Download as pdf or txt
You might also like
- English For Pharmacists - 25, 67, 79, 110, 127 PDFDocument5 pagesEnglish For Pharmacists - 25, 67, 79, 110, 127 PDFJosé Henríquez GalánNo ratings yet
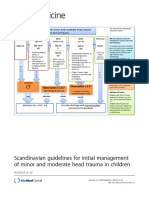
- Scandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenDocument20 pagesScandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenRafael Mujica OreNo ratings yet
- Tirado-Bsn 4d-Journal Summary and ReflectionDocument3 pagesTirado-Bsn 4d-Journal Summary and ReflectionJeniper Marie Cute29No ratings yet
- Art 10.1186 - 1757 7241 22 20Document5 pagesArt 10.1186 - 1757 7241 22 20Ahmad Tri Anggara SasmitaNo ratings yet
- ЧМТР 11 1Document3 pagesЧМТР 11 1Iryna ZapekaNo ratings yet
- Epidemiology of Head Injury - A Level 1 Taei Centre StudyDocument2 pagesEpidemiology of Head Injury - A Level 1 Taei Centre StudyIJAR JOURNALNo ratings yet
- Pediatric GuidelineDocument13 pagesPediatric GuidelineAi NurfaiziyahNo ratings yet
- Management of Traumatic Brain Injury PatientsDocument14 pagesManagement of Traumatic Brain Injury Patientsyayaslaras96No ratings yet
- Assessing The Severity of Traumatic Brain Injury-Time For A Change?Document12 pagesAssessing The Severity of Traumatic Brain Injury-Time For A Change?Anonymous R6ex8BM0No ratings yet
- Assess The Traumatic Brain Injury Outcomes in Pakistani Emergency DepartmentDocument27 pagesAssess The Traumatic Brain Injury Outcomes in Pakistani Emergency DepartmentsanamaqsoodmalikNo ratings yet
- Management and Outcome of Traumatic Epidural Hematoma in 41 Infants and Children From A Single CenterDocument7 pagesManagement and Outcome of Traumatic Epidural Hematoma in 41 Infants and Children From A Single CenterMariska JuanitaNo ratings yet
- Prognostic Factors For Relapse and Outcome in Pediatric Acute Transverse MyelitisDocument11 pagesPrognostic Factors For Relapse and Outcome in Pediatric Acute Transverse Myelitisyusak sampeNo ratings yet
- Multidetector CT in ChildrenDocument21 pagesMultidetector CT in Childrenpaquidermo85No ratings yet
- Citicoline in Severe Traumatic Brain Injury: Indications For Improved OutcomeDocument8 pagesCiticoline in Severe Traumatic Brain Injury: Indications For Improved OutcomeMira TamilaNo ratings yet
- Tce 2020 LibanoDocument11 pagesTce 2020 LibanoLaura ScottNo ratings yet
- Perioperative Management of The Pediatric Patient With Traumatic Brain InjuryDocument14 pagesPerioperative Management of The Pediatric Patient With Traumatic Brain InjuryBaha MirzaeifarNo ratings yet
- Article BI Knowledge Grid Support For Treatment of Traumatic Brain Injury VictimsDocument10 pagesArticle BI Knowledge Grid Support For Treatment of Traumatic Brain Injury VictimsjlkazadiNo ratings yet
- Nihms 1921257Document119 pagesNihms 1921257ja.arenas904pfizerNo ratings yet
- Medicine: Incidence of Hydrocephalus in Traumatic Brain InjuryDocument8 pagesMedicine: Incidence of Hydrocephalus in Traumatic Brain Injury相壮壮No ratings yet
- 2019 - Kang - Does A Mobile App Improve Patients'Document9 pages2019 - Kang - Does A Mobile App Improve Patients'Warsi MaryatiNo ratings yet
- Pediatric Head Trauma: A Review and Update: Practice GapsDocument16 pagesPediatric Head Trauma: A Review and Update: Practice GapsnadiaNo ratings yet
- Journal 6Document9 pagesJournal 6yustinasusantisokaNo ratings yet
- Risk Factors For and The Role of Dental Extractions in Osteoradionecrosis of The Jaws: A National-Based Cohort StudyDocument9 pagesRisk Factors For and The Role of Dental Extractions in Osteoradionecrosis of The Jaws: A National-Based Cohort Studyita mustainahNo ratings yet
- Research: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryDocument8 pagesResearch: CATCH: A Clinical Decision Rule For The Use of Computed Tomography in Children With Minor Head InjuryCarlos Martin Yafac RiscoNo ratings yet
- Diagnostics 12 02541 With CoverDocument20 pagesDiagnostics 12 02541 With CoverasadprlNo ratings yet
- Differences in Radiation Dose For Computed Tomography of The Brain Among Pediatric Patients at The Emergency Departments: An Observational StudyDocument10 pagesDifferences in Radiation Dose For Computed Tomography of The Brain Among Pediatric Patients at The Emergency Departments: An Observational StudyHamza ArjahNo ratings yet
- TSNC - F Cognitivas SubrayadoDocument8 pagesTSNC - F Cognitivas SubrayadoEus CádizNo ratings yet
- Pattern of Traumatic Head Injury in Makurdi, North Central Nigeria: Accident and Emergency ExperienceDocument9 pagesPattern of Traumatic Head Injury in Makurdi, North Central Nigeria: Accident and Emergency ExperienceMhmdzlkfli 12No ratings yet
- SJAMS 66 2563 2566 C PDFDocument4 pagesSJAMS 66 2563 2566 C PDFVitta Kusma WijayaNo ratings yet
- ARTG - 2022 - Long-Term Outcomes of Patients With Primary Brain Tumors After Acute RehabilitationDocument11 pagesARTG - 2022 - Long-Term Outcomes of Patients With Primary Brain Tumors After Acute RehabilitationSM199021No ratings yet
- Stroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item GenerationDocument8 pagesStroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item Generationandi kurniawanNo ratings yet
- Sudanese ResearchDocument11 pagesSudanese Researchhassanabdullah0777No ratings yet
- Children 09 01560Document9 pagesChildren 09 01560Susana MartinezNo ratings yet
- Optimization of Cutting Fluid Using VIKOR MethodDocument9 pagesOptimization of Cutting Fluid Using VIKOR MethodEditor IJTSRDNo ratings yet
- European Journal of Radiology: M Kiani, A ChaparianDocument7 pagesEuropean Journal of Radiology: M Kiani, A ChaparianHamza ArjahNo ratings yet
- Paediatric Neck MassesDocument7 pagesPaediatric Neck MassesGiovanni HenryNo ratings yet
- Lancent BrainDocument62 pagesLancent BrainAdriana SerratoNo ratings yet
- Volumetric and Morphometric MRI Findings in Patients With Mild Traumatic Brain InjuryDocument10 pagesVolumetric and Morphometric MRI Findings in Patients With Mild Traumatic Brain Injuryrhegi isdiara FairuzNo ratings yet
- Article 1Document7 pagesArticle 1gogih64190No ratings yet
- Symptoms in Primary Care With Time To Diagnosis of Brain TumoursDocument8 pagesSymptoms in Primary Care With Time To Diagnosis of Brain TumoursHILA GINANo ratings yet
- Thrombolysis in Pediatric Stroke Study: Special ReportDocument19 pagesThrombolysis in Pediatric Stroke Study: Special ReportErick DjuandaNo ratings yet
- Tec Pediatrico ActualizacionDocument11 pagesTec Pediatrico ActualizacionDarelys LopezNo ratings yet
- Flaherty 2016Document6 pagesFlaherty 2016Diornald MogiNo ratings yet
- Management of Traumatic Brain Injury (TBI) - A Clinical Neuroscience-Led Pathway For The NHSDocument8 pagesManagement of Traumatic Brain Injury (TBI) - A Clinical Neuroscience-Led Pathway For The NHS彭金辉 KIVINo ratings yet
- JurnalDocument7 pagesJurnalskocabzzNo ratings yet
- Manejo de Tce Severo en PediatriaDocument14 pagesManejo de Tce Severo en PediatriaAlejandro LaraNo ratings yet
- Management of Concussion and Mild Traumatic Brain Injury: A Synthesis of Practice GuidelinesDocument12 pagesManagement of Concussion and Mild Traumatic Brain Injury: A Synthesis of Practice GuidelinesKomangNo ratings yet
- 2020 Article 712Document8 pages2020 Article 712Agrinto TaloimNo ratings yet
- Literature Review Brain InjuryDocument8 pagesLiterature Review Brain Injuryafdtwudac100% (1)
- Ashina2020 Article EfficacyTolerabilityAndSafetyODocument9 pagesAshina2020 Article EfficacyTolerabilityAndSafetyOFirjatullahNo ratings yet
- Medip, IJCMPH-5398 ODocument6 pagesMedip, IJCMPH-5398 OAlpasca FirdausNo ratings yet
- Traumatic BrainDocument6 pagesTraumatic Brainmutia nur rahmiNo ratings yet
- Severe Traumatic Brain Injury Targeted Management in The Intensive Care UnitDocument24 pagesSevere Traumatic Brain Injury Targeted Management in The Intensive Care UnitJuan Sebastian Rodriguez GarciaNo ratings yet
- Guidelines For Neuroprognostication in Adults With Traumatic Spinal Cord InjuryDocument23 pagesGuidelines For Neuroprognostication in Adults With Traumatic Spinal Cord Injurymarius vaidaNo ratings yet
- Management of Mild and Moderate Head Injuries in Adults: Dana Turliuc, A. CucuDocument11 pagesManagement of Mild and Moderate Head Injuries in Adults: Dana Turliuc, A. CucuSarrah Kusuma DewiNo ratings yet
- Prehospital Care of Traumatic Brain InjuryDocument6 pagesPrehospital Care of Traumatic Brain Injuryaffa_lechyNo ratings yet
- Delaroche 2016Document21 pagesDelaroche 2016Erick DjuandaNo ratings yet
- A Machine Learning Model For Predicting Favorable Outcome in Severe Traumatic Brain Injury Patients After 6 MonthsDocument8 pagesA Machine Learning Model For Predicting Favorable Outcome in Severe Traumatic Brain Injury Patients After 6 MonthsRashellya RasyidaNo ratings yet
- (19330693 - Journal of Neurosurgery) Estimating The Global Incidence of Traumatic Brain InjuryDocument18 pages(19330693 - Journal of Neurosurgery) Estimating The Global Incidence of Traumatic Brain InjuryIqra AlghifarihNo ratings yet
- 0068KJR - KJR 23 343Document12 pages0068KJR - KJR 23 343Yulita MustikasariNo ratings yet
- Diagnostic Imaging in Head and Neck CancerFrom EverandDiagnostic Imaging in Head and Neck CancerHiroya OjiriNo ratings yet
- AlzheimerDocument9 pagesAlzheimerbruno lopez lucasNo ratings yet
- Micro Buzz Words - KEY WordsDocument8 pagesMicro Buzz Words - KEY WordsKris GulleyNo ratings yet
- Silodosin 1Document7 pagesSilodosin 1Akhmad MustafaNo ratings yet
- Quick Guide - Antenatal Care NHSDocument28 pagesQuick Guide - Antenatal Care NHSLimfc UfscNo ratings yet
- Neonatal Resuscitation DrugsDocument4 pagesNeonatal Resuscitation Drugsblast2111No ratings yet
- Nursing Research and Clinical Update Post Test (Responses) - Form Responses 1Document6 pagesNursing Research and Clinical Update Post Test (Responses) - Form Responses 1Indah PermatasariNo ratings yet
- Curriculum Vita DR - Mousa 3Document7 pagesCurriculum Vita DR - Mousa 3Mostafa OmranNo ratings yet
- Hospital and Healthcare FacilitiesDocument23 pagesHospital and Healthcare FacilitiesGueanne ConsolacionNo ratings yet
- Cology MCQDocument4 pagesCology MCQHemant BaraiNo ratings yet
- The Reliability and Validity of A Brief Diabetes Knowledge TestDocument5 pagesThe Reliability and Validity of A Brief Diabetes Knowledge TestIonela BărbosNo ratings yet
- Burns Summary of EvidenceDocument23 pagesBurns Summary of EvidenceYudhaNo ratings yet
- Hamilton Depression Rating Scale (HDRS)Document2 pagesHamilton Depression Rating Scale (HDRS)Rian Candra Ibrahim100% (1)
- Hearing LossDocument18 pagesHearing LossYaska MusaNo ratings yet
- Module 6Document4 pagesModule 6Leah LlobellNo ratings yet
- Chest Guidelines - WarfarinDocument41 pagesChest Guidelines - Warfarinkedaw100% (1)
- Sheet - Respiratory ExaminationDocument11 pagesSheet - Respiratory ExaminationbakesamiNo ratings yet
- Volume 15, Number 1 January 2011Document233 pagesVolume 15, Number 1 January 2011Nicolai BabaliciNo ratings yet
- Lab ReportDocument1 pageLab ReportNishantNo ratings yet
- Jurnal Internasional 55 PDFDocument5 pagesJurnal Internasional 55 PDFPutri UtamiNo ratings yet
- Identicifation of Hookworm Species in Stool by Harada Mori CultureDocument2 pagesIdenticifation of Hookworm Species in Stool by Harada Mori CultureMeenachi ChidambaramNo ratings yet
- Comparison Between Manual Procedure and Automated For Determinant of Wbcs and PCV in Maternity and Labor Hospital in Karbala CityDocument3 pagesComparison Between Manual Procedure and Automated For Determinant of Wbcs and PCV in Maternity and Labor Hospital in Karbala Cityyousrazeidan1979No ratings yet
- Side Effect Information: Post Vaccine Dose #2 of Moderna VaccineDocument1 pageSide Effect Information: Post Vaccine Dose #2 of Moderna VaccineLiza PreissNo ratings yet
- Chapter 09 RespiratoryDocument3 pagesChapter 09 RespiratoryBernard Paul Guinto0% (2)
- Notice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Document12 pagesNotice: Meetings: Recognized Standards List Modifications (Recognition List Number 018)Justia.comNo ratings yet
- Vital Signs ScriptDocument2 pagesVital Signs ScriptRed Angela Dinson100% (1)
- Ulceration and Ulcers: Ulceration - Is The Cellular Death of Superficial Tissue Leading ToDocument4 pagesUlceration and Ulcers: Ulceration - Is The Cellular Death of Superficial Tissue Leading ToAshref BelhajNo ratings yet
- Thieme E-Journals - Seminars in Neurology - Full TextDocument1 pageThieme E-Journals - Seminars in Neurology - Full TextLeandro SebastianNo ratings yet
- Capella Workout Club Indemnity FormDocument2 pagesCapella Workout Club Indemnity FormbrussellwkNo ratings yet
- Implementation of The AntiDocument13 pagesImplementation of The AntiFirst NameNo ratings yet