
Cirugi A Espan Ola: Scoring Systems of Severity in Patients With Multiple Trauma
Cirugi A Espan Ola: Scoring Systems of Severity in Patients With Multiple Trauma
You might also like
- 07 Aromatherapy Questionnaire PDFDocument1 page07 Aromatherapy Questionnaire PDFAgnesNo ratings yet
- Sample Haad QuestionDocument20 pagesSample Haad QuestionBobet Reña100% (3)
- Medical Mimics 2016Document24 pagesMedical Mimics 2016Susan Redmond-VaughtNo ratings yet
- Measuring Injury Severity: A Brief IntroductionDocument38 pagesMeasuring Injury Severity: A Brief IntroductionJerome LagahanNo ratings yet
- Trauma Scoring Systems: ReviewDocument4 pagesTrauma Scoring Systems: ReviewguillosarahNo ratings yet
- Performance Evaluation and Validation of The Animal TraumaDocument18 pagesPerformance Evaluation and Validation of The Animal TraumaPedro HenriqueNo ratings yet
- RTS 2011Document8 pagesRTS 2011Puspa AmandatyNo ratings yet
- Injury Severity ScoresDocument32 pagesInjury Severity ScoresscribdnillyNo ratings yet
- Trauma Geriatrico EstudioDocument6 pagesTrauma Geriatrico Estudioliz escalanteNo ratings yet
- ICMLWSDocument10 pagesICMLWSAhmed AlaaNo ratings yet
- Trauma Report 2022 WEB-2Document32 pagesTrauma Report 2022 WEB-2Jeff ONo ratings yet
- JudulDocument3 pagesJudulCacaNo ratings yet
- Trauma Mechanism Predicts The Frequency and The Severity of Injuries in Blunt Trauma PatientsDocument8 pagesTrauma Mechanism Predicts The Frequency and The Severity of Injuries in Blunt Trauma PatientsKaren CastroNo ratings yet
- Iss Rts IndoDocument6 pagesIss Rts IndoPingkanNo ratings yet
- ATLS-9e Trauma Scores PDFDocument3 pagesATLS-9e Trauma Scores PDFWaeel HamoudaNo ratings yet
- 01ta0000058130304905d 230213 040555Document10 pages01ta0000058130304905d 230213 040555nadia87nobreNo ratings yet
- WTA 2019 - Evaluation and Management of Abdominal Gunshot WoundsDocument8 pagesWTA 2019 - Evaluation and Management of Abdominal Gunshot WoundsKevin QuinterosNo ratings yet
- Trauma Scoring Systems ExplainedDocument12 pagesTrauma Scoring Systems ExplainedputugunaNo ratings yet
- Academia and Clinic: Assessing The Value of Risk Predictions by Using Risk Stratification TablesDocument11 pagesAcademia and Clinic: Assessing The Value of Risk Predictions by Using Risk Stratification Tablesbrian.p.lucasNo ratings yet
- Analisis Jurnal Pico Siti Rahma Savira AzzuhraDocument4 pagesAnalisis Jurnal Pico Siti Rahma Savira AzzuhraJoyi Park00No ratings yet
- Injury: Roman Maduz, Patrick Kugelmeier, Severin Meili, Robert Döring, Christoph Meier, Peter WahlDocument5 pagesInjury: Roman Maduz, Patrick Kugelmeier, Severin Meili, Robert Döring, Christoph Meier, Peter Wahlcirugia general Hospital San RafaelNo ratings yet
- Jurnal EbnDocument9 pagesJurnal EbnCacaNo ratings yet
- J Injury 2017 02 015Document5 pagesJ Injury 2017 02 015Ricky Rusydi SatriawanNo ratings yet
- Emerg 4 088 (9497)Document4 pagesEmerg 4 088 (9497)Taufik EffendyNo ratings yet
- Punto de Corte RR ORDocument7 pagesPunto de Corte RR ORGregorio Ramos OrtegaNo ratings yet
- Classification Multiple InjuriesDocument2 pagesClassification Multiple InjuriesElmer NarvaezNo ratings yet
- Is The New Injury Severity Score (NISS) ADocument7 pagesIs The New Injury Severity Score (NISS) ASamNo ratings yet
- Halkiadakis - A Prospective Assessment of Resilience in Trauma Patients Using The Connor-Davidson Resilience ScaleDocument6 pagesHalkiadakis - A Prospective Assessment of Resilience in Trauma Patients Using The Connor-Davidson Resilience ScaleBrittany Caroline BlackNo ratings yet
- Classification of Trauma in Children - UpToDateDocument15 pagesClassification of Trauma in Children - UpToDateLeonardo Tavares de OliveiraNo ratings yet
- Journal of Pediatric SurgeryDocument4 pagesJournal of Pediatric SurgeryRadityo Budi LeksonoNo ratings yet
- Bjs 11306Document11 pagesBjs 11306Carlos Perez RiveraNo ratings yet
- STROBE-checklist-v4-cohort-polytrauma in Pediatric Patients-1-1Document7 pagesSTROBE-checklist-v4-cohort-polytrauma in Pediatric Patients-1-1Ramona ManolitaNo ratings yet
- Propensity ScoreDocument33 pagesPropensity Scoredjsavi69100% (1)
- Review Jurnal Kelompok 1Document12 pagesReview Jurnal Kelompok 1Satria Yosi HernawanNo ratings yet
- Perioperative Risk Stratification and ModificationDocument23 pagesPerioperative Risk Stratification and ModificationDianita P Ñáñez VaronaNo ratings yet
- Journal of Statistical Software: Diagtest3Grp: An R Package For Analyzing Diagnostic Tests With Three Ordinal GroupsDocument24 pagesJournal of Statistical Software: Diagtest3Grp: An R Package For Analyzing Diagnostic Tests With Three Ordinal GroupsKhanh Ha NguyenNo ratings yet
- Acute Medicine Surgery - 2019 - Shibahashi - Can The Shock Index Be A Reliable Predictor of Early Mortality After TraumaDocument7 pagesAcute Medicine Surgery - 2019 - Shibahashi - Can The Shock Index Be A Reliable Predictor of Early Mortality After TraumaFidencio ParraNo ratings yet
- Prognostic Models in Severe Traumatic Brain Injury: A Systematic Review and Meta-AnalysisDocument16 pagesPrognostic Models in Severe Traumatic Brain Injury: A Systematic Review and Meta-AnalysisCaroline FelicianoNo ratings yet
- Classification of Trauma in ChildrenDocument9 pagesClassification of Trauma in ChildrenRita ValenteNo ratings yet
- Imaging Chronic Traumatic Brain Injury As A Risk Factor For Neurodegeneration Alzheimers DementiaDocument8 pagesImaging Chronic Traumatic Brain Injury As A Risk Factor For Neurodegeneration Alzheimers Dementiaapi-308065432No ratings yet
- S StreamDocument5 pagesS Streamad_c18No ratings yet
- Metabric Dataset Surv Analysis Gradient BoostingDocument9 pagesMetabric Dataset Surv Analysis Gradient BoostingKeren Evangeline. INo ratings yet
- Prevalence of Post Stroke Depression in Ambulatory PatientsDocument7 pagesPrevalence of Post Stroke Depression in Ambulatory PatientsSitti Rosdiana YahyaNo ratings yet
- Trauma Score ExerciseDocument6 pagesTrauma Score ExercisebobbyNo ratings yet
- Assessing The Performance of PredictionDocument11 pagesAssessing The Performance of Predictionmamanpanti00No ratings yet
- Dyac 131Document10 pagesDyac 131kkgy24tdnzNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- Healthcare 10 01438 v3Document14 pagesHealthcare 10 01438 v3Zeera MohamadNo ratings yet
- Epidemiology of Sports InjuriesDocument12 pagesEpidemiology of Sports InjuriesSurgicalgownNo ratings yet
- Trauma Scores: A Review of The Literature: ArticleDocument8 pagesTrauma Scores: A Review of The Literature: ArticleXenia PopovNo ratings yet
- The New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionDocument9 pagesThe New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionاوكتافياNo ratings yet
- The New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionDocument9 pagesThe New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionstellaNo ratings yet
- Coley 2019Document8 pagesColey 2019KaniNo ratings yet
- The GMS Hypospadias Score: Assessment of Inter-Observer Reliability and Correlation With Post - Operative ComplicationsDocument6 pagesThe GMS Hypospadias Score: Assessment of Inter-Observer Reliability and Correlation With Post - Operative ComplicationsbenimhepfiNo ratings yet
- A Comparison of The Revised Delirium Rating ScaleDocument8 pagesA Comparison of The Revised Delirium Rating ScaleMaharRkpNo ratings yet
- Cervical Spine Collar Clearance in The Obtunded Adult Blunt Trauma Patient A Systematic Review and Practice Management Guideline From The EasternDocument10 pagesCervical Spine Collar Clearance in The Obtunded Adult Blunt Trauma Patient A Systematic Review and Practice Management Guideline From The EasternMadalina TalpauNo ratings yet
- Buegeria 06 ValidationDocument28 pagesBuegeria 06 ValidationAmine BouhadiNo ratings yet
- Developing Well-Calibrated Illness Severity Scores For Decision Support in The Critically Ill - Nature-2019Document8 pagesDeveloping Well-Calibrated Illness Severity Scores For Decision Support in The Critically Ill - Nature-2019AbhishekNo ratings yet
- Periop Risk ScoringDocument7 pagesPeriop Risk ScoringMabelis EstherNo ratings yet
- Degree of Injury On Visum Et Repertum: Upine PublishersDocument2 pagesDegree of Injury On Visum Et Repertum: Upine Publishersyunita sariNo ratings yet
- Consistency of Ao Fracture Classification For The Distal RadiusDocument6 pagesConsistency of Ao Fracture Classification For The Distal RadiusNatalie AlvaradoNo ratings yet
- Zoltie N, Et Al., 1993Document4 pagesZoltie N, Et Al., 1993Hendry SusantoNo ratings yet
- Biostatistics Explored Through R Software: An OverviewFrom EverandBiostatistics Explored Through R Software: An OverviewRating: 3.5 out of 5 stars3.5/5 (2)
- Anaphylaxis Assessment and Referral After Emergency Treatment PDF 35109510368965Document15 pagesAnaphylaxis Assessment and Referral After Emergency Treatment PDF 35109510368965Rasangi Sumudu Clare SuraweeraNo ratings yet
- Acute Upper Gastrointestinal Bleeding in Over 16s Management PDF 35109565796293Document13 pagesAcute Upper Gastrointestinal Bleeding in Over 16s Management PDF 35109565796293Rasangi Sumudu Clare SuraweeraNo ratings yet
- From Goodto OutstandingDocument4 pagesFrom Goodto OutstandingRasangi Sumudu Clare SuraweeraNo ratings yet
- Schools With Soul Case Studies and Frameworks 3Document39 pagesSchools With Soul Case Studies and Frameworks 3Rasangi Sumudu Clare SuraweeraNo ratings yet
- CCM1Document5 pagesCCM1Rasangi Sumudu Clare SuraweeraNo ratings yet
- Ccr16 BookDocument228 pagesCcr16 BookRasangi Sumudu Clare SuraweeraNo ratings yet
- Peripheral Vasopressor Guide FinalDocument16 pagesPeripheral Vasopressor Guide FinalRasangi Sumudu Clare SuraweeraNo ratings yet
- Gastroparesis in Adults Oral Erythromycin PDF 54116458939430341Document29 pagesGastroparesis in Adults Oral Erythromycin PDF 54116458939430341Rasangi Sumudu Clare SuraweeraNo ratings yet
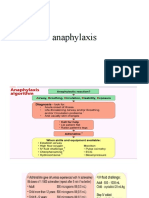
- AnaphylaxisDocument13 pagesAnaphylaxisRasangi Sumudu Clare SuraweeraNo ratings yet
- Colon CancerDocument2 pagesColon CancersweetyjonasNo ratings yet
- Antigen-Specific Immunomodulatory Effects of Transfer FactorDocument4 pagesAntigen-Specific Immunomodulatory Effects of Transfer FactorErikaAdamNo ratings yet
- Changing Paradigms Optometric Vision Therapy Is Neuro-ScienceDocument4 pagesChanging Paradigms Optometric Vision Therapy Is Neuro-SciencePierre A. RodulfoNo ratings yet
- Transport in Humans Powerpoint SlidesDocument55 pagesTransport in Humans Powerpoint SlidesTay Kai xin (Ahs)100% (1)
- A Screening Instrument For Autism Months of Age: A Follow-Up StudyDocument9 pagesA Screening Instrument For Autism Months of Age: A Follow-Up StudyJose Alonso Aguilar ValeraNo ratings yet
- Plastic Surgery Logbook Batch A - EditedDocument11 pagesPlastic Surgery Logbook Batch A - EditedRidham RanaNo ratings yet
- Pulmonary HypertensionDocument1 pagePulmonary HypertensionSa KhunNo ratings yet
- Suicide Risk Assessment Form: (Adapted From Becks Suicidal Intent Scale)Document2 pagesSuicide Risk Assessment Form: (Adapted From Becks Suicidal Intent Scale)nora_annisaNo ratings yet
- Acetaminophen Toxicity: Michira I Getange Umb/15-A/054Document31 pagesAcetaminophen Toxicity: Michira I Getange Umb/15-A/054Ahmed Ben BellaNo ratings yet
- Toshiba Xario 200 ManualDocument12 pagesToshiba Xario 200 ManualWaleed AlDhaifiNo ratings yet
- ACute Pylonephris Case PresentationDocument6 pagesACute Pylonephris Case PresentationbantilanNo ratings yet
- Braden ScaleDocument2 pagesBraden ScaleFrancis Alfred Escaran100% (1)
- ZDocument5 pagesZBiljana Custovic RadicicNo ratings yet
- 5 Different Types of PathogenDocument2 pages5 Different Types of PathogenAnonymous MvlFkyPP0% (1)
- 06 - Ambulatory Care PDFDocument50 pages06 - Ambulatory Care PDFandirio7486No ratings yet
- Yoga Meditation Class Reservation Healthy Lifestyle Instagram StoryDocument16 pagesYoga Meditation Class Reservation Healthy Lifestyle Instagram StoryRanjell Allain Bayona TorresNo ratings yet
- Acid Base BalanceDocument13 pagesAcid Base BalanceRashed ShatnawiNo ratings yet
- Prevention of Clinical Course and Complications of LymphedemaDocument3 pagesPrevention of Clinical Course and Complications of LymphedemaCentral Asian StudiesNo ratings yet
- Patent Ductus ArteriosusDocument31 pagesPatent Ductus ArteriosussuderiNo ratings yet
- Drug Abuse and Its Prevention PowerpointDocument15 pagesDrug Abuse and Its Prevention PowerpointChrizel NiloNo ratings yet
- Consequences of Overweight and ObesityDocument2 pagesConsequences of Overweight and Obesitykezia lohoNo ratings yet
- Level of PreventionDocument39 pagesLevel of PreventionMoiz Ahmed BhattiNo ratings yet
- Active Assisted and Passive Movement in TreatmentDocument4 pagesActive Assisted and Passive Movement in TreatmentshravaniNo ratings yet
- Flowing of Blood in HeartDocument5 pagesFlowing of Blood in HeartAkshay BahetyNo ratings yet
- Medina Et Al-2005-EpilepsiaDocument8 pagesMedina Et Al-2005-EpilepsiaGriselNo ratings yet
- Read More About MBT Sepsityper IVD Workflow 1682516329Document8 pagesRead More About MBT Sepsityper IVD Workflow 1682516329Jose ZelayaNo ratings yet
- Diabetes Algorithm Executive SummaryDocument30 pagesDiabetes Algorithm Executive SummaryLuis Alberto Alvarez AnkassNo ratings yet































































































Download as pdf or txt
You might also like
- 07 Aromatherapy Questionnaire PDFDocument1 page07 Aromatherapy Questionnaire PDFAgnesNo ratings yet
- Sample Haad QuestionDocument20 pagesSample Haad QuestionBobet Reña100% (3)
- Medical Mimics 2016Document24 pagesMedical Mimics 2016Susan Redmond-VaughtNo ratings yet
- Measuring Injury Severity: A Brief IntroductionDocument38 pagesMeasuring Injury Severity: A Brief IntroductionJerome LagahanNo ratings yet
- Trauma Scoring Systems: ReviewDocument4 pagesTrauma Scoring Systems: ReviewguillosarahNo ratings yet
- Performance Evaluation and Validation of The Animal TraumaDocument18 pagesPerformance Evaluation and Validation of The Animal TraumaPedro HenriqueNo ratings yet
- RTS 2011Document8 pagesRTS 2011Puspa AmandatyNo ratings yet
- Injury Severity ScoresDocument32 pagesInjury Severity ScoresscribdnillyNo ratings yet
- Trauma Geriatrico EstudioDocument6 pagesTrauma Geriatrico Estudioliz escalanteNo ratings yet
- ICMLWSDocument10 pagesICMLWSAhmed AlaaNo ratings yet
- Trauma Report 2022 WEB-2Document32 pagesTrauma Report 2022 WEB-2Jeff ONo ratings yet
- JudulDocument3 pagesJudulCacaNo ratings yet
- Trauma Mechanism Predicts The Frequency and The Severity of Injuries in Blunt Trauma PatientsDocument8 pagesTrauma Mechanism Predicts The Frequency and The Severity of Injuries in Blunt Trauma PatientsKaren CastroNo ratings yet
- Iss Rts IndoDocument6 pagesIss Rts IndoPingkanNo ratings yet
- ATLS-9e Trauma Scores PDFDocument3 pagesATLS-9e Trauma Scores PDFWaeel HamoudaNo ratings yet
- 01ta0000058130304905d 230213 040555Document10 pages01ta0000058130304905d 230213 040555nadia87nobreNo ratings yet
- WTA 2019 - Evaluation and Management of Abdominal Gunshot WoundsDocument8 pagesWTA 2019 - Evaluation and Management of Abdominal Gunshot WoundsKevin QuinterosNo ratings yet
- Trauma Scoring Systems ExplainedDocument12 pagesTrauma Scoring Systems ExplainedputugunaNo ratings yet
- Academia and Clinic: Assessing The Value of Risk Predictions by Using Risk Stratification TablesDocument11 pagesAcademia and Clinic: Assessing The Value of Risk Predictions by Using Risk Stratification Tablesbrian.p.lucasNo ratings yet
- Analisis Jurnal Pico Siti Rahma Savira AzzuhraDocument4 pagesAnalisis Jurnal Pico Siti Rahma Savira AzzuhraJoyi Park00No ratings yet
- Injury: Roman Maduz, Patrick Kugelmeier, Severin Meili, Robert Döring, Christoph Meier, Peter WahlDocument5 pagesInjury: Roman Maduz, Patrick Kugelmeier, Severin Meili, Robert Döring, Christoph Meier, Peter Wahlcirugia general Hospital San RafaelNo ratings yet
- Jurnal EbnDocument9 pagesJurnal EbnCacaNo ratings yet
- J Injury 2017 02 015Document5 pagesJ Injury 2017 02 015Ricky Rusydi SatriawanNo ratings yet
- Emerg 4 088 (9497)Document4 pagesEmerg 4 088 (9497)Taufik EffendyNo ratings yet
- Punto de Corte RR ORDocument7 pagesPunto de Corte RR ORGregorio Ramos OrtegaNo ratings yet
- Classification Multiple InjuriesDocument2 pagesClassification Multiple InjuriesElmer NarvaezNo ratings yet
- Is The New Injury Severity Score (NISS) ADocument7 pagesIs The New Injury Severity Score (NISS) ASamNo ratings yet
- Halkiadakis - A Prospective Assessment of Resilience in Trauma Patients Using The Connor-Davidson Resilience ScaleDocument6 pagesHalkiadakis - A Prospective Assessment of Resilience in Trauma Patients Using The Connor-Davidson Resilience ScaleBrittany Caroline BlackNo ratings yet
- Classification of Trauma in Children - UpToDateDocument15 pagesClassification of Trauma in Children - UpToDateLeonardo Tavares de OliveiraNo ratings yet
- Journal of Pediatric SurgeryDocument4 pagesJournal of Pediatric SurgeryRadityo Budi LeksonoNo ratings yet
- Bjs 11306Document11 pagesBjs 11306Carlos Perez RiveraNo ratings yet
- STROBE-checklist-v4-cohort-polytrauma in Pediatric Patients-1-1Document7 pagesSTROBE-checklist-v4-cohort-polytrauma in Pediatric Patients-1-1Ramona ManolitaNo ratings yet
- Propensity ScoreDocument33 pagesPropensity Scoredjsavi69100% (1)
- Review Jurnal Kelompok 1Document12 pagesReview Jurnal Kelompok 1Satria Yosi HernawanNo ratings yet
- Perioperative Risk Stratification and ModificationDocument23 pagesPerioperative Risk Stratification and ModificationDianita P Ñáñez VaronaNo ratings yet
- Journal of Statistical Software: Diagtest3Grp: An R Package For Analyzing Diagnostic Tests With Three Ordinal GroupsDocument24 pagesJournal of Statistical Software: Diagtest3Grp: An R Package For Analyzing Diagnostic Tests With Three Ordinal GroupsKhanh Ha NguyenNo ratings yet
- Acute Medicine Surgery - 2019 - Shibahashi - Can The Shock Index Be A Reliable Predictor of Early Mortality After TraumaDocument7 pagesAcute Medicine Surgery - 2019 - Shibahashi - Can The Shock Index Be A Reliable Predictor of Early Mortality After TraumaFidencio ParraNo ratings yet
- Prognostic Models in Severe Traumatic Brain Injury: A Systematic Review and Meta-AnalysisDocument16 pagesPrognostic Models in Severe Traumatic Brain Injury: A Systematic Review and Meta-AnalysisCaroline FelicianoNo ratings yet
- Classification of Trauma in ChildrenDocument9 pagesClassification of Trauma in ChildrenRita ValenteNo ratings yet
- Imaging Chronic Traumatic Brain Injury As A Risk Factor For Neurodegeneration Alzheimers DementiaDocument8 pagesImaging Chronic Traumatic Brain Injury As A Risk Factor For Neurodegeneration Alzheimers Dementiaapi-308065432No ratings yet
- S StreamDocument5 pagesS Streamad_c18No ratings yet
- Metabric Dataset Surv Analysis Gradient BoostingDocument9 pagesMetabric Dataset Surv Analysis Gradient BoostingKeren Evangeline. INo ratings yet
- Prevalence of Post Stroke Depression in Ambulatory PatientsDocument7 pagesPrevalence of Post Stroke Depression in Ambulatory PatientsSitti Rosdiana YahyaNo ratings yet
- Trauma Score ExerciseDocument6 pagesTrauma Score ExercisebobbyNo ratings yet
- Assessing The Performance of PredictionDocument11 pagesAssessing The Performance of Predictionmamanpanti00No ratings yet
- Dyac 131Document10 pagesDyac 131kkgy24tdnzNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- Healthcare 10 01438 v3Document14 pagesHealthcare 10 01438 v3Zeera MohamadNo ratings yet
- Epidemiology of Sports InjuriesDocument12 pagesEpidemiology of Sports InjuriesSurgicalgownNo ratings yet
- Trauma Scores: A Review of The Literature: ArticleDocument8 pagesTrauma Scores: A Review of The Literature: ArticleXenia PopovNo ratings yet
- The New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionDocument9 pagesThe New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionاوكتافياNo ratings yet
- The New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionDocument9 pagesThe New Trauma Score (NTS) : A Modification of The Revised Trauma Score For Better Trauma Mortality PredictionstellaNo ratings yet
- Coley 2019Document8 pagesColey 2019KaniNo ratings yet
- The GMS Hypospadias Score: Assessment of Inter-Observer Reliability and Correlation With Post - Operative ComplicationsDocument6 pagesThe GMS Hypospadias Score: Assessment of Inter-Observer Reliability and Correlation With Post - Operative ComplicationsbenimhepfiNo ratings yet
- A Comparison of The Revised Delirium Rating ScaleDocument8 pagesA Comparison of The Revised Delirium Rating ScaleMaharRkpNo ratings yet
- Cervical Spine Collar Clearance in The Obtunded Adult Blunt Trauma Patient A Systematic Review and Practice Management Guideline From The EasternDocument10 pagesCervical Spine Collar Clearance in The Obtunded Adult Blunt Trauma Patient A Systematic Review and Practice Management Guideline From The EasternMadalina TalpauNo ratings yet
- Buegeria 06 ValidationDocument28 pagesBuegeria 06 ValidationAmine BouhadiNo ratings yet
- Developing Well-Calibrated Illness Severity Scores For Decision Support in The Critically Ill - Nature-2019Document8 pagesDeveloping Well-Calibrated Illness Severity Scores For Decision Support in The Critically Ill - Nature-2019AbhishekNo ratings yet
- Periop Risk ScoringDocument7 pagesPeriop Risk ScoringMabelis EstherNo ratings yet
- Degree of Injury On Visum Et Repertum: Upine PublishersDocument2 pagesDegree of Injury On Visum Et Repertum: Upine Publishersyunita sariNo ratings yet
- Consistency of Ao Fracture Classification For The Distal RadiusDocument6 pagesConsistency of Ao Fracture Classification For The Distal RadiusNatalie AlvaradoNo ratings yet
- Zoltie N, Et Al., 1993Document4 pagesZoltie N, Et Al., 1993Hendry SusantoNo ratings yet
- Biostatistics Explored Through R Software: An OverviewFrom EverandBiostatistics Explored Through R Software: An OverviewRating: 3.5 out of 5 stars3.5/5 (2)
- Anaphylaxis Assessment and Referral After Emergency Treatment PDF 35109510368965Document15 pagesAnaphylaxis Assessment and Referral After Emergency Treatment PDF 35109510368965Rasangi Sumudu Clare SuraweeraNo ratings yet
- Acute Upper Gastrointestinal Bleeding in Over 16s Management PDF 35109565796293Document13 pagesAcute Upper Gastrointestinal Bleeding in Over 16s Management PDF 35109565796293Rasangi Sumudu Clare SuraweeraNo ratings yet
- From Goodto OutstandingDocument4 pagesFrom Goodto OutstandingRasangi Sumudu Clare SuraweeraNo ratings yet
- Schools With Soul Case Studies and Frameworks 3Document39 pagesSchools With Soul Case Studies and Frameworks 3Rasangi Sumudu Clare SuraweeraNo ratings yet
- CCM1Document5 pagesCCM1Rasangi Sumudu Clare SuraweeraNo ratings yet
- Ccr16 BookDocument228 pagesCcr16 BookRasangi Sumudu Clare SuraweeraNo ratings yet
- Peripheral Vasopressor Guide FinalDocument16 pagesPeripheral Vasopressor Guide FinalRasangi Sumudu Clare SuraweeraNo ratings yet
- Gastroparesis in Adults Oral Erythromycin PDF 54116458939430341Document29 pagesGastroparesis in Adults Oral Erythromycin PDF 54116458939430341Rasangi Sumudu Clare SuraweeraNo ratings yet
- AnaphylaxisDocument13 pagesAnaphylaxisRasangi Sumudu Clare SuraweeraNo ratings yet
- Colon CancerDocument2 pagesColon CancersweetyjonasNo ratings yet
- Antigen-Specific Immunomodulatory Effects of Transfer FactorDocument4 pagesAntigen-Specific Immunomodulatory Effects of Transfer FactorErikaAdamNo ratings yet
- Changing Paradigms Optometric Vision Therapy Is Neuro-ScienceDocument4 pagesChanging Paradigms Optometric Vision Therapy Is Neuro-SciencePierre A. RodulfoNo ratings yet
- Transport in Humans Powerpoint SlidesDocument55 pagesTransport in Humans Powerpoint SlidesTay Kai xin (Ahs)100% (1)
- A Screening Instrument For Autism Months of Age: A Follow-Up StudyDocument9 pagesA Screening Instrument For Autism Months of Age: A Follow-Up StudyJose Alonso Aguilar ValeraNo ratings yet
- Plastic Surgery Logbook Batch A - EditedDocument11 pagesPlastic Surgery Logbook Batch A - EditedRidham RanaNo ratings yet
- Pulmonary HypertensionDocument1 pagePulmonary HypertensionSa KhunNo ratings yet
- Suicide Risk Assessment Form: (Adapted From Becks Suicidal Intent Scale)Document2 pagesSuicide Risk Assessment Form: (Adapted From Becks Suicidal Intent Scale)nora_annisaNo ratings yet
- Acetaminophen Toxicity: Michira I Getange Umb/15-A/054Document31 pagesAcetaminophen Toxicity: Michira I Getange Umb/15-A/054Ahmed Ben BellaNo ratings yet
- Toshiba Xario 200 ManualDocument12 pagesToshiba Xario 200 ManualWaleed AlDhaifiNo ratings yet
- ACute Pylonephris Case PresentationDocument6 pagesACute Pylonephris Case PresentationbantilanNo ratings yet
- Braden ScaleDocument2 pagesBraden ScaleFrancis Alfred Escaran100% (1)
- ZDocument5 pagesZBiljana Custovic RadicicNo ratings yet
- 5 Different Types of PathogenDocument2 pages5 Different Types of PathogenAnonymous MvlFkyPP0% (1)
- 06 - Ambulatory Care PDFDocument50 pages06 - Ambulatory Care PDFandirio7486No ratings yet
- Yoga Meditation Class Reservation Healthy Lifestyle Instagram StoryDocument16 pagesYoga Meditation Class Reservation Healthy Lifestyle Instagram StoryRanjell Allain Bayona TorresNo ratings yet
- Acid Base BalanceDocument13 pagesAcid Base BalanceRashed ShatnawiNo ratings yet
- Prevention of Clinical Course and Complications of LymphedemaDocument3 pagesPrevention of Clinical Course and Complications of LymphedemaCentral Asian StudiesNo ratings yet
- Patent Ductus ArteriosusDocument31 pagesPatent Ductus ArteriosussuderiNo ratings yet
- Drug Abuse and Its Prevention PowerpointDocument15 pagesDrug Abuse and Its Prevention PowerpointChrizel NiloNo ratings yet
- Consequences of Overweight and ObesityDocument2 pagesConsequences of Overweight and Obesitykezia lohoNo ratings yet
- Level of PreventionDocument39 pagesLevel of PreventionMoiz Ahmed BhattiNo ratings yet
- Active Assisted and Passive Movement in TreatmentDocument4 pagesActive Assisted and Passive Movement in TreatmentshravaniNo ratings yet
- Flowing of Blood in HeartDocument5 pagesFlowing of Blood in HeartAkshay BahetyNo ratings yet
- Medina Et Al-2005-EpilepsiaDocument8 pagesMedina Et Al-2005-EpilepsiaGriselNo ratings yet
- Read More About MBT Sepsityper IVD Workflow 1682516329Document8 pagesRead More About MBT Sepsityper IVD Workflow 1682516329Jose ZelayaNo ratings yet
- Diabetes Algorithm Executive SummaryDocument30 pagesDiabetes Algorithm Executive SummaryLuis Alberto Alvarez AnkassNo ratings yet