Download as pdf or txt
You might also like
- Nursing Laboratory and Diagnostic Tests Demystified, Second EditionFrom EverandNursing Laboratory and Diagnostic Tests Demystified, Second EditionNo ratings yet
- Case Study About HyperthyroidismDocument11 pagesCase Study About HyperthyroidismRheciel Abarquez Briones RN100% (4)
- 100 Test Aarogya 2.0:: Mrs - Gunjan MisraDocument19 pages100 Test Aarogya 2.0:: Mrs - Gunjan Misramomo misraNo ratings yet
- LabReportNew - 2023-07-29T172316.072Document6 pagesLabReportNew - 2023-07-29T172316.072Deependra YadavNo ratings yet
- MR - Abhishek PangotraDocument6 pagesMR - Abhishek PangotraAbishek Pangotra (Abi Sharma)No ratings yet
- Date 07/feb/2021 08:43AM Unit Bio Ref Interval: Laboratory Investigation ReportDocument8 pagesDate 07/feb/2021 08:43AM Unit Bio Ref Interval: Laboratory Investigation ReportRaghav SinghNo ratings yet
- K SUJATHA-Female55 Years-927Document5 pagesK SUJATHA-Female55 Years-927vijaykumarNo ratings yet
- DRRKDocument1 pageDRRKrevanth kallaNo ratings yet
- LabreportnewDocument14 pagesLabreportnewRajesh SharmaNo ratings yet
- FC1138497Document5 pagesFC1138497SK FahimNo ratings yet
- Lab ReportDocument4 pagesLab ReportanilchowdaryNo ratings yet
- ReportDocument3 pagesReportFascino WhiteNo ratings yet
- C Koro PV 384341Document4 pagesC Koro PV 384341Arnold SchwarzeneggerNo ratings yet
- PatientReport 2Document11 pagesPatientReport 2Sagarika MishraNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Document3 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 102Ramesh KumarNo ratings yet
- Department of Clinical Biochemistry: Investigation Name Result Bio. Ref. Range MethodDocument8 pagesDepartment of Clinical Biochemistry: Investigation Name Result Bio. Ref. Range MethodarupNo ratings yet
- ReportDocument7 pagesReportsri harshaNo ratings yet
- Plot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Document11 pagesPlot No.428, Phase-IV, Udyog Vihar, Gurgaon, Haryana - 122 015Pksk SkpkNo ratings yet
- LabTest 29dec2023Document15 pagesLabTest 29dec2023Ayush KumarNo ratings yet
- 1-Liver Function Test - PO4201376835-816 PDFDocument6 pages1-Liver Function Test - PO4201376835-816 PDFkhooniNo ratings yet
- Test Name Result Unit Bio Ref. Interval Method: Glucose, FastingDocument6 pagesTest Name Result Unit Bio Ref. Interval Method: Glucose, FastingDeepneel KunduNo ratings yet
- Shailendra Tamanekar 06102022 Report-1Document2 pagesShailendra Tamanekar 06102022 Report-1Shailendra TamanekarNo ratings yet
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDocument6 pagesDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodJaya LakshmiNo ratings yet
- Mr. SALIMDocument2 pagesMr. SALIMClan of comedyNo ratings yet
- Bilas, Remedios Maloloy-On 2485027317Document5 pagesBilas, Remedios Maloloy-On 2485027317mjdigitalprint18No ratings yet
- Atrnoq04nglh2b355kfl2vueDocument4 pagesAtrnoq04nglh2b355kfl2vueDev MathurNo ratings yet
- Report (5) DasuDocument1 pageReport (5) DasuDasu GundiNo ratings yet
- 100 Test Aarogya 2.0:: Mrs - Nisha KatouriaDocument18 pages100 Test Aarogya 2.0:: Mrs - Nisha KatouriaNisha KathuriaNo ratings yet
- Ajtj3770052-050224 2662Document1 pageAjtj3770052-050224 2662desilvamnimeshNo ratings yet
- Lab ReportDocument1 pageLab ReportManav MohataNo ratings yet
- Sample Type: Serum Client Address:: Obtained ValueDocument1 pageSample Type: Serum Client Address:: Obtained Valuesrini vasuNo ratings yet
- Department of Biochemistry Test Name Result Unit Bio. Ref. RangeDocument3 pagesDepartment of Biochemistry Test Name Result Unit Bio. Ref. RangeAdityaNo ratings yet
- 101 Test Aarogya 2.0:: Mrs - Phulwanti KaurDocument13 pages101 Test Aarogya 2.0:: Mrs - Phulwanti KaurNaunidh SinghNo ratings yet
- Laboratory Test Report: Male 16 YearsDocument3 pagesLaboratory Test Report: Male 16 YearsChandrika VeerareddyNo ratings yet
- Test ReportDocument2 pagesTest ReportChaudhary Ahmed IftikharNo ratings yet
- A51166900073265155 - RLS Blood & Urinal TestDocument9 pagesA51166900073265155 - RLS Blood & Urinal TestAjay Chowdary Ajay ChowdaryNo ratings yet
- Labreportnew AspxDocument2 pagesLabreportnew AspxAhana MondalNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 141Document6 pagesLaboratory Test Report: Test Name Result Biological Reference Interval Fasting Plasma Glucose: 141Ravichandran M.N.No ratings yet
- Aaop3438201-121123 2662Document1 pageAaop3438201-121123 2662fahadcaderNo ratings yet
- Patient Report Direct ViewDocument2 pagesPatient Report Direct ViewalishNo ratings yet
- Lab Report002443618Document2 pagesLab Report002443618Ed LucasNo ratings yet
- IRNDM2600110 - Report PDFDocument2 pagesIRNDM2600110 - Report PDFPhilipNo ratings yet
- Wlifr1p4cvapn5otog23kbblDocument4 pagesWlifr1p4cvapn5otog23kbblGajanan KodnikarNo ratings yet
- SR8767151Document2 pagesSR8767151imbipuldas14No ratings yet
- Report - Murli Dhar Singh (40122400045)Document8 pagesReport - Murli Dhar Singh (40122400045)amit7609singhNo ratings yet
- Department of Biochemistry Iho - Rural Camp Package Test Name Result Unit Bio. Ref. RangeDocument4 pagesDepartment of Biochemistry Iho - Rural Camp Package Test Name Result Unit Bio. Ref. Rangethakurvikrant40678No ratings yet
- UgpeDocument3 pagesUgpeOlety Subrahmanya SastryNo ratings yet
- LipidDocument1 pageLipidrajanarora72No ratings yet
- Usjl2707Document2 pagesUsjl2707Ashvik AnumakondaNo ratings yet
- IRNEF2600160Document2 pagesIRNEF2600160Gopakumar KesavakurupNo ratings yet
- Department of Biochemistry-Routine: Test Name Result Unit Bio. Ref. Range MethodDocument10 pagesDepartment of Biochemistry-Routine: Test Name Result Unit Bio. Ref. Range MethodbfdfndfNo ratings yet
- MorrrDocument4 pagesMorrrveenit2512No ratings yet
- 2021 - 07 - 24 8 - 15 PM Office LensDocument9 pages2021 - 07 - 24 8 - 15 PM Office LensY RahulNo ratings yet
- Laboratory Investigation Report::: Patient Name: Age/Sex:: Order Date Uhid: Ref. Doctor 2Document2 pagesLaboratory Investigation Report::: Patient Name: Age/Sex:: Order Date Uhid: Ref. Doctor 2tanmayNo ratings yet
- Kongamdana: Clinical BiochemistryDocument5 pagesKongamdana: Clinical BiochemistryShariqNo ratings yet
- RXUV8166Document1 pageRXUV8166nagakiran9No ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveDocument5 pagesLaboratory Test Report: Test Name Result Biological Reference Interval TSH UltrasensitiveP Nagaraju RajuNo ratings yet
- Mr. PAWAN JAINDocument1 pageMr. PAWAN JAINAshish BakliwalNo ratings yet
- FC0850661Document1 pageFC0850661SK FahimNo ratings yet
- MR - SOMASEKHAR 4401 1339028Document2 pagesMR - SOMASEKHAR 4401 1339028Sampangi Bellary SomasekharNo ratings yet
- Labreportnew - 2024-03-15T102048.645Document4 pagesLabreportnew - 2024-03-15T102048.645AnkushNo ratings yet
- Republic of The Philippines Tarlac State UniversityDocument36 pagesRepublic of The Philippines Tarlac State UniversityLeslie Rufino100% (1)
- Thyroiditis Dissertation SignedDocument29 pagesThyroiditis Dissertation SignedRogers256No ratings yet
- J Ejrad 2015 02 009Document5 pagesJ Ejrad 2015 02 009sujit naikNo ratings yet
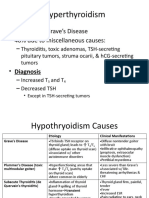
- Hyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesDocument6 pagesHyperthyroidism: - 60% Due To Grave's Disease - 40% Due To Miscellaneous CausesLeitavia D.No ratings yet
- Istar 500 Drawray Catalog PDFDocument2 pagesIstar 500 Drawray Catalog PDFCV Langgeng Jaya Bojonegoro50% (2)
- Reflexology Association of Canada - Foot Chart: Plantar ViewDocument1 pageReflexology Association of Canada - Foot Chart: Plantar ViewprabhaNo ratings yet
- KHURAISADocument6 pagesKHURAISASAINI JONINo ratings yet
- Lecture 2 - Pituitary Hormones and Their Control by The HypothalamusDocument39 pagesLecture 2 - Pituitary Hormones and Their Control by The HypothalamusHomeground entertainmentNo ratings yet
- Name Test Asked Amh, T3-T4-Tsh:: Sample Collected At: Ref. By: DR S KumarDocument2 pagesName Test Asked Amh, T3-T4-Tsh:: Sample Collected At: Ref. By: DR S KumarPraful SahooNo ratings yet
- Endocrine System - QuizizzDocument8 pagesEndocrine System - QuizizzushduNo ratings yet
- CC2 Lab 13Document10 pagesCC2 Lab 13Junea SeeNo ratings yet
- Dpa Cross Sectional Study On The Prevalence of Thyroid Disorders in The Urban Community of DelhiDocument54 pagesDpa Cross Sectional Study On The Prevalence of Thyroid Disorders in The Urban Community of DelhiGurmeet SinghNo ratings yet
- 2022 ATA Abstracts Submission Guide FinalDocument17 pages2022 ATA Abstracts Submission Guide FinalMiNo ratings yet
- Thyroid Function Test (TFT)Document16 pagesThyroid Function Test (TFT)PAPUN KUMAR ROUTNo ratings yet
- DIPRINTDocument1 pageDIPRINTAnonymous wRiKUO07DHNo ratings yet
- ReportDocument1 pageReportRanjan Mano100% (1)
- Askari Lab, Gojra RD.: Reference BillDocument1 pageAskari Lab, Gojra RD.: Reference Billmeer haadiNo ratings yet
- Durg SytudDocument5 pagesDurg SytudRocco WalksNo ratings yet
- Anatomy and Physiology of Adrenal GlandsDocument4 pagesAnatomy and Physiology of Adrenal Glandsxxxcamzxxx100% (3)
- 2.pituitary AdenomaDocument2 pages2.pituitary Adenoma張宏軒No ratings yet
- Endocrine-System-Lesson-Plan Final Na FinalDocument11 pagesEndocrine-System-Lesson-Plan Final Na FinalRaymond Joseph Bersamin100% (3)
- Thyroid GlandDocument59 pagesThyroid Glandbessan alfqeatNo ratings yet
- AIA Test Menu - Catalogue - CDocument2 pagesAIA Test Menu - Catalogue - CÂn Đình0% (1)
- "Oral Questions in Clinical Surgery" Case 1. LipomaDocument19 pages"Oral Questions in Clinical Surgery" Case 1. LipomaSherif Magdi100% (3)
- Referat 6. Daftar Pustaka HipertiroidDocument2 pagesReferat 6. Daftar Pustaka HipertiroidSigit Dwi RahardjoNo ratings yet
- Secretion of Small IntestineDocument18 pagesSecretion of Small IntestineMaliha MumtazNo ratings yet
- Digestive and Endocrine System: 5141 CN 111 - Anatomy and PhysiologyDocument4 pagesDigestive and Endocrine System: 5141 CN 111 - Anatomy and PhysiologyAlthea Joyce OngNo ratings yet
- HYPERTHYROIDISMDocument40 pagesHYPERTHYROIDISMEmmanuelNo ratings yet
- Evaluation of Some Thyriod Hormones in Diabetics Attending Abia State University Teaching HospitalDocument7 pagesEvaluation of Some Thyriod Hormones in Diabetics Attending Abia State University Teaching HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet