Download as pdf or txt
You might also like
- Thoracic WallDocument87 pagesThoracic WallAuza Moses IbrahimNo ratings yet
- Null 2Document34 pagesNull 2Esdras DountioNo ratings yet
- 2 PleuraDocument28 pages2 Pleuradrshubhamvyas.08No ratings yet
- Thoracic Diaphragm Group-TDocument42 pagesThoracic Diaphragm Group-TVivev JatNo ratings yet
- Chest Wall, Pelural Cavity, LungDocument48 pagesChest Wall, Pelural Cavity, LungKizuna Hiki-kunNo ratings yet
- Chest WallDocument26 pagesChest WallDeepti KakkarNo ratings yet
- Diaphragm, Suprapleural and Endothoracic Fascia: Lecturer Radiology M Shah ZebDocument17 pagesDiaphragm, Suprapleural and Endothoracic Fascia: Lecturer Radiology M Shah ZebShimmering MoonNo ratings yet
- Anatomy of Thoracic Wall & Pleura-DikonversiDocument69 pagesAnatomy of Thoracic Wall & Pleura-DikonversiFira TasyaNo ratings yet
- Diaphragm, Intercostal Muscles and Muscles of The Vertebral ColumnDocument30 pagesDiaphragm, Intercostal Muscles and Muscles of The Vertebral Columnsamthomasvarghese2019No ratings yet
- LUNGSDocument43 pagesLUNGSelliot kafumukacheNo ratings yet
- 14 - Intercostal SpaceDocument33 pages14 - Intercostal SpaceVandana RaviNo ratings yet
- The Thoracic CageDocument35 pagesThe Thoracic Cagehananabodeaf41No ratings yet
- Anatomy (Respiratory)Document63 pagesAnatomy (Respiratory)moazamaakbarNo ratings yet
- Null 4Document47 pagesNull 4Kenyan MillanNo ratings yet
- Anatomy of Thoracic WallDocument27 pagesAnatomy of Thoracic WallSamuel Pola Karta Sembiring100% (1)
- THORAX Complete 200LDocument193 pagesTHORAX Complete 200Layomideolaniran14No ratings yet
- Anatomy Week 3 NotesDocument32 pagesAnatomy Week 3 NotesBasil AdeelNo ratings yet
- Anatomy I: by Dr. Ziyad M. Al Zeer Orthopedic Surgeon MD - PHDDocument36 pagesAnatomy I: by Dr. Ziyad M. Al Zeer Orthopedic Surgeon MD - PHDMOHAMMAD ALSWEITYNo ratings yet
- Notes On The Thorax: Anatomy RHS 241Document71 pagesNotes On The Thorax: Anatomy RHS 241William JonathanNo ratings yet
- Thoracic Cage and Wall: Dr. Afdal, Spa, M. BiomedDocument62 pagesThoracic Cage and Wall: Dr. Afdal, Spa, M. Biomedadhima indriNo ratings yet
- The Thorax Part Ii - The Thoracic Cavity: Juan Guido G. Joyo, PTRP Juvi G. Alicabo, PTRP, CCP, CTMBP, CTTTPDocument98 pagesThe Thorax Part Ii - The Thoracic Cavity: Juan Guido G. Joyo, PTRP Juvi G. Alicabo, PTRP, CCP, CTMBP, CTTTPFerjie Angelica DalandaoNo ratings yet
- Structure of Chest, Dr. Hasan Nyambe PDFDocument45 pagesStructure of Chest, Dr. Hasan Nyambe PDFAndi Meidin AnugerahNo ratings yet
- DiaphragmDocument18 pagesDiaphragmAuza Moses IbrahimNo ratings yet
- Muscles of The Thoracic Wall, Pectoral Region - 2023 - 1Document28 pagesMuscles of The Thoracic Wall, Pectoral Region - 2023 - 1202112360No ratings yet
- Chest Cavity.Document29 pagesChest Cavity.Shimmering MoonNo ratings yet
- Thoracic WallDocument117 pagesThoracic WallKAYISIRE EMERYNo ratings yet
- Posterior MediastinumDocument121 pagesPosterior MediastinumAuza Moses IbrahimNo ratings yet
- Sternum OsteologyDocument34 pagesSternum OsteologyRohit SahNo ratings yet
- Abdominal WallDocument56 pagesAbdominal WallTanaka ChadambukaNo ratings yet
- Anatomy of ThoraxDocument68 pagesAnatomy of Thoraxangela marie abadillaNo ratings yet
- Diaphragm: Mr. Abdur Rehman BS-cardiology Kmu-IpmsDocument19 pagesDiaphragm: Mr. Abdur Rehman BS-cardiology Kmu-IpmsAbdurrehman SafiNo ratings yet
- DiaphragmDocument22 pagesDiaphragmcollinsmagNo ratings yet
- Share '1579792243522 - Lecture 2Document21 pagesShare '1579792243522 - Lecture 2MOHAMMAD ALSWEITYNo ratings yet
- ThoraxDocument29 pagesThoraxapi-249972919No ratings yet
- Part 1 RespDocument21 pagesPart 1 RespBishal JB KunworNo ratings yet
- H.A Assessing Thorax and LungsDocument68 pagesH.A Assessing Thorax and LungsMc Ramil B. Pradero100% (1)
- Anatomy of DiaphragmDocument21 pagesAnatomy of DiaphragmEniola abdullahi AduagbaNo ratings yet
- Thoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دDocument18 pagesThoracic cavity & contents: Thorax Unit Lecture 3 & 4 مسعلأا ليلج رديح .دMuhammad UsmanNo ratings yet
- Prof. Ghabisha Saif Posterior Abdominal Wall AnatomyDocument36 pagesProf. Ghabisha Saif Posterior Abdominal Wall AnatomyAzizNo ratings yet
- Abdominal WallDocument56 pagesAbdominal WallAHMAD KHANNo ratings yet
- The DiaphramDocument30 pagesThe DiaphramKAYISIRE EMERYNo ratings yet
- L5 Surface Anatomy & DiaphragmDocument45 pagesL5 Surface Anatomy & DiaphragmatefmoussaNo ratings yet
- Anatomy of The LarynxDocument37 pagesAnatomy of The LarynxAftab Khalil100% (1)
- 8 MediastinumDocument30 pages8 MediastinumAuza Moses Ibrahim100% (2)
- General Anatomy 4 Thoracic Cavity: Dr. Wesam BaderDocument46 pagesGeneral Anatomy 4 Thoracic Cavity: Dr. Wesam BaderAhmadNo ratings yet
- Thoracic Wall: by Professor NzarubaraDocument76 pagesThoracic Wall: by Professor NzarubaraEsdras DountioNo ratings yet
- Thorax AllDocument174 pagesThorax Allravindra sharmaNo ratings yet
- Lab 2Document8 pagesLab 2Ehab AbazaNo ratings yet
- 2 DiaphragmDocument21 pages2 Diaphragmelliot kafumukacheNo ratings yet
- Pleura & LungsDocument87 pagesPleura & LungsKAYISIRE EMERYNo ratings yet
- Pectoral MusclesDocument28 pagesPectoral MusclesShivanshu BhardwajNo ratings yet
- Thoracic WallDocument100 pagesThoracic WallEman RiazNo ratings yet
- Dr. Heta Patel (PT) Assistant Professor Arip CharusatDocument25 pagesDr. Heta Patel (PT) Assistant Professor Arip CharusatfdjkvfjvNo ratings yet
- 2 Intercostal-SpaceDocument35 pages2 Intercostal-SpaceDua NjeemNo ratings yet
- Anatomy 3Document33 pagesAnatomy 3bikedet268No ratings yet
- The Axilla: Shah Hussain LECTURER (Surgical)Document81 pagesThe Axilla: Shah Hussain LECTURER (Surgical)Ibrar KhanNo ratings yet
- Anterolateral Abdominal Wall and Abdominal IncisionsDocument42 pagesAnterolateral Abdominal Wall and Abdominal IncisionsSamar AhmadNo ratings yet
- Respiratory System - AnatomyDocument28 pagesRespiratory System - AnatomyDinesh KumarNo ratings yet
- F646 CompleteSampleDocument36 pagesF646 CompleteSampleraj4523No ratings yet
- Captura de Pantalla 2023-07-20 A La(s) 14.25Document1 pageCaptura de Pantalla 2023-07-20 A La(s) 14.25Jonathan RodriguezNo ratings yet
- Class 12physics - Electric Charges and Fields - McqsDocument16 pagesClass 12physics - Electric Charges and Fields - Mcqskhushi GoyalNo ratings yet
- Product Data Sheet Powernics 9701 Black Lead Free: Berger Nippon Paint Automotive Coatings Private LimitedDocument2 pagesProduct Data Sheet Powernics 9701 Black Lead Free: Berger Nippon Paint Automotive Coatings Private LimitedSamNo ratings yet
- Aakash AIPMT 2014 Code R SolutionDocument27 pagesAakash AIPMT 2014 Code R Solutionblue_l1No ratings yet
- Strengths: Mixers - AeratorsDocument2 pagesStrengths: Mixers - AeratorsKashif MasudNo ratings yet
- Agenda: o Current Task Group Actions o Overview of API 6D 24 Edition o Future Task Group ActionsDocument29 pagesAgenda: o Current Task Group Actions o Overview of API 6D 24 Edition o Future Task Group ActionsdliyaxNo ratings yet
- Hitachi FathersdayDocument8 pagesHitachi FathersdayRiverland Welding and Tool SuppliesNo ratings yet
- DMT 231 Analogue Electronics: Introduction To Field Effect TransistorsDocument28 pagesDMT 231 Analogue Electronics: Introduction To Field Effect TransistorsAmriNo ratings yet
- BUT000 Business Partner: Topic / Contains..Document6 pagesBUT000 Business Partner: Topic / Contains..Rahul MalhotraNo ratings yet
- EN40: Dynamics and Vibrations: Solutions To Differential Equations of Motion For Vibrating SystemsDocument8 pagesEN40: Dynamics and Vibrations: Solutions To Differential Equations of Motion For Vibrating SystemsDennis KorirNo ratings yet
- CLASS - IX Mathematics (Co-Ordinate Geometry) : Material Downloaded From - 1 / 7Document7 pagesCLASS - IX Mathematics (Co-Ordinate Geometry) : Material Downloaded From - 1 / 7Neerraj YadavNo ratings yet
- PH of Buffers Hydrolysed SaltsDocument27 pagesPH of Buffers Hydrolysed SaltsFmipa Khaeru NisaaNo ratings yet
- Reactive Power Problems and System: Submitted By:-Section: - Roll No: - SubjectDocument16 pagesReactive Power Problems and System: Submitted By:-Section: - Roll No: - SubjectShubham AgrawalNo ratings yet
- Science Comprehensive Worksheet For Midterm Class 7 Ans KeyDocument8 pagesScience Comprehensive Worksheet For Midterm Class 7 Ans KeyALI ImranNo ratings yet
- National Institute of Technology Warangal Electronics & Communication Engineering DepartmentDocument5 pagesNational Institute of Technology Warangal Electronics & Communication Engineering DepartmentNaveen ShankarNo ratings yet
- MAF101 Formula Sheet-2010TR1Document2 pagesMAF101 Formula Sheet-2010TR1Ann VuNo ratings yet
- For All Sanfoundry MCQ (1000+ MCQ) JOIN Telegram GroupDocument472 pagesFor All Sanfoundry MCQ (1000+ MCQ) JOIN Telegram GroupRitesh DeshmukhNo ratings yet
- RPT ManualDocument20 pagesRPT Manualamele25No ratings yet
- A Mathematician's Apology - MediumDocument5 pagesA Mathematician's Apology - MediumPramav100% (1)
- Manage Tablespaces in A Container Database (CDB) and Pluggable Database (PDB)Document3 pagesManage Tablespaces in A Container Database (CDB) and Pluggable Database (PDB)Ahmed NagyNo ratings yet
- Eigenvalues and Eigenvectors TutorialDocument11 pagesEigenvalues and Eigenvectors TutorialMebeek DagnewNo ratings yet
- Natural Convection Heat Transfer Enhancement in New Designs of Plate-Fin Based Heat Sinks-with-cover-page-V2Document23 pagesNatural Convection Heat Transfer Enhancement in New Designs of Plate-Fin Based Heat Sinks-with-cover-page-V2ACOPIO GUAMALNo ratings yet
- Lab Report Marking Rubrics Phy645Document3 pagesLab Report Marking Rubrics Phy645Ridhwan RosliNo ratings yet
- Mechanical Datasheet - Wellhead Compressor Package Rev BDocument12 pagesMechanical Datasheet - Wellhead Compressor Package Rev BRokan Pipeline100% (1)
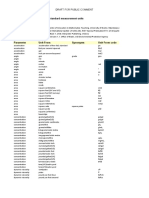
- Multipliers Used To Convert To Standard Measurement Units ReferencesDocument18 pagesMultipliers Used To Convert To Standard Measurement Units Referencesira huttNo ratings yet
- SIMATIC S7 Graph For S7-300 400 - Getting StartedDocument24 pagesSIMATIC S7 Graph For S7-300 400 - Getting StartedErica BeasleyNo ratings yet
- Eng (A724 A728 Upgrade)Document10 pagesEng (A724 A728 Upgrade)Nelson AltuveNo ratings yet
- Nano Atomic Bit ProcessingDocument296 pagesNano Atomic Bit ProcessingtrineshNo ratings yet
- Ece F314 - 2022Document3 pagesEce F314 - 2022ARCHISHA SINGHNo ratings yet