Download as pdf or txt
You might also like
- Star Wars Republic Holonet NewsDocument13 pagesStar Wars Republic Holonet NewsJessie Abraham LaidlawNo ratings yet
- Smoke Extraction System Sample CalculationDocument5 pagesSmoke Extraction System Sample Calculationsmcsaminda100% (3)
- Arthroscopic Irrigation and Debridement Is Associated With Favourable Short-Term Outcomes vs. Open Management - An ACS-NSQIP Database AnalysisDocument7 pagesArthroscopic Irrigation and Debridement Is Associated With Favourable Short-Term Outcomes vs. Open Management - An ACS-NSQIP Database AnalysisLaura AreizaNo ratings yet
- 10 36516-Jocass 1276127-3055931Document5 pages10 36516-Jocass 1276127-3055931yyyyx842No ratings yet
- Nej M Abbotts TentDocument11 pagesNej M Abbotts TentWKYC.comNo ratings yet
- Prior Knee ArthrosDocument5 pagesPrior Knee ArthrosMaría Fernanda LópezNo ratings yet
- Foot & Ankle International: Minimal Incision Surgery For Tibiotalocalcaneal ArthrodesisDocument14 pagesFoot & Ankle International: Minimal Incision Surgery For Tibiotalocalcaneal Arthrodesisapi-241264935No ratings yet
- The Journal of Foot & Ankle SurgeryDocument5 pagesThe Journal of Foot & Ankle SurgeryGilbert Tormis DaguploNo ratings yet
- Patho BCISDocument8 pagesPatho BCISthanawatsimaNo ratings yet
- The Journal of Arthroplasty: Aaron J. Casp, MD, James A. Browne, MD, Nicole E. Durig, MD, MS, Brian C. Werner, MDDocument4 pagesThe Journal of Arthroplasty: Aaron J. Casp, MD, James A. Browne, MD, Nicole E. Durig, MD, MS, Brian C. Werner, MDLussy Tri OctavianiNo ratings yet
- Relación Flujo y Fractura ClinicaDocument5 pagesRelación Flujo y Fractura ClinicaPedro TorresNo ratings yet
- Cardio VacDocument6 pagesCardio VacstarzecNo ratings yet
- Lberaçao Capsular Posteror CrurgcaDocument7 pagesLberaçao Capsular Posteror CrurgcaEduardo FilhoNo ratings yet
- 2023 Article 35384Document9 pages2023 Article 35384RoqueAlvaradoNo ratings yet
- The Timing of Corticosteroid Injections After Arthroscopic Shoulder ProceduresDocument7 pagesThe Timing of Corticosteroid Injections After Arthroscopic Shoulder Proceduresjo chenNo ratings yet
- Zalavras 2009Document6 pagesZalavras 2009Mohamed GoudaNo ratings yet
- BasilDocument10 pagesBasilDavid FlynnNo ratings yet
- Siman2017 ORTOPEDIADocument6 pagesSiman2017 ORTOPEDIAOrto MespNo ratings yet
- Clinical Outcomes in Patients With Scaphoid Non UnDocument5 pagesClinical Outcomes in Patients With Scaphoid Non UndominguezdoradopatriciaNo ratings yet
- 1 s2.0 S0022480422008150 MainDocument11 pages1 s2.0 S0022480422008150 MainYodi SoebadiNo ratings yet
- Venous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesDocument13 pagesVenous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesSebastiano Della CasaNo ratings yet
- Vascular Injury With FXDocument4 pagesVascular Injury With FXDoctor's BettaNo ratings yet
- Higher - C=4 - n=15 - J Clin Med - Osteoarthritis Progression after ACL Reconstruction Was Significantly Higher Than That of the Healthy Contralateral Knees- Long-Term Follow Up Study of Mean 16.4 YearsDocument8 pagesHigher - C=4 - n=15 - J Clin Med - Osteoarthritis Progression after ACL Reconstruction Was Significantly Higher Than That of the Healthy Contralateral Knees- Long-Term Follow Up Study of Mean 16.4 YearsrandocalNo ratings yet
- Atm 08 23 1626Document12 pagesAtm 08 23 1626Susana MalleaNo ratings yet
- Intracranial Haemorrhage (ICH) Occurs in About 5% of Patients With IEDocument5 pagesIntracranial Haemorrhage (ICH) Occurs in About 5% of Patients With IETnf-alpha DelusionNo ratings yet
- 53 - Changes in Arthroscopic Findings in The Anterior Cruciate Ligament Deficient Knee Prior To Reconstructive SurgeryDocument3 pages53 - Changes in Arthroscopic Findings in The Anterior Cruciate Ligament Deficient Knee Prior To Reconstructive SurgeryrandocalNo ratings yet
- Alar Hay em 2018Document5 pagesAlar Hay em 2018Amelia Kristin SimanjuntakNo ratings yet
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Document6 pagesSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaNo ratings yet
- Boissonneault2019 PDFDocument17 pagesBoissonneault2019 PDFBangkit PrimayudhaNo ratings yet
- EstudosDocument8 pagesEstudosPaulo ManoelNo ratings yet
- WRR 12418Document7 pagesWRR 12418nindaNo ratings yet
- Fate of The ACL-Injured Patient - A Prospective Study (Daniel Et Al1993)Document13 pagesFate of The ACL-Injured Patient - A Prospective Study (Daniel Et Al1993)nsboyadzhievNo ratings yet
- JCM 11 06915Document9 pagesJCM 11 06915CLINIC SURGERY 17THNo ratings yet
- Mcrae 2015Document8 pagesMcrae 2015Ananth BalakrishnanNo ratings yet
- Asensio, JA, (2020) - Tratamiento Quirúrgico de Las Lesiones de La Arteria Braquial y Predictores de Resultado.Document12 pagesAsensio, JA, (2020) - Tratamiento Quirúrgico de Las Lesiones de La Arteria Braquial y Predictores de Resultado.Edgar Geovanny Cardenas FigueroaNo ratings yet
- Dco 5 PDFDocument10 pagesDco 5 PDFGauda GranthanaNo ratings yet
- Arthroplasty As Primary Treatment For Distal Humeral Fractures Produces Reliable Results With Regards To Revisions and Adverse Events A Registry-Based Study2019Document7 pagesArthroplasty As Primary Treatment For Distal Humeral Fractures Produces Reliable Results With Regards To Revisions and Adverse Events A Registry-Based Study2019camilaNo ratings yet
- Our Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteDocument11 pagesOur Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteAthenaeum Scientific PublishersNo ratings yet
- Ekim, H. y Tuncer, M. (2009) - Manejo de Lesiones Traumáticas de La Arteria Braquial Informe de 49 PacientesDocument5 pagesEkim, H. y Tuncer, M. (2009) - Manejo de Lesiones Traumáticas de La Arteria Braquial Informe de 49 PacientesEdgar Geovanny Cardenas FigueroaNo ratings yet
- 08 Subasi NecmiogluDocument7 pages08 Subasi Necmiogludoos1No ratings yet
- The Chertsey Classification of Tibial Plateau FracDocument2 pagesThe Chertsey Classification of Tibial Plateau FracWahyuu N PutraNo ratings yet
- Length of Stay Total Knee ArthroplastyDocument9 pagesLength of Stay Total Knee ArthroplastyRista MarginaNo ratings yet
- Pelvic BinderDocument9 pagesPelvic BinderrizcoolNo ratings yet
- J Jacc 2012 10 036Document6 pagesJ Jacc 2012 10 036Ertan ALNo ratings yet
- Triple Arthrodesis in Rheumatoid ArthritisDocument5 pagesTriple Arthrodesis in Rheumatoid ArthritisZahrotul Fitria SuryawanNo ratings yet
- Septic Ligament: ArthroscopicDocument7 pagesSeptic Ligament: ArthroscopicleonardocahyoNo ratings yet
- Biomedicines 11 00979Document10 pagesBiomedicines 11 00979akinaNo ratings yet
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocument8 pagesMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersNo ratings yet
- Precontoured Locking CompressiDocument8 pagesPrecontoured Locking CompressiPrincess BabyNo ratings yet
- Onwudike 2020Document10 pagesOnwudike 2020Han's OfficialNo ratings yet
- 1494-Article Text-5451-1-10-20240329Document12 pages1494-Article Text-5451-1-10-20240329Indra SanjayaNo ratings yet
- Upper Extremity Venous Thromboembolism Following ODocument7 pagesUpper Extremity Venous Thromboembolism Following ODeborah SalinasNo ratings yet
- A-Line Complication PDFDocument8 pagesA-Line Complication PDFaeagesNo ratings yet
- 2004 Espectro Clínico Del Síndrome Compartimental Agudo Del Muslo y Su Relación Con Las Lesiones AsociadasDocument7 pages2004 Espectro Clínico Del Síndrome Compartimental Agudo Del Muslo y Su Relación Con Las Lesiones AsociadasDeybid CaihuaraNo ratings yet
- Clavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseDocument6 pagesClavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseAngel IschiaNo ratings yet
- Acute Compartment Syndrome of The Lower Leg: Retrospective Study On Prevalence, Technique, and Outcome of FasciotomiesDocument5 pagesAcute Compartment Syndrome of The Lower Leg: Retrospective Study On Prevalence, Technique, and Outcome of FasciotomiesTHE.GUNNERSNo ratings yet
- Khairy 2017Document7 pagesKhairy 2017Beby Dwi Lestari BajryNo ratings yet
- Clinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyDocument7 pagesClinical Presentation, Management, and Prognosis of Pseudogout in Joint Arthroplasty: A Retrospective Cohort StudyPutri Aswariyah RamliNo ratings yet
- Case Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesDocument10 pagesCase Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesdorfynatorNo ratings yet
- Epididymo-Orchitis in Spinal Cord Injury Patients On Cic: A Case SeriesDocument3 pagesEpididymo-Orchitis in Spinal Cord Injury Patients On Cic: A Case SeriesIJAR JOURNALNo ratings yet
- Readmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsDocument9 pagesReadmission and Other Adverse Events After Transsphenoidal Surgery: Prevalence, Timing, and Predictive FactorsbobNo ratings yet
- Unicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsFrom EverandUnicompartmental Knee Arthroplasty: Indications, Surgical Techniques and ComplicationsTad L. GerlingerNo ratings yet
- Creativity in Engineering Design ProcessDocument12 pagesCreativity in Engineering Design ProcessNurhuda HayatiNo ratings yet
- Autonomous Ships ChallengesDocument5 pagesAutonomous Ships ChallengesCristianAlbaArrietaNo ratings yet
- Absolute C 6th Edition Savitch Test BankDocument36 pagesAbsolute C 6th Edition Savitch Test Bankproteosemolehill.g1n1h100% (25)
- Ubuntu FeistyDocument242 pagesUbuntu FeistySlamet Budi SantosoNo ratings yet
- Crypt Arithmatic Problem SolutionDocument10 pagesCrypt Arithmatic Problem SolutionHariom Patel100% (4)
- Talent Acquisition 2008 - Survey and Analysis of The Changing Recruiting Landscape PDFDocument20 pagesTalent Acquisition 2008 - Survey and Analysis of The Changing Recruiting Landscape PDFVaishnavi SivaNo ratings yet
- LG 29FG1RL 12950 Chassis CW-62C Manual de ServicioDocument34 pagesLG 29FG1RL 12950 Chassis CW-62C Manual de Serviciopepe sanchezNo ratings yet
- SponsorDocument11 pagesSponsorMaulina SalmahNo ratings yet
- 6 Feasibility Assessment ToolDocument5 pages6 Feasibility Assessment Toolalibaba1888No ratings yet
- Bullock Cart: Aarushree KhobragadeDocument13 pagesBullock Cart: Aarushree KhobragadeAzure MidoriyaNo ratings yet
- Category:UR Madam / Sir,: Please Affix Your Recent Passport Size Colour Photograph & Sign AcrossDocument2 pagesCategory:UR Madam / Sir,: Please Affix Your Recent Passport Size Colour Photograph & Sign AcrossVasu Ram JayanthNo ratings yet
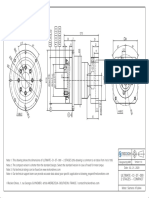
- ULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Document1 pageULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Francesco SchioppaNo ratings yet
- The Impact of Low Heat Load and Activated Carbon Treatment of Second Wort On Beer Taste and Flavour StabilityDocument8 pagesThe Impact of Low Heat Load and Activated Carbon Treatment of Second Wort On Beer Taste and Flavour StabilitySefa YücesoyNo ratings yet
- Instant Download Ebook PDF Dorlands Illustrated Medical Dictionary 32nd Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Dorlands Illustrated Medical Dictionary 32nd Edition PDF Scribdemiko.johnson659100% (44)
- 100 S Oem S: 102R Low Flow PumpheadDocument2 pages100 S Oem S: 102R Low Flow PumpheadtechniqueNo ratings yet
- Basic Computer SkillsDocument11 pagesBasic Computer SkillsreneeNo ratings yet
- REPORT Multiple DisabilitiesDocument8 pagesREPORT Multiple DisabilitiesIrene FriasNo ratings yet
- Website ErrorDocument5 pagesWebsite ErrorJosé DavidNo ratings yet
- PCR AslamkhanDocument1 pagePCR AslamkhanKoteswar MandavaNo ratings yet
- IA BrochureDocument12 pagesIA BrochureChris WallaceNo ratings yet
- CA Empanelment-Application FormatDocument5 pagesCA Empanelment-Application FormatPV REDDY AssociatesNo ratings yet
- Math Chapter 3 Study GuideDocument3 pagesMath Chapter 3 Study Guideapi-311999132No ratings yet
- Chapter 3 CVPDocument26 pagesChapter 3 CVPshuhadaNo ratings yet
- Simple Past TenseDocument3 pagesSimple Past TenseClara UbaltonNo ratings yet
- An Experiment of DensityDocument4 pagesAn Experiment of DensitySamuel TumewaNo ratings yet
- General Chemistry 1: Matter and Its PropertiesDocument35 pagesGeneral Chemistry 1: Matter and Its PropertiesRomalyn MoralesNo ratings yet
- Core Timers T305 T308 FinalDocument14 pagesCore Timers T305 T308 FinalSana UllahNo ratings yet
- Bomba 750 GPM 130 McaDocument1 pageBomba 750 GPM 130 McaEDWIN HUMBERTO QUICENO CANONo ratings yet