Download as pdf or txt
You might also like
- Final Exam NRNP-6531 Advanced PracticeDocument21 pagesFinal Exam NRNP-6531 Advanced PracticeGeorge Ekai100% (4)
- MLS ASCP Exam Recall Questions Flashcards - QuizletDocument8 pagesMLS ASCP Exam Recall Questions Flashcards - Quizletyeliz kurt100% (3)
- MKSAP 16 - Infectious DiseaseDocument340 pagesMKSAP 16 - Infectious DiseaseBacanator75% (4)
- (HOT) AMC MCQ Recalls 2020Document33 pages(HOT) AMC MCQ Recalls 2020Gofi100% (1)
- Sle Prometric August 2011 RiyadhDocument10 pagesSle Prometric August 2011 RiyadhWardah Tariq Malik100% (7)
- Problem Solving in RheumatologyDocument293 pagesProblem Solving in RheumatologyGaudeamus IgiturNo ratings yet
- Immunology Exam Questions SampleDocument14 pagesImmunology Exam Questions Sampleseviee86% (14)
- Comply With Infection Prevention and Control Policies and ProceduresDocument42 pagesComply With Infection Prevention and Control Policies and Procedurespavan0% (1)
- Meningitis and Lumbar PunctureDocument38 pagesMeningitis and Lumbar PunctureJeo ThomasNo ratings yet
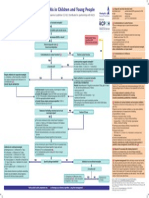
- Bacterial Meningitis and Meningococcal Septicaemia in Under 16s Diagnosis of Bacterial Meningitis and Meningococcal Septicaemia in Secondary CareDocument16 pagesBacterial Meningitis and Meningococcal Septicaemia in Under 16s Diagnosis of Bacterial Meningitis and Meningococcal Septicaemia in Secondary CareNatalia E PenagosNo ratings yet
- HemeOnc - Fever and Neutropenia 2013Document3 pagesHemeOnc - Fever and Neutropenia 2013Andrew McGowanNo ratings yet
- Journal Read ChiaDocument14 pagesJournal Read ChiaChris Tine ChiaNo ratings yet
- Evidence Based Medicine To Cut or Not To CutDocument98 pagesEvidence Based Medicine To Cut or Not To CutMikhail BrionesNo ratings yet
- Evaluation of In-Patients With FeverDocument125 pagesEvaluation of In-Patients With FeverStangPongritNo ratings yet
- Mastering MRCP Vol2Document348 pagesMastering MRCP Vol2mostachek88% (8)
- Introduction To The Principles of Laboratory MedicineDocument19 pagesIntroduction To The Principles of Laboratory MedicineKelvin L. CafirmaNo ratings yet
- Introduction To The Principles of Laboratory MedicineDocument19 pagesIntroduction To The Principles of Laboratory Medicinedanielle kaye arangoteNo ratings yet
- Bcps Preparatory Class On Pediatrics: Saba Javed HussainDocument65 pagesBcps Preparatory Class On Pediatrics: Saba Javed HussainSyahrul Tuba Al FatihNo ratings yet
- CK Recalls 1Document12 pagesCK Recalls 1nreena aslam100% (3)
- PPS WISE Questionnaire - 2nd Year_WISE 2022 FinalDocument23 pagesPPS WISE Questionnaire - 2nd Year_WISE 2022 FinalPunsalan ChecaNo ratings yet
- RITE Practice QuestionsDocument28 pagesRITE Practice QuestionsDesiree Mejica100% (2)
- Bux PresentationDocument17 pagesBux Presentationapi-648757084No ratings yet
- PediaDocument20 pagesPediaMedha ReddyNo ratings yet
- Bacterial Meningitis in Children - DynaMedDocument88 pagesBacterial Meningitis in Children - DynaMedCarlos CalderwoodNo ratings yet
- NSG 6340 Final Exam 1.........Document9 pagesNSG 6340 Final Exam 1.........Tom0% (1)
- Quiz Critical CareDocument15 pagesQuiz Critical CareSuma AhmadNo ratings yet
- 0221 Community-Acquired-PneumoniaDocument29 pages0221 Community-Acquired-PneumoniaDiego YanezNo ratings yet
- Case scenario-VIROLOGYDocument5 pagesCase scenario-VIROLOGYsanjeev09122005No ratings yet
- 10.1007@s12098 020 03454 1Document6 pages10.1007@s12098 020 03454 1rayhantaswinNo ratings yet
- BiemansDocument13 pagesBiemansPaco MsnroNo ratings yet
- Diagnosis and Treatment of Bacterial Meningitis: Arch. Dis. ChildDocument7 pagesDiagnosis and Treatment of Bacterial Meningitis: Arch. Dis. Childapi-214563632No ratings yet
- Junal PyodermaDocument6 pagesJunal PyodermaJares Clinton Saragih SimarmataNo ratings yet
- Tuberculosis NclexDocument3 pagesTuberculosis NclexMarinill SolimanNo ratings yet
- Case 10 Fever PDFDocument5 pagesCase 10 Fever PDFSue HuangNo ratings yet
- Weekly Task at Pediatric Intensive Unite (Picu) 1Document9 pagesWeekly Task at Pediatric Intensive Unite (Picu) 1Reem ApadiNo ratings yet
- More Than A Sore ThroatDocument17 pagesMore Than A Sore ThroatEmily EresumaNo ratings yet
- Guideline MeningitisDocument1 pageGuideline MeningitisAmbc Smfk-uaj100% (1)
- Chapter 04 - Immunologic ProblemsDocument7 pagesChapter 04 - Immunologic ProblemscariNo ratings yet
- LMS: View Results: No Question Type Weightage Questions Associate Answers Score StatusDocument5 pagesLMS: View Results: No Question Type Weightage Questions Associate Answers Score StatusRaja SolaimalaiNo ratings yet
- Penatalaksanaan CAPDocument31 pagesPenatalaksanaan CAPridhoNo ratings yet
- Journal of Pediatric HematologyDocument10 pagesJournal of Pediatric HematologyasepNo ratings yet
- Nephro Gudie For HODocument22 pagesNephro Gudie For HOSarmad AsifNo ratings yet
- Covid 19 Guidelines April 2021Document42 pagesCovid 19 Guidelines April 2021K.sushmaNo ratings yet
- Ob Part 2Document7 pagesOb Part 2gmik02No ratings yet
- Inflammation ReviewerDocument17 pagesInflammation ReviewerAinee MeuvinNo ratings yet
- Pediatric Hematology Oncology CaseDocument107 pagesPediatric Hematology Oncology CaseSayyed Ahmad KhursheedNo ratings yet
- Microbiology MMV-Sample-MCQsDocument8 pagesMicrobiology MMV-Sample-MCQsMuhammad AttiqueNo ratings yet
- Immune Complex Complications MeningococcemiaDocument4 pagesImmune Complex Complications MeningococcemiaElena EllaNo ratings yet
- Medical Therapeutics Journal Appraisal 3B 2009-70197: 1. Is It Relevant?Document4 pagesMedical Therapeutics Journal Appraisal 3B 2009-70197: 1. Is It Relevant?Maria Christina SalazarNo ratings yet
- Infectious Diseases IIDocument57 pagesInfectious Diseases IIAhmad Makhlouf100% (1)
- Journal Report (OB) - Neonatal SepsisDocument6 pagesJournal Report (OB) - Neonatal SepsisAllan Alejandro SevillaNo ratings yet
- SOP Neutropenic PatientDocument7 pagesSOP Neutropenic Patientdrsp2001No ratings yet
- SOP Neutropenic PatientDocument7 pagesSOP Neutropenic Patientdrsp2001No ratings yet
- Typhoid Blood Test ReportDocument3 pagesTyphoid Blood Test ReportPranay BhosaleNo ratings yet
- Neonatal Sepsis: Prof DR Saima BatoolDocument31 pagesNeonatal Sepsis: Prof DR Saima BatoolSAIMA BATOOLNo ratings yet
- 10 1016@j Jaad 2012 12 513Document1 page10 1016@j Jaad 2012 12 513Kuro ChanNo ratings yet
- Sepsis NeonatalDocument21 pagesSepsis NeonatalRaissa 'Icha' Nurwany RizalNo ratings yet
- 2nd IA Portions and QuestionsDocument6 pages2nd IA Portions and Questionsjaisurya srinivasanNo ratings yet
- Intermediate Coding 2012Document13 pagesIntermediate Coding 2012Umarani MohanasundaramNo ratings yet
- 6 - Infectious DiseasesDocument35 pages6 - Infectious DiseasesTalaat OmranNo ratings yet
- Enarm Train Quiz WoaDocument231 pagesEnarm Train Quiz WoaJohon Lou MartinezNo ratings yet
- Tuberculosis in ChildrenDocument4 pagesTuberculosis in ChildrenMarthin TheservantNo ratings yet
- Case Report JurnalDocument16 pagesCase Report JurnalAstrid PuspaNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Major Changes in Revised NSSKDocument2 pagesMajor Changes in Revised NSSKOleOhhNo ratings yet
- Villanueva 2016Document4 pagesVillanueva 2016OleOhhNo ratings yet
- Neuro Exam and Localization For The InternistDocument6 pagesNeuro Exam and Localization For The InternistOleOhhNo ratings yet
- Reflection: 24 - Dr.R.Thamilselvi - Pinky Ponky - ACME 12 - 2021B - 2.6C - Programmatic Assessment - Topic - 2 ReflectionDocument2 pagesReflection: 24 - Dr.R.Thamilselvi - Pinky Ponky - ACME 12 - 2021B - 2.6C - Programmatic Assessment - Topic - 2 ReflectionOleOhhNo ratings yet
- Revised Budgets NRP - Advanced NRP 2022Document4 pagesRevised Budgets NRP - Advanced NRP 2022OleOhhNo ratings yet
- Dr. G. Sivakumar M.D., (Anaes) : Department of PaediatricsDocument1 pageDr. G. Sivakumar M.D., (Anaes) : Department of PaediatricsOleOhhNo ratings yet
- TUTY - Infant Death Baby of Muthumari-003Document1 pageTUTY - Infant Death Baby of Muthumari-003OleOhhNo ratings yet
- Tuty-Hud - Id - Sep-22Document3 pagesTuty-Hud - Id - Sep-22OleOhhNo ratings yet
- Initial Assesment FormDocument4 pagesInitial Assesment FormOleOhhNo ratings yet
- UntitledDocument1 pageUntitledOleOhhNo ratings yet
- BACKGROUND: Through Thrombolysis Is The Ideal Treatment For CardiacDocument2 pagesBACKGROUND: Through Thrombolysis Is The Ideal Treatment For CardiacOleOhhNo ratings yet
- UntitledDocument1 pageUntitledOleOhhNo ratings yet
- UntitledDocument2 pagesUntitledOleOhhNo ratings yet
- Crmi - Pediatrics NMC 2021 RegulationsDocument2 pagesCrmi - Pediatrics NMC 2021 RegulationsOleOhhNo ratings yet
- Metabolic Acidosis: DR - Vijula.A, Junior Resident, MD General Medicine, Thoothukudi Medical College and HospitalDocument1 pageMetabolic Acidosis: DR - Vijula.A, Junior Resident, MD General Medicine, Thoothukudi Medical College and HospitalOleOhhNo ratings yet
- BibiliographyDocument5 pagesBibiliographyOleOhhNo ratings yet
- UntitledDocument1 pageUntitledOleOhhNo ratings yet
- Strategies Advantages Dis-AdvantagesDocument3 pagesStrategies Advantages Dis-AdvantagesOleOhhNo ratings yet
- Programmatic Assessment: Turning Process Into Practice by Teaching For LearningDocument8 pagesProgrammatic Assessment: Turning Process Into Practice by Teaching For LearningOleOhhNo ratings yet
- Diabetic KetoacidosisDocument1 pageDiabetic KetoacidosisOleOhhNo ratings yet
- Hypoparathyroidism: A Clinical Casebook Natalie E. CusanoDocument15 pagesHypoparathyroidism: A Clinical Casebook Natalie E. CusanoOleOhhNo ratings yet
- Multicentric Hospital-Based Surveillance of Pertussis Amongst Infants Admitted in Tertiary Care Facilities in IndiaDocument11 pagesMulticentric Hospital-Based Surveillance of Pertussis Amongst Infants Admitted in Tertiary Care Facilities in IndiaOleOhhNo ratings yet
- Diploma Pediatric Allergy and Asthma (DPAA) : The Ganga Ram Institute For Postgraduate Medical Education and ResearchDocument8 pagesDiploma Pediatric Allergy and Asthma (DPAA) : The Ganga Ram Institute For Postgraduate Medical Education and ResearchOleOhhNo ratings yet
- Introduction & Objectives: Nishad Plakkal Associate Professor Department of Neonatology, JIPMERDocument13 pagesIntroduction & Objectives: Nishad Plakkal Associate Professor Department of Neonatology, JIPMEROleOhhNo ratings yet
- Literature Summary: DKA and Cerebral EdemaDocument2 pagesLiterature Summary: DKA and Cerebral EdemaOleOhhNo ratings yet
- Problem Based Learning: Case StudyDocument27 pagesProblem Based Learning: Case StudyOleOhhNo ratings yet
- CBC (Adult)Document1 pageCBC (Adult)MAYE AMARNo ratings yet
- Scleritis and EpiscleritisDocument27 pagesScleritis and EpiscleritisJT RodierNo ratings yet
- FIGURE: Haemobartonella Felis in Blood From A Cat. Organisms Appear As Small Cocci, Rods, orDocument3 pagesFIGURE: Haemobartonella Felis in Blood From A Cat. Organisms Appear As Small Cocci, Rods, orabdulNo ratings yet
- Non Specific and Specific Host Defense MechanismDocument7 pagesNon Specific and Specific Host Defense Mechanismcheskhadomingo33No ratings yet
- Melinda PechaycoDocument30 pagesMelinda PechaycoChristian Paul ChuaNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- Bpac Antibiotics Booklet PDFDocument20 pagesBpac Antibiotics Booklet PDFVenny Tri Pahlevi IINo ratings yet
- Presentation 3Document14 pagesPresentation 3olayemi morakinyoNo ratings yet
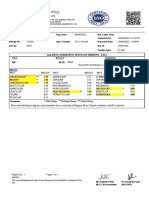
- Allergy Screening Tests (By Immuno - Eia)Document1 pageAllergy Screening Tests (By Immuno - Eia)Patel DhruviNo ratings yet
- Management of Infection Guidance For Primary Care in IrelandDocument29 pagesManagement of Infection Guidance For Primary Care in IrelandLouise GleesonNo ratings yet
- Haemobartonellosis in A Domestic Cat in Indonesia: A Case StudyDocument4 pagesHaemobartonellosis in A Domestic Cat in Indonesia: A Case StudyBima Ary WibowoNo ratings yet
- Chapter 10Document24 pagesChapter 10Kandarpa SaikiaNo ratings yet
- Arayat Holy Child Educational Foundation Inc.: Medicine A of 12 STEM 3Document9 pagesArayat Holy Child Educational Foundation Inc.: Medicine A of 12 STEM 3Lamour ManlapazNo ratings yet
- A Hefty Volume: Immunology and Molecular Biology of Parasitic InfectionsDocument1 pageA Hefty Volume: Immunology and Molecular Biology of Parasitic InfectionsRichard TamreNo ratings yet
- Coxsackievirus: Presented By: LKCDocument18 pagesCoxsackievirus: Presented By: LKCLeang KarichakNo ratings yet
- Withania Somnifera As An ImmunomodulatorDocument8 pagesWithania Somnifera As An ImmunomodulatorNorin MemonNo ratings yet
- Biopharmaceu Tical Classification System (BCS) Class IIDocument2 pagesBiopharmaceu Tical Classification System (BCS) Class IIGULSHAN MADHURNo ratings yet
- WHO Global Pandemic Phases and The Stages For Federal Government ResponseDocument4 pagesWHO Global Pandemic Phases and The Stages For Federal Government ResponseMara Luisa PanopioNo ratings yet
- Chapter 15 Nematode Study GuideDocument3 pagesChapter 15 Nematode Study GuideKristine Marie PateñoNo ratings yet
- Description: Aloedetox - From Premier Research LabsDocument5 pagesDescription: Aloedetox - From Premier Research LabsahceneNo ratings yet
- Lecture 1 - PsoriasisDocument5 pagesLecture 1 - PsoriasismaryannejkiemNo ratings yet
- Clinical: GuidelinesDocument58 pagesClinical: Guidelinesdonovandube8235No ratings yet
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Tetanus Toxoid VaccinationDocument26 pagesTetanus Toxoid Vaccinationdevon dirgahayuNo ratings yet
- Is An Ancient Disease That Causes Permanent Physical Disability AmongDocument6 pagesIs An Ancient Disease That Causes Permanent Physical Disability Amongkian5No ratings yet
- Emerging, Re-Emerging Infectious Diseases and Neglected TropicalDocument32 pagesEmerging, Re-Emerging Infectious Diseases and Neglected TropicalMelia100% (1)