Download as pdf or txt
You might also like
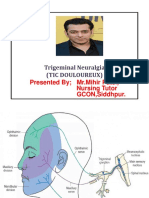
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- BS 8110Document9 pagesBS 8110Priyadarshini Sahoo100% (1)
- Chemrite Grout NSDocument2 pagesChemrite Grout NSghazanfar0% (1)
- Trigeminal Neuralgia: Dr. Deepthi AthuluruDocument69 pagesTrigeminal Neuralgia: Dr. Deepthi AthuluruLakshya NainNo ratings yet
- Neuralgia TrigeminalDocument5 pagesNeuralgia TrigeminalcantikarevieraNo ratings yet
- Trigeminal NeurlgiaDocument5 pagesTrigeminal NeurlgiaAnonymous V1tCwPHlDNo ratings yet
- Trigeminal NeuralgiaDocument5 pagesTrigeminal Neuralgiawidad syairoziNo ratings yet
- Pathophysiology, Causes, and Differential Diagnosis: Multiple SclerosisDocument4 pagesPathophysiology, Causes, and Differential Diagnosis: Multiple SclerosisjaideepbaggaNo ratings yet
- Trigeminal Neuralgia PDFDocument4 pagesTrigeminal Neuralgia PDFCHenyLeeNo ratings yet
- Trigeminal NeuralgiaDocument7 pagesTrigeminal NeuralgiaEricsonMitraNo ratings yet
- What Is Trigeminal NeuralgiaDocument3 pagesWhat Is Trigeminal NeuralgiakewpietheresaNo ratings yet
- Trigeminal NeuralgiaDocument54 pagesTrigeminal NeuralgiaSarah Khan100% (1)
- Trigeminal Neuralgia and Its Management: Data Supplement ReferencesDocument6 pagesTrigeminal Neuralgia and Its Management: Data Supplement ReferencesfendiNo ratings yet
- Mendoza Outline of DiseasesDocument28 pagesMendoza Outline of DiseasesAleks MendozaNo ratings yet
- What Is Trigeminal Neuralgia?Document4 pagesWhat Is Trigeminal Neuralgia?Tiger_2011No ratings yet
- Wilhour-Nahas2018 Article The NeuralgiasDocument8 pagesWilhour-Nahas2018 Article The NeuralgiasCamilo Benavides BurbanoNo ratings yet
- TN OverviewDocument6 pagesTN OverviewNursing DepartmentNo ratings yet
- Trigeminal Neuralgia DMDocument12 pagesTrigeminal Neuralgia DMPermata GBKP Runggun SurabayaNo ratings yet
- Rehabilitation of Patients Suffering Trigeminal Nerve NeuragiaDocument22 pagesRehabilitation of Patients Suffering Trigeminal Nerve NeuragiacosornoNo ratings yet
- Trigeminal NeuralgiaDocument3 pagesTrigeminal NeuralgiaAira Alaro50% (2)
- Acc 61 - Supp2 96Document7 pagesAcc 61 - Supp2 96intermediosamberesNo ratings yet
- Trigeminal NeuralgiaDocument6 pagesTrigeminal NeuralgiamimirkuNo ratings yet
- 15.trigeminal NeuralgiaDocument25 pages15.trigeminal NeuralgiaBhakti WashilkarNo ratings yet
- Diseases of The Nerves and MusclesDocument17 pagesDiseases of The Nerves and MusclesHadil AltilbaniNo ratings yet
- Overview of Craniofacial Pain - UpToDateDocument24 pagesOverview of Craniofacial Pain - UpToDateNana ShkodinaNo ratings yet
- Orofacial PainDocument40 pagesOrofacial Painghazy100% (1)
- 7vol6issue5p28-32 20200918050408Document5 pages7vol6issue5p28-32 20200918050408SkAliHassanNo ratings yet
- Trigeminal Neuralgi (Kuliah)Document26 pagesTrigeminal Neuralgi (Kuliah)shofyan_2005_yarsiNo ratings yet
- Trigeminal Neuralgia Overview: Sleep Anxiety Depression Malnutrition SuicidalDocument57 pagesTrigeminal Neuralgia Overview: Sleep Anxiety Depression Malnutrition SuicidalAmy Rose EugenioNo ratings yet
- Trigeminal Neuralgia: DR Tay Kwang Hui Dept of Anaesthesia 08 January 2011Document40 pagesTrigeminal Neuralgia: DR Tay Kwang Hui Dept of Anaesthesia 08 January 2011Shalim BagusNo ratings yet
- Trigeminal NeuralgiaDocument3 pagesTrigeminal NeuralgiaPao JeyNo ratings yet
- Management Trigeminal NeuralgiaDocument28 pagesManagement Trigeminal NeuralgiaApeksha JadhavNo ratings yet
- Differentiating Trigeminal Neuropathy From Trigeminal NeuralgiaDocument11 pagesDifferentiating Trigeminal Neuropathy From Trigeminal NeuralgiaGarryNo ratings yet
- Trigeminal NeuralgiaDocument18 pagesTrigeminal NeuralgiaKaran KohliNo ratings yet
- Trigeminal Neuralgia Recent Approach in ClassificaDocument9 pagesTrigeminal Neuralgia Recent Approach in ClassificaFKUPR 2017No ratings yet
- Trigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, SiddhpurDocument15 pagesTrigeminal Neuralgia (Tic Douloureux) : Presented by MR - Mihir Patel, Nursing Tutor GCON, Siddhpurandreas kevinNo ratings yet
- 7 TrigeminalNeuralgia PDFDocument2 pages7 TrigeminalNeuralgia PDFGursimran PannuNo ratings yet
- Management of NeuralgiaDocument2 pagesManagement of NeuralgiaNeivashini MaDhavanNo ratings yet
- Differential Diagnosis of NICODocument13 pagesDifferential Diagnosis of NICOscribdmikaelNo ratings yet
- Fact Sheet Trigeminal NeuralgiaDocument2 pagesFact Sheet Trigeminal Neuralgiasarmad78No ratings yet
- Neurosurgical Treatment of Pain - AishuDocument24 pagesNeurosurgical Treatment of Pain - AishuAishwarya PoojaryNo ratings yet
- Trigeminal Neuralgia Outline ScriptDocument4 pagesTrigeminal Neuralgia Outline ScriptRogerQuxNo ratings yet
- Pemicu 1: Blok Sistem Saraf Dan KejiwaanDocument50 pagesPemicu 1: Blok Sistem Saraf Dan KejiwaancecilliacynthiaNo ratings yet
- Lapsus Ablasi Radiofrekuensi Pada Neuralgia Trigeminal Dengan Panduan FluoroskopiDocument8 pagesLapsus Ablasi Radiofrekuensi Pada Neuralgia Trigeminal Dengan Panduan FluoroskopivalenciaNo ratings yet
- Cranial Neuralgia Keynote PDFDocument21 pagesCranial Neuralgia Keynote PDFRuki HartawanNo ratings yet
- Neuralgia Del TrigeminoDocument10 pagesNeuralgia Del TrigeminoDanni MontielNo ratings yet
- B. Wayne Blount, MD, MPHDocument28 pagesB. Wayne Blount, MD, MPHSanjaya Deeptha ThennakoonNo ratings yet
- Trigeminal Neuralgia (Facial Pain)Document6 pagesTrigeminal Neuralgia (Facial Pain)Aisyah AlviNo ratings yet
- Trigeminal Neuralgia: FJ Dowd, Creighton University School of Medicine, Omaha, NE, USADocument5 pagesTrigeminal Neuralgia: FJ Dowd, Creighton University School of Medicine, Omaha, NE, USAWalter Espinoza CiertoNo ratings yet
- Orofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsDocument49 pagesOrofacial Pain: DR Samreen Younas Pgr-I (FCPS) OmfsmishaNo ratings yet
- Facial Pain PDFDocument4 pagesFacial Pain PDFSuprit SnNo ratings yet
- NerualgiaDocument7 pagesNerualgiaKabirNo ratings yet
- Orofacial PainDocument6 pagesOrofacial PainAnnaNguyenNo ratings yet
- A Case of Occipital NeuralgiaDocument20 pagesA Case of Occipital NeuralgiaLakNo ratings yet
- The Neuralgias Diagnosis and Management Curr Neurol Neurosci Rep 2014Document8 pagesThe Neuralgias Diagnosis and Management Curr Neurol Neurosci Rep 2014Fernando BravoNo ratings yet
- Trigeminal Neuralgia Oral SurgeryDocument48 pagesTrigeminal Neuralgia Oral SurgeryFourthMolar.com67% (3)
- Trigeminal Neuralgia (Tic Douloureux)Document49 pagesTrigeminal Neuralgia (Tic Douloureux)Mohsin HabibNo ratings yet
- Dolor NeuropaticoDocument21 pagesDolor NeuropaticoMarco Antonio García LunaNo ratings yet
- Oro Facial Pain Part 2 2022Document27 pagesOro Facial Pain Part 2 2022pxb8dhqgs9No ratings yet
- Management of Trigeminal Neuralgia. A Comparison of Two TechniquesDocument20 pagesManagement of Trigeminal Neuralgia. A Comparison of Two TechniquesAbhikNo ratings yet
- Intralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?From EverandIntralipid infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?No ratings yet
- A Simple Guide to Neuralgia and Related Nerve DisordersFrom EverandA Simple Guide to Neuralgia and Related Nerve DisordersRating: 5 out of 5 stars5/5 (5)
- Fartlek - WikipediaDocument7 pagesFartlek - Wikipediamohan raoNo ratings yet
- Lesson 2 Discrete Probability DistributionsDocument11 pagesLesson 2 Discrete Probability DistributionsReign SaplacoNo ratings yet
- Best Practice & Research Clinical RheumatologyDocument15 pagesBest Practice & Research Clinical RheumatologyTatiana GonzalezNo ratings yet
- Offshore Wind FarmDocument32 pagesOffshore Wind FarmKonstantinos Papadopoulos100% (1)
- Sapphire Hi-Pressure 2 TdsDocument2 pagesSapphire Hi-Pressure 2 TdsfahreezNo ratings yet
- Assessment and Transportation Risk-1Document7 pagesAssessment and Transportation Risk-1TanzeemNo ratings yet
- Contoh Praktis Menggunakan EVIEWSDocument46 pagesContoh Praktis Menggunakan EVIEWSDidi JunaediNo ratings yet
- Body ThesisDocument408 pagesBody ThesissridharanNo ratings yet
- Nisarg CSCDocument34 pagesNisarg CSCNarendra MehtaNo ratings yet
- Membean RootsDocument14 pagesMembean RootsMuhammad Sohail SialNo ratings yet
- Grade 9 TOSDocument4 pagesGrade 9 TOSManuel EsponillaNo ratings yet
- Of Truth by Francis Bacon: Notes PDF Is in The Description Box of This VideoDocument8 pagesOf Truth by Francis Bacon: Notes PDF Is in The Description Box of This VideoMuhammad NomanNo ratings yet
- Un Român, Aeronaut În Polonia, La Începutul Secolului Al Xix - Lea: Iordache CuparencuDocument26 pagesUn Român, Aeronaut În Polonia, La Începutul Secolului Al Xix - Lea: Iordache CuparencuCodrin Codrin100% (1)
- Pre-Excavation ChecklistDocument2 pagesPre-Excavation ChecklistminimeezyNo ratings yet
- QUINTA DE PACOS PresentationDocument2 pagesQUINTA DE PACOS PresentationBeatrice ŞtefaniaNo ratings yet
- Manual Haier HYC-390 enDocument24 pagesManual Haier HYC-390 enDaniel BuitragoNo ratings yet
- Review - 1 Faculty: Manikandan Slot: Tb1 Course: Introduction To The Innovative Physics Projects (Phy1999)Document6 pagesReview - 1 Faculty: Manikandan Slot: Tb1 Course: Introduction To The Innovative Physics Projects (Phy1999)RamNo ratings yet
- Cambridge Secondary 1 Checkpoint: Cambridge Assessment International EducationDocument7 pagesCambridge Secondary 1 Checkpoint: Cambridge Assessment International Educationigloo79No ratings yet
- Vann Air ValveDocument4 pagesVann Air ValveDedeLesmanaNo ratings yet
- Kings Meadows Public ToiletDocument16 pagesKings Meadows Public ToiletThe ExaminerNo ratings yet
- Can CommunicationDocument139 pagesCan CommunicationMirceaNo ratings yet
- Introduction To Sports: Sports Benefits of Playing SportDocument7 pagesIntroduction To Sports: Sports Benefits of Playing SportMa. Karyl Ashrivelle CarreonNo ratings yet
- Fire Pump Field Acceptance TestDocument23 pagesFire Pump Field Acceptance Testwalitedison100% (1)
- Principles and Interpretation of CardiotocographyDocument9 pagesPrinciples and Interpretation of CardiotocographyCKNo ratings yet
- Straight / Angulated Multi-Unit System: © MIS Corporation. All Rights ReservedDocument12 pagesStraight / Angulated Multi-Unit System: © MIS Corporation. All Rights ReservedKrupali JainNo ratings yet
- Dispersion PollutantsDocument18 pagesDispersion PollutantsAmira GogoantaNo ratings yet
- GY 112 Lecture NotesDocument13 pagesGY 112 Lecture NotesSyed Jabed Miadad AliNo ratings yet
- Project 89 May 2012 UpdateDocument73 pagesProject 89 May 2012 UpdategonflynnNo ratings yet