Other SystemsDocument29 pagesC - Other SystemsVũ Xuân MinhNo ratings yet
- The Digestive System Handouts GENBIO2 STEM12Document4 pagesThe Digestive System Handouts GENBIO2 STEM12April Joy T. GrijaldoNo ratings yet
- Unit IV - Digestive and Excretory SystemDocument54 pagesUnit IV - Digestive and Excretory SystemsahilNo ratings yet
- 12DIGESTIVEDocument5 pages12DIGESTIVEDaniellaRuth Cajurao CanalesNo ratings yet
- 6 CH25 General Anatomy & Digestive Processes & Mouth To Esophagus 2015Document32 pages6 CH25 General Anatomy & Digestive Processes & Mouth To Esophagus 2015AbdullionNo ratings yet
- Lec Activity16-And-17 Digestive SystemDocument8 pagesLec Activity16-And-17 Digestive SystemYda Maxine PalmaNo ratings yet
- Digestive System Anatomy and Physiology - NurseslabsDocument33 pagesDigestive System Anatomy and Physiology - NurseslabsMari FeNo ratings yet
- JHS Digestive SystemDocument35 pagesJHS Digestive SystemGojo KaisenNo ratings yet
- Digestive System ContinuationDocument38 pagesDigestive System ContinuationLocal ClownNo ratings yet
- Digestive System - Mahti Ahsan: Juristat September 2015Document3 pagesDigestive System - Mahti Ahsan: Juristat September 2015Kr VishalNo ratings yet
- DigestiveDocument5 pagesDigestiveadrianmanansala3360No ratings yet
- Vile Parle Shri Kelavani Mandal's C.N.M.School & N.D.Parekh Pre-Primary School Biology - Study Sheet - STD Viii (2021-22) Digestive SystemDocument5 pagesVile Parle Shri Kelavani Mandal's C.N.M.School & N.D.Parekh Pre-Primary School Biology - Study Sheet - STD Viii (2021-22) Digestive SystemUploaded 2103No ratings yet
- The Digestive SystemDocument10 pagesThe Digestive Systemofurumchinyere9No ratings yet
- Gastrointestinal Physiology: Department of Physiology CHS, UniosunDocument59 pagesGastrointestinal Physiology: Department of Physiology CHS, UniosunTeeNo ratings yet
- Chapter 24: The Digestive SystemDocument4 pagesChapter 24: The Digestive SystemTHÂN TÂM VUI KHOẺNo ratings yet
- THE Disgestive System: by Second GroupDocument17 pagesTHE Disgestive System: by Second GroupAuliya AlfaNo ratings yet
- Drugs Acting On The Gastrointestinal (Gi) System Digestive SystemDocument6 pagesDrugs Acting On The Gastrointestinal (Gi) System Digestive SystemAdiel CalsaNo ratings yet
- Medtech Git Upper and LowerDocument72 pagesMedtech Git Upper and LowerBabe YamonganNo ratings yet
- The Digestive System: S.Kep, NS., M.KepDocument10 pagesThe Digestive System: S.Kep, NS., M.KepAuliya AlfaNo ratings yet
- NCMB 316 M1 Cu1Document23 pagesNCMB 316 M1 Cu1Maica Lectana100% (1)
- Gastrointestinal SystemDocument21 pagesGastrointestinal Systemsayan27.sikdarNo ratings yet
- Ahp Ut4Document83 pagesAhp Ut4jeniferNo ratings yet
- All About GIT PhysiologyDocument79 pagesAll About GIT PhysiologySherwan R Shal91% (23)
- Diseases of The Mouth and Related StructuresDocument333 pagesDiseases of The Mouth and Related StructuresAmisalu NigusieNo ratings yet
- Wardlaws Perspectives in Nutrition A Functional Approach 1St Edition Byrd Bredbenner Solutions Manual Full Chapter PDFDocument36 pagesWardlaws Perspectives in Nutrition A Functional Approach 1St Edition Byrd Bredbenner Solutions Manual Full Chapter PDFcharles.osborne574100% (11)
- The Digestive SystemDocument45 pagesThe Digestive SystemgwormtalaveraNo ratings yet
- Definition of TermsDocument3 pagesDefinition of TermsJoanne Sianson BucayanNo ratings yet
- Chapter 06Document47 pagesChapter 06gayathmipereraNo ratings yet
- Non Perforated Peptic Ulcer Disease, Multidetector CT Finding, Complication, and Differential DiagnosisDocument15 pagesNon Perforated Peptic Ulcer Disease, Multidetector CT Finding, Complication, and Differential DiagnosisIndra PrimaNo ratings yet
- GCP - Anatomy and PhysiologyDocument4 pagesGCP - Anatomy and PhysiologyKrishelle Kate PannigNo ratings yet
- Postpyloric Feeding Access in Infants And.4Document7 pagesPostpyloric Feeding Access in Infants And.4Yazmin TorresNo ratings yet
- Digestive System Parts and FunctionsDocument3 pagesDigestive System Parts and Functionsshindou ai67% (3)
- Drenaj EndoscopicDocument20 pagesDrenaj EndoscopicLivia GudacNo ratings yet
- Nutrition in Animals Class 7 Science Notes - Chapter 2: Different Ways of Taking FoodDocument4 pagesNutrition in Animals Class 7 Science Notes - Chapter 2: Different Ways of Taking FoodVikrant Deshmukh100% (1)
- Gall Bladder & Pancreas HistologyDocument48 pagesGall Bladder & Pancreas HistologyGood BoyNo ratings yet
- 8A Food and DigestionDocument20 pages8A Food and DigestionPoornimaNo ratings yet
- Digestive SystemDocument6 pagesDigestive SystemDorence SimuntalaNo ratings yet
- Pitfalls of BCLC-2Document2 pagesPitfalls of BCLC-2saikrishhNo ratings yet
- Introduction Abdomen DR 130818235819 Phpapp02Document11 pagesIntroduction Abdomen DR 130818235819 Phpapp02Namrata GabaNo ratings yet
- Gastrointestinal Drugs 26269Document10 pagesGastrointestinal Drugs 26269Elena CondicNo ratings yet
- Cirugía BariátricaDocument7 pagesCirugía BariátricalicgenaroNo ratings yet
- Digestive System WorksheetsDocument3 pagesDigestive System Worksheetsapi-258634162100% (1)
- Mindmap PBL 4 GI - Raisa Zalfa Meutia Abubakar - 1906317865Document1 pageMindmap PBL 4 GI - Raisa Zalfa Meutia Abubakar - 1906317865Raisa ZalfaNo ratings yet
- Detailed Lesson Plan in Science 8Document9 pagesDetailed Lesson Plan in Science 8Jerlan Tambola100% (1)
- Test Bank For Paramedic Care Principles and Practice Vols 1 5 5th Edition Bryan e Bledsoe Robert S Porter Richard A CherryDocument18 pagesTest Bank For Paramedic Care Principles and Practice Vols 1 5 5th Edition Bryan e Bledsoe Robert S Porter Richard A CherryStephanieMoorefiat100% (43)
- InSure ONE Instructions For UseDocument2 pagesInSure ONE Instructions For UseJaja DavidNo ratings yet
- Understanding Medical Surgical Nursing - 0843-0843Document1 pageUnderstanding Medical Surgical Nursing - 0843-0843Anas TasyaNo ratings yet
- Curriculum Vitae: Professor René AdamDocument4 pagesCurriculum Vitae: Professor René AdamdoctorNo ratings yet
- Laparoscopic CholecystectomyDocument100 pagesLaparoscopic CholecystectomyRakshay Kaul100% (1)
- Small IntestineDocument2 pagesSmall Intestineiron100% (1)
- Structural Organisation in AnimalsDocument7 pagesStructural Organisation in Animalszoombs1223No ratings yet
- Ulcerative ColitisDocument12 pagesUlcerative Colitisquidditch07No ratings yet
- Sistem Pencernaan 231019Document19 pagesSistem Pencernaan 231019Exan KurniawanNo ratings yet
- Agricultural Sciences Grade 12 2020 JIT Term1 1Document60 pagesAgricultural Sciences Grade 12 2020 JIT Term1 1malatjikagiso168No ratings yet
- Gastric and Duodenal UlcerDocument56 pagesGastric and Duodenal UlcerMatthew MckenzieNo ratings yet
- Embriologi GastroDocument50 pagesEmbriologi GastroYeni100% (1)