
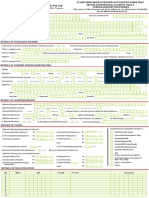
Health Insurance Claim Form
Health Insurance Claim Form
You might also like
- Phtls 9th Edition UpdateDocument36 pagesPhtls 9th Edition Updatealfred dahbi67% (9)
- Evidence Based Nursing PracticeDocument21 pagesEvidence Based Nursing PracticeChithra Saju71% (7)
- Dementia Research ProposalDocument12 pagesDementia Research ProposalOmowunmiItunuNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistorySwapnil NageNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Primary InsuredDocument8 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Primary InsuredHimansh ChandakNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- HDFC ERGO General Insurance Company LimitedDocument6 pagesHDFC ERGO General Insurance Company LimitedShibani DesaiNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ADocument6 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ARamesh WalkeNo ratings yet
- Claim Reimbursement FormDocument7 pagesClaim Reimbursement FormBagavathi RNo ratings yet
- Claim Form 10 - EditableDocument9 pagesClaim Form 10 - EditableharshiNo ratings yet
- Claim Form: Claim Form Part A Section A - Details of Primary InsuredDocument8 pagesClaim Form: Claim Form Part A Section A - Details of Primary InsuredAnonymous d8d8k1LiyNo ratings yet
- ReimbursementFormA B2016Document7 pagesReimbursementFormA B2016DESIGN CGMPNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- Health Insurance - Claim Form - Part A (To Be Filled by Insured)Document4 pagesHealth Insurance - Claim Form - Part A (To Be Filled by Insured)Shaikh AyyubNo ratings yet
- Health File3Document9 pagesHealth File3kulbirplusNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- ProHealth V7 ClaimFormA April23Document7 pagesProHealth V7 ClaimFormA April23njthakkarNo ratings yet
- E Claim FormDocument8 pagesE Claim FormronNo ratings yet
- Reimbursement Claim FormDocument10 pagesReimbursement Claim FormranjanNo ratings yet
- ProHealth Cash Claim A March2021 V3 V3Document7 pagesProHealth Cash Claim A March2021 V3 V3Harsh MandaniNo ratings yet
- Reimbursement A PDFDocument4 pagesReimbursement A PDFAniruddha ShivalNo ratings yet
- Details of Primary Insured: Bajaj Allianz General Insurance Company LimitedDocument3 pagesDetails of Primary Insured: Bajaj Allianz General Insurance Company LimitedBellapu Durga vara prasadNo ratings yet
- Claim Form GMCDocument7 pagesClaim Form GMCBhaskar RawatNo ratings yet
- EH Claim FormDocument8 pagesEH Claim FormAmol PakhaleNo ratings yet
- ClaimFormDocument6 pagesClaimFormKanhaiya Lal SahuNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyMruthunjaya Reddy LakkamNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet
- Magma Claim FormDocument4 pagesMagma Claim FormAbhinav JaganaNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Reimbursement CLaim Form IRDADocument5 pagesReimbursement CLaim Form IRDADhaval ThakkarNo ratings yet
- Reimbursement Claim Form-1Document7 pagesReimbursement Claim Form-1Mayuresh DalviNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone No ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyArunsNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicySudipta DeNo ratings yet
- 05-01-2022 - Manuj Om HospitalisationDocument20 pages05-01-2022 - Manuj Om HospitalisationManuj RathoreNo ratings yet
- Group Mediprime Claim FormDocument8 pagesGroup Mediprime Claim FormRahulNo ratings yet
- Claim Form - Part A: To Be Filled in by The InsuredDocument2 pagesClaim Form - Part A: To Be Filled in by The InsuredAli ArsalaanNo ratings yet
- Easy Health Insurance Claim Form PDFDocument4 pagesEasy Health Insurance Claim Form PDFAnkithNo ratings yet
- AMHI-new Claim Form PDFDocument4 pagesAMHI-new Claim Form PDFQwerty TNo ratings yet
- To Be Filled in by The Insured: Details of Primary InsuredDocument4 pagesTo Be Filled in by The Insured: Details of Primary Insurednaveen pointNo ratings yet
- Claim Form Part ADocument8 pagesClaim Form Part AJos'fAntonyRinoNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- Veneer Classification .PDGDocument10 pagesVeneer Classification .PDGAndykaYayanSetiawanNo ratings yet
- The Effects of Auditory Hallucination Symptom ManagementDocument12 pagesThe Effects of Auditory Hallucination Symptom ManagementAndika FahruroziNo ratings yet
- Severe Acute Malnutrition - ManagementDocument14 pagesSevere Acute Malnutrition - ManagementArkadeb Kar100% (1)
- The Benefits of An Ageing PopulationDocument9 pagesThe Benefits of An Ageing PopulationYa LiNo ratings yet
- ASA PS Classifications From The American Society of AnesthesiologistsDocument1 pageASA PS Classifications From The American Society of AnesthesiologistsaffifulichwanNo ratings yet
- Retail Sale Drugs License AFFIDAVITDocument40 pagesRetail Sale Drugs License AFFIDAVITIndranil DattaNo ratings yet
- NCD Project: Togu Marpaung, MDDocument11 pagesNCD Project: Togu Marpaung, MDTogu MarpaungNo ratings yet
- Healthcare Predictive Analytics Using Machine Learning and Deep Learning Techniques: A SurveyDocument45 pagesHealthcare Predictive Analytics Using Machine Learning and Deep Learning Techniques: A SurveyMuhammad Sadiq Khan NasarNo ratings yet
- LEGASPI Nomination Papers For PGH Directorship (2015)Document6 pagesLEGASPI Nomination Papers For PGH Directorship (2015)karl_poorNo ratings yet
- Narrative ReportDocument3 pagesNarrative ReportCamille De PaduaNo ratings yet
- Test Bank For Mosbys Textbook For Nursing Assistants 9th Edition by SorrentinoDocument11 pagesTest Bank For Mosbys Textbook For Nursing Assistants 9th Edition by Sorrentinodiodontmetacism.0jw2al100% (46)
- National Mediclaim Policy PDFDocument19 pagesNational Mediclaim Policy PDFTanmoy Pal ChowdhuryNo ratings yet
- NTB ppt-1Document76 pagesNTB ppt-1yazgariNo ratings yet
- Updated Resume 11 19Document2 pagesUpdated Resume 11 19api-454845978No ratings yet
- Cuong Vong - Resume - RevisedDocument2 pagesCuong Vong - Resume - Revisedapi-300295160No ratings yet
- Spirituality, Religion and Mental IllnessDocument9 pagesSpirituality, Religion and Mental IllnessJericho CabelloNo ratings yet
- Tamayo - History of Psychiatric NursingDocument1 pageTamayo - History of Psychiatric NursingVictoria Castillo TamayoNo ratings yet
- Patient History Taking TemplateDocument2 pagesPatient History Taking TemplateVarshini Tamil SelvanNo ratings yet
- Nurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanDocument5 pagesNurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement Planzadem5266No ratings yet
- SC DHEC Infant Mortality Rate ReportDocument40 pagesSC DHEC Infant Mortality Rate ReportABC15 NewsNo ratings yet
- Sreevidya Nair - PresentationDocument16 pagesSreevidya Nair - PresentationArk GroupNo ratings yet
- Organizational StructureDocument61 pagesOrganizational Structuretahira ahmedNo ratings yet
- Myanmar LNGO Directory 2012Document138 pagesMyanmar LNGO Directory 2012kk_mangneo100% (1)
- Family Names of DrugsDocument1 pageFamily Names of DrugsangelNo ratings yet
- Abhijeet Singh Ankit Kr. Agrawal (3C) Vaibhav Gupta Pankul Gupta Prateek MittalDocument13 pagesAbhijeet Singh Ankit Kr. Agrawal (3C) Vaibhav Gupta Pankul Gupta Prateek MittalAbhijeet SinghNo ratings yet
- Tanzania National Strategic Plan For The Control of Viral Hepatitis 2018-19-2022-23Document72 pagesTanzania National Strategic Plan For The Control of Viral Hepatitis 2018-19-2022-23daniel mwanduNo ratings yet
- NCMA113 FUNDA SKILL 2 Donning Doffing PPEsDocument4 pagesNCMA113 FUNDA SKILL 2 Donning Doffing PPEsJessoliver GalvezNo ratings yet























































































Download as pdf or txt
You might also like
- Phtls 9th Edition UpdateDocument36 pagesPhtls 9th Edition Updatealfred dahbi67% (9)
- Evidence Based Nursing PracticeDocument21 pagesEvidence Based Nursing PracticeChithra Saju71% (7)
- Dementia Research ProposalDocument12 pagesDementia Research ProposalOmowunmiItunuNo ratings yet
- Health Assurance Claim FormDocument8 pagesHealth Assurance Claim FormHarmeet MaanNo ratings yet
- Claims FormDocument16 pagesClaims FormPhunsukh WangduNo ratings yet
- Heartbeat Claim Form PDFDocument16 pagesHeartbeat Claim Form PDFAnkitThakkarNo ratings yet
- Vipul Corp TPA PVT LTD.: Details of Insurance HistoryDocument6 pagesVipul Corp TPA PVT LTD.: Details of Insurance HistorybrajendraNo ratings yet
- VMPL - Claim Form (A)Document3 pagesVMPL - Claim Form (A)Rahul RathodNo ratings yet
- Claim Form PDFDocument5 pagesClaim Form PDFmeghaNo ratings yet
- Heartbeat Claim FormDocument8 pagesHeartbeat Claim Formto.animeshsen604No ratings yet
- Claim FormDocument6 pagesClaim Formashu9649No ratings yet
- Reimbursement Claim FormDocument7 pagesReimbursement Claim FormashishladooNo ratings yet
- Claim FormDocument3 pagesClaim FormVediappan Alies RajaNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryChatterjee KushalNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistoryDocument7 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Insurance HistorySwapnil NageNo ratings yet
- Claim Form Part ADocument4 pagesClaim Form Part Ajeparal482No ratings yet
- Aditya Birla Claim Form Part ADocument8 pagesAditya Birla Claim Form Part Astatus addaNo ratings yet
- Claim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part ADocument7 pagesClaim Form For Health Insurance Policies Other Than Travel and Personal Accident - Part Aharmeet singhNo ratings yet
- Max Bupa Claims FormDocument16 pagesMax Bupa Claims FormraviNo ratings yet
- Vipul Corp Lnsurance TPA PVT LTD.: Details of Primary InsuredDocument8 pagesVipul Corp Lnsurance TPA PVT LTD.: Details of Primary InsuredHimansh ChandakNo ratings yet
- Claim Form - HospitalizationDocument8 pagesClaim Form - HospitalizationNishantShah100% (1)
- HDFC ERGO General Insurance Company LimitedDocument6 pagesHDFC ERGO General Insurance Company LimitedShibani DesaiNo ratings yet
- Easy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ADocument6 pagesEasy Ways To Speed Up The Claims Process: Manipalcigna Prohealth Insurance Policy Claim Form ARamesh WalkeNo ratings yet
- Claim Reimbursement FormDocument7 pagesClaim Reimbursement FormBagavathi RNo ratings yet
- Claim Form 10 - EditableDocument9 pagesClaim Form 10 - EditableharshiNo ratings yet
- Claim Form: Claim Form Part A Section A - Details of Primary InsuredDocument8 pagesClaim Form: Claim Form Part A Section A - Details of Primary InsuredAnonymous d8d8k1LiyNo ratings yet
- ReimbursementFormA B2016Document7 pagesReimbursementFormA B2016DESIGN CGMPNo ratings yet
- Claim Form - Part A General InsuranceDocument3 pagesClaim Form - Part A General Insurancejignesh vyasNo ratings yet
- ReimbursementFormA B2016 PDFDocument5 pagesReimbursementFormA B2016 PDFranganathNo ratings yet
- Health Insurance - Claim Form - Part A (To Be Filled by Insured)Document4 pagesHealth Insurance - Claim Form - Part A (To Be Filled by Insured)Shaikh AyyubNo ratings yet
- Health File3Document9 pagesHealth File3kulbirplusNo ratings yet
- HDFC Group Health Insurance - Claim ManualDocument6 pagesHDFC Group Health Insurance - Claim ManualNeir KrNo ratings yet
- ProHealth V7 ClaimFormA April23Document7 pagesProHealth V7 ClaimFormA April23njthakkarNo ratings yet
- E Claim FormDocument8 pagesE Claim FormronNo ratings yet
- Reimbursement Claim FormDocument10 pagesReimbursement Claim FormranjanNo ratings yet
- ProHealth Cash Claim A March2021 V3 V3Document7 pagesProHealth Cash Claim A March2021 V3 V3Harsh MandaniNo ratings yet
- Reimbursement A PDFDocument4 pagesReimbursement A PDFAniruddha ShivalNo ratings yet
- Details of Primary Insured: Bajaj Allianz General Insurance Company LimitedDocument3 pagesDetails of Primary Insured: Bajaj Allianz General Insurance Company LimitedBellapu Durga vara prasadNo ratings yet
- Claim Form GMCDocument7 pagesClaim Form GMCBhaskar RawatNo ratings yet
- EH Claim FormDocument8 pagesEH Claim FormAmol PakhaleNo ratings yet
- ClaimFormDocument6 pagesClaimFormKanhaiya Lal SahuNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyMruthunjaya Reddy LakkamNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance Policyanil sangwanNo ratings yet
- Magma Claim FormDocument4 pagesMagma Claim FormAbhinav JaganaNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicypawanNo ratings yet
- Reimbursement CLaim Form IRDADocument5 pagesReimbursement CLaim Form IRDADhaval ThakkarNo ratings yet
- Reimbursement Claim Form-1Document7 pagesReimbursement Claim Form-1Mayuresh DalviNo ratings yet
- Reimbursement Claim FormDocument4 pagesReimbursement Claim FormhariharanccetNo ratings yet
- Bajaj Claim FormDocument9 pagesBajaj Claim FormYogi’s iphone No ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicyArunsNo ratings yet
- Claim Form - Part A' To 'Claim Form For Health Insurance PolicyDocument6 pagesClaim Form - Part A' To 'Claim Form For Health Insurance PolicySudipta DeNo ratings yet
- 05-01-2022 - Manuj Om HospitalisationDocument20 pages05-01-2022 - Manuj Om HospitalisationManuj RathoreNo ratings yet
- Group Mediprime Claim FormDocument8 pagesGroup Mediprime Claim FormRahulNo ratings yet
- Claim Form - Part A: To Be Filled in by The InsuredDocument2 pagesClaim Form - Part A: To Be Filled in by The InsuredAli ArsalaanNo ratings yet
- Easy Health Insurance Claim Form PDFDocument4 pagesEasy Health Insurance Claim Form PDFAnkithNo ratings yet
- AMHI-new Claim Form PDFDocument4 pagesAMHI-new Claim Form PDFQwerty TNo ratings yet
- To Be Filled in by The Insured: Details of Primary InsuredDocument4 pagesTo Be Filled in by The Insured: Details of Primary Insurednaveen pointNo ratings yet
- Claim Form Part ADocument8 pagesClaim Form Part AJos'fAntonyRinoNo ratings yet
- Disaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsFrom EverandDisaster Dollars: Financial Preparation and Recovery for Towns, Businesses, Farms, and IndividualsNo ratings yet
- Veneer Classification .PDGDocument10 pagesVeneer Classification .PDGAndykaYayanSetiawanNo ratings yet
- The Effects of Auditory Hallucination Symptom ManagementDocument12 pagesThe Effects of Auditory Hallucination Symptom ManagementAndika FahruroziNo ratings yet
- Severe Acute Malnutrition - ManagementDocument14 pagesSevere Acute Malnutrition - ManagementArkadeb Kar100% (1)
- The Benefits of An Ageing PopulationDocument9 pagesThe Benefits of An Ageing PopulationYa LiNo ratings yet
- ASA PS Classifications From The American Society of AnesthesiologistsDocument1 pageASA PS Classifications From The American Society of AnesthesiologistsaffifulichwanNo ratings yet
- Retail Sale Drugs License AFFIDAVITDocument40 pagesRetail Sale Drugs License AFFIDAVITIndranil DattaNo ratings yet
- NCD Project: Togu Marpaung, MDDocument11 pagesNCD Project: Togu Marpaung, MDTogu MarpaungNo ratings yet
- Healthcare Predictive Analytics Using Machine Learning and Deep Learning Techniques: A SurveyDocument45 pagesHealthcare Predictive Analytics Using Machine Learning and Deep Learning Techniques: A SurveyMuhammad Sadiq Khan NasarNo ratings yet
- LEGASPI Nomination Papers For PGH Directorship (2015)Document6 pagesLEGASPI Nomination Papers For PGH Directorship (2015)karl_poorNo ratings yet
- Narrative ReportDocument3 pagesNarrative ReportCamille De PaduaNo ratings yet
- Test Bank For Mosbys Textbook For Nursing Assistants 9th Edition by SorrentinoDocument11 pagesTest Bank For Mosbys Textbook For Nursing Assistants 9th Edition by Sorrentinodiodontmetacism.0jw2al100% (46)
- National Mediclaim Policy PDFDocument19 pagesNational Mediclaim Policy PDFTanmoy Pal ChowdhuryNo ratings yet
- NTB ppt-1Document76 pagesNTB ppt-1yazgariNo ratings yet
- Updated Resume 11 19Document2 pagesUpdated Resume 11 19api-454845978No ratings yet
- Cuong Vong - Resume - RevisedDocument2 pagesCuong Vong - Resume - Revisedapi-300295160No ratings yet
- Spirituality, Religion and Mental IllnessDocument9 pagesSpirituality, Religion and Mental IllnessJericho CabelloNo ratings yet
- Tamayo - History of Psychiatric NursingDocument1 pageTamayo - History of Psychiatric NursingVictoria Castillo TamayoNo ratings yet
- Patient History Taking TemplateDocument2 pagesPatient History Taking TemplateVarshini Tamil SelvanNo ratings yet
- Nurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanDocument5 pagesNurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement Planzadem5266No ratings yet
- SC DHEC Infant Mortality Rate ReportDocument40 pagesSC DHEC Infant Mortality Rate ReportABC15 NewsNo ratings yet
- Sreevidya Nair - PresentationDocument16 pagesSreevidya Nair - PresentationArk GroupNo ratings yet
- Organizational StructureDocument61 pagesOrganizational Structuretahira ahmedNo ratings yet
- Myanmar LNGO Directory 2012Document138 pagesMyanmar LNGO Directory 2012kk_mangneo100% (1)
- Family Names of DrugsDocument1 pageFamily Names of DrugsangelNo ratings yet
- Abhijeet Singh Ankit Kr. Agrawal (3C) Vaibhav Gupta Pankul Gupta Prateek MittalDocument13 pagesAbhijeet Singh Ankit Kr. Agrawal (3C) Vaibhav Gupta Pankul Gupta Prateek MittalAbhijeet SinghNo ratings yet
- Tanzania National Strategic Plan For The Control of Viral Hepatitis 2018-19-2022-23Document72 pagesTanzania National Strategic Plan For The Control of Viral Hepatitis 2018-19-2022-23daniel mwanduNo ratings yet
- NCMA113 FUNDA SKILL 2 Donning Doffing PPEsDocument4 pagesNCMA113 FUNDA SKILL 2 Donning Doffing PPEsJessoliver GalvezNo ratings yet