Download as pdf or txt
You might also like
- DIY MAP Your Soul Plan Chart: T/DR Markus Van Der WesthuizenDocument14 pagesDIY MAP Your Soul Plan Chart: T/DR Markus Van Der WesthuizenValentin Mihai100% (4)
- Chess Lesson Plan NewDocument3 pagesChess Lesson Plan NewJhen Mendoza100% (3)
- Fonc 11 599243Document7 pagesFonc 11 599243Faki D'pasnizerNo ratings yet
- Development and Validation of The Oral Mucositis Risk Assessment Scale in Hematology PatientsDocument6 pagesDevelopment and Validation of The Oral Mucositis Risk Assessment Scale in Hematology PatientsPaola GilNo ratings yet
- Policy On Pediatric Dental Pain ManagementDocument3 pagesPolicy On Pediatric Dental Pain ManagementمعتزباللهNo ratings yet
- Charalambous2018 OkDocument9 pagesCharalambous2018 Okdayana nopridaNo ratings yet
- 10.1007@s40368 017 0290 Z 3Document6 pages10.1007@s40368 017 0290 Z 3andi winayaNo ratings yet
- Meta-Analysis of Randomized Controlled Trials of The Efficacy of Propolis Mouthwash in Cancer Therapy-Induced Oral MucositisDocument9 pagesMeta-Analysis of Randomized Controlled Trials of The Efficacy of Propolis Mouthwash in Cancer Therapy-Induced Oral MucositisandikaisnaeniNo ratings yet
- Honey and A Mixture of Honey, Beeswax, and OliveDocument9 pagesHoney and A Mixture of Honey, Beeswax, and OlivecarolineNo ratings yet
- Ariffin 2020Document6 pagesAriffin 2020Parminderpal SinghNo ratings yet
- SCCM Clinical - Practice - Guideline Safe Medication Use in ICUDocument6 pagesSCCM Clinical - Practice - Guideline Safe Medication Use in ICULuciana OliveiraNo ratings yet
- BrazilDocument7 pagesBrazilkarinagitakNo ratings yet
- Family Support and Self-Esteem of Patient With Breast CancerDocument5 pagesFamily Support and Self-Esteem of Patient With Breast CancerDean Rex Azriel TelaumbanuaNo ratings yet
- Journal of The American Academy of Pediatrics, Valuing Reduced Antibiotic Use For OMADocument7 pagesJournal of The American Academy of Pediatrics, Valuing Reduced Antibiotic Use For OMARaymond PNo ratings yet
- VitaminaD y AlergiaDocument12 pagesVitaminaD y AlergiaJorge Eneas DosoliNo ratings yet
- AAPD Caries Risk Management For InfantsDocument9 pagesAAPD Caries Risk Management For InfantsDulce MartinezNo ratings yet
- MagicMouthwash For OralMucositis Sol Stanford PDFDocument2 pagesMagicMouthwash For OralMucositis Sol Stanford PDFManuel ArenasNo ratings yet
- Oral CryotherapyDocument16 pagesOral CryotherapyDemilyadioppy AbevitNo ratings yet
- Development of A Stable Oral Pediatric Solution of Hydrochlorothiazide by The Combined Use of Cyclodextrins and Hydrophilic PolymersDocument9 pagesDevelopment of A Stable Oral Pediatric Solution of Hydrochlorothiazide by The Combined Use of Cyclodextrins and Hydrophilic PolymersAntony Joel Meza LoardoNo ratings yet
- Kesalahan Obat Di Arab SaudiDocument8 pagesKesalahan Obat Di Arab SaudiEnggar Ardiani TagapNo ratings yet
- Yeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisDocument9 pagesYeung H Et Al 2012. Patient Reported Reasons For The Discontinuation of Commonly Used Treatments For Moderate To Severe PsoriasisAndi MarsaliNo ratings yet
- Role of Taste Perception in WSL Formation During Orthodontic TreatmentDocument6 pagesRole of Taste Perception in WSL Formation During Orthodontic TreatmentShreya JohnNo ratings yet
- Periodontology 2000 - 2019 - Beck - Advances in Precision Oral HealthDocument18 pagesPeriodontology 2000 - 2019 - Beck - Advances in Precision Oral HealthAdil KaukabNo ratings yet
- 29 110 3 PBDocument9 pages29 110 3 PBWidia WidanaNo ratings yet
- Original Article: AbstractDocument3 pagesOriginal Article: Abstractyohanes22No ratings yet
- Part 1 InglesDocument8 pagesPart 1 InglesAlondraNo ratings yet
- Acad Dermatol Venereol - 2021 - Thormann - Position Statement On The Role of Nurses in Therapeutic Patient Education inDocument6 pagesAcad Dermatol Venereol - 2021 - Thormann - Position Statement On The Role of Nurses in Therapeutic Patient Education inmaituuyen1997No ratings yet
- BJOG - 2022 - Weelden - The Effect of Progestin Therapy in Advanced and Recurrent Endometrial Cancer A Systematic ReviewDocument10 pagesBJOG - 2022 - Weelden - The Effect of Progestin Therapy in Advanced and Recurrent Endometrial Cancer A Systematic ReviewAnonymous l6Q1ROq2No ratings yet
- 1 s2.0 S1319016421001407 MainDocument8 pages1 s2.0 S1319016421001407 MainarafathNo ratings yet
- Dental Care Throughout Pregnancy: Do's and Don'tsDocument3 pagesDental Care Throughout Pregnancy: Do's and Don'tsdrzana78No ratings yet
- Review Article: Fertility Preservation in GirlsDocument10 pagesReview Article: Fertility Preservation in GirlsAndri Adma WijayaNo ratings yet
- Prenatal Diagnosis - 2021 - Spencer - Development of Standard Definitions and Grading For Maternal and Fetal Adverse EventDocument12 pagesPrenatal Diagnosis - 2021 - Spencer - Development of Standard Definitions and Grading For Maternal and Fetal Adverse Eventtriska antonyNo ratings yet
- Honey Wounds CancerDocument6 pagesHoney Wounds CancerburhanNo ratings yet
- Journal of Pediatric Nursing Volume Issue 2019 (Doi 10.1016 - J.pedn.2019.02.001) Konuk Sener, Dilek Aydin, Meryem Cangur, Sengul Guven, Evren - The Effect of Oral Care With Chlorhexidine, Vitamin PDFDocument7 pagesJournal of Pediatric Nursing Volume Issue 2019 (Doi 10.1016 - J.pedn.2019.02.001) Konuk Sener, Dilek Aydin, Meryem Cangur, Sengul Guven, Evren - The Effect of Oral Care With Chlorhexidine, Vitamin PDFNovia WiyantiNo ratings yet
- PIIS0190962223028785Document14 pagesPIIS0190962223028785niidea7No ratings yet
- Bouberhan (2019)Document5 pagesBouberhan (2019)Aprilla Ayu WulandariNo ratings yet
- Use of Therapeutic Laser For Prevention and Treatment of Oral MucositisDocument6 pagesUse of Therapeutic Laser For Prevention and Treatment of Oral Mucositishendra ardiantoNo ratings yet
- Pregnancy CAM TurkeyDocument10 pagesPregnancy CAM TurkeyTuğba ÖzcanNo ratings yet
- sẩy thai liên tiếp thrombophiliaDocument28 pagessẩy thai liên tiếp thrombophiliahthoailocNo ratings yet
- Aust J Dermatology - 2023 - AcneDocument4 pagesAust J Dermatology - 2023 - Acnesara3elena3manolacheNo ratings yet
- Antibióticos y EndodonciaDocument8 pagesAntibióticos y EndodonciaPaola AndreaNo ratings yet
- British Society For Rheumatology Guideline On Prescribing Drugs in Pregnancy and Breastfeeding Immunomodulatory Anti-Rheumatic Drugs and CorticosteroidsDocument41 pagesBritish Society For Rheumatology Guideline On Prescribing Drugs in Pregnancy and Breastfeeding Immunomodulatory Anti-Rheumatic Drugs and CorticosteroidsKori Karina Cueva TovarNo ratings yet
- Saudi Pharmaceutical Journal: Original ArticleDocument5 pagesSaudi Pharmaceutical Journal: Original ArticleDicky CaritoNo ratings yet
- Reproductive Health Guideline Final 2020Document28 pagesReproductive Health Guideline Final 2020MilenaNo ratings yet
- Of Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionDocument7 pagesOf Antimicrobial Resistance: The Who Aware (Access, Watch, Reserve) Antibiotic Book and PreventionBBD BBDNo ratings yet
- Safe Handling of Oral Chemotherapeutic Agents Among Nurses in Oncology UnitsDocument14 pagesSafe Handling of Oral Chemotherapeutic Agents Among Nurses in Oncology Unitseditorial.boardNo ratings yet
- Novel Strategies For The Bioavailability Augmentation and Efficacy Improvement of Natural Products in Oral Cancer PDFDocument30 pagesNovel Strategies For The Bioavailability Augmentation and Efficacy Improvement of Natural Products in Oral Cancer PDFNourhan AbdalkaderNo ratings yet
- 2023 - Leche y Riesgo de 12 Cáncer @lumsdenDocument8 pages2023 - Leche y Riesgo de 12 Cáncer @lumsdenJorge Toshio Yazawa ChaconNo ratings yet
- 3920 B 20 XavierDocument7 pages3920 B 20 Xavierكرار حيدر وهيبNo ratings yet
- 11 ArticuloDocument9 pages11 ArticuloNia MoonNo ratings yet
- Intensive & Critical Care Nursing: Research ArticleDocument6 pagesIntensive & Critical Care Nursing: Research ArticleJaemin cuteNo ratings yet
- Burden of Family Caregivers of Patients With Oral Cancer in Home Care in TaiwanDocument11 pagesBurden of Family Caregivers of Patients With Oral Cancer in Home Care in Taiwansofia limaNo ratings yet
- Comparison of Malnutrition and Malnutrition Screening Tools in Pediatric Oncology Patients A Cross-Sectional StudyDocument5 pagesComparison of Malnutrition and Malnutrition Screening Tools in Pediatric Oncology Patients A Cross-Sectional StudySebastian MarinNo ratings yet
- Detecting Severe Acute Malnutrition in Children Under Five at Scale: The Challenges of Anthropometry To Reach The Missed MillionsDocument5 pagesDetecting Severe Acute Malnutrition in Children Under Five at Scale: The Challenges of Anthropometry To Reach The Missed MillionsaudriNo ratings yet
- The Role of PK/PD Analysis in The Development and Evaluation of AntimicrobialsDocument29 pagesThe Role of PK/PD Analysis in The Development and Evaluation of AntimicrobialsdrnguyenbvtkNo ratings yet
- 2020 American College of Rheumatology Guideline For The Management of Reproductive Health in Rheumatic and Musculoskeletal DiseasesDocument28 pages2020 American College of Rheumatology Guideline For The Management of Reproductive Health in Rheumatic and Musculoskeletal Diseasessanty ayu puspita perdhanaNo ratings yet
- Periodontology 2000 - 2023 - Herrera - Europe S Contribution To The Evaluation of The Use of Systemic Antimicrobials in TheDocument28 pagesPeriodontology 2000 - 2023 - Herrera - Europe S Contribution To The Evaluation of The Use of Systemic Antimicrobials in TheEngku Ahmad MuzhaffarNo ratings yet
- Caries Activity TestDocument19 pagesCaries Activity TestArizona GreyNo ratings yet
- Effect of Oral Cryotherapy in Preventing Chemotherapy Induced Oral Stomatitis Among Childhood Acute Lymphoblastic LeukemiaDocument10 pagesEffect of Oral Cryotherapy in Preventing Chemotherapy Induced Oral Stomatitis Among Childhood Acute Lymphoblastic LeukemiaIjahss JournalNo ratings yet
- PNL Issue 14 A2022Document5 pagesPNL Issue 14 A2022RPH gulzaibNo ratings yet
- Baseline Caries Risk Assessment As A Predictor of Caries IncidenceDocument7 pagesBaseline Caries Risk Assessment As A Predictor of Caries IncidenceAvina Anin NasiaNo ratings yet
- Cultural Practices and DermatosesFrom EverandCultural Practices and DermatosesNeelam A. VashiNo ratings yet
- Wilcom EmroiWilcom Embroidery Software Learning Tutorial in HindiDocument10 pagesWilcom EmroiWilcom Embroidery Software Learning Tutorial in HindiGuillermo RosasNo ratings yet
- Nurses Bill of RightsDocument1 pageNurses Bill of RightsFlauros Ryu Jabien100% (1)
- Learning Skill For 21ST CenturyDocument16 pagesLearning Skill For 21ST CenturyKSSNo ratings yet
- EXERCIZIO 1 ARCHI - ScoreDocument7 pagesEXERCIZIO 1 ARCHI - ScoreFranco PerloNo ratings yet
- Deloitte Au Tech Marathon Case Study 171215Document2 pagesDeloitte Au Tech Marathon Case Study 171215shivangiNo ratings yet
- Art 20199983Document3 pagesArt 20199983Devaki SubasriNo ratings yet
- Assignment of Kesavananda Bharti V State of KeralaDocument17 pagesAssignment of Kesavananda Bharti V State of KeralaFarjana Akter67% (3)
- Design Thinking: Secure Car ParkDocument12 pagesDesign Thinking: Secure Car ParkSiddhesh JadhavNo ratings yet
- Alls Well That Ends WellDocument31 pagesAlls Well That Ends WellGAREN100% (2)
- English Hots 1Document69 pagesEnglish Hots 1Aswin Shriram UmaThiagarajanNo ratings yet
- Taxation of Cross Border ActivitiesDocument5 pagesTaxation of Cross Border ActivitiesTriila manillaNo ratings yet
- Chapter 20-52-00, 201 Chapter 20-53-00, 201: Table 601. Tools/Equipment and Recommended MaterialsDocument1 pageChapter 20-52-00, 201 Chapter 20-53-00, 201: Table 601. Tools/Equipment and Recommended Materialsianmcnultywork83No ratings yet
- TI Manual SJX Elevator-2Document11 pagesTI Manual SJX Elevator-2Alex MillerNo ratings yet
- Banners of The Insurgent Army of N. Makhno 1918-1921Document10 pagesBanners of The Insurgent Army of N. Makhno 1918-1921Malcolm ArchibaldNo ratings yet
- Ecofeminism Perspective - A Gendered Approach in Reducing Poverty by Implementing Sustainable Development Practices in IndonesiaDocument20 pagesEcofeminism Perspective - A Gendered Approach in Reducing Poverty by Implementing Sustainable Development Practices in IndonesiaM. NaQviNo ratings yet
- Tesla Manufacturing Plant in Canada AnnouncementDocument1 pageTesla Manufacturing Plant in Canada AnnouncementMaria MeranoNo ratings yet
- 3 Year - V - Sem - FinalDocument208 pages3 Year - V - Sem - FinalKARTHIK ANo ratings yet
- Dahua HD IR Vari Focal Dome Network Camera Quick Start Guide (Web 3 - 0) V1 - 0 - 1 - 20171106Document19 pagesDahua HD IR Vari Focal Dome Network Camera Quick Start Guide (Web 3 - 0) V1 - 0 - 1 - 20171106jori ahuefafreeNo ratings yet
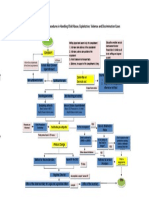
- Rules and Procedures in Handling Child Abuse CasesDocument1 pageRules and Procedures in Handling Child Abuse CasesJoyce Carreon50% (2)
- MicroChannel HeatExchangersDocument16 pagesMicroChannel HeatExchangerskhushal bhanderiNo ratings yet
- TFWP 2022q4 Pos enDocument1,088 pagesTFWP 2022q4 Pos enMuhammad NaqashNo ratings yet
- Kerala Agricultural University: Main Campus, Vellanikkara, Thrissur - 680 656, KeralaDocument3 pagesKerala Agricultural University: Main Campus, Vellanikkara, Thrissur - 680 656, KeralaAyyoobNo ratings yet
- Internship Cover LetterDocument7 pagesInternship Cover LetterIeqa HaziqahNo ratings yet
- Death and The AfterlifeDocument2 pagesDeath and The AfterlifeAdityaNandanNo ratings yet
- Management Unit 5 MCQDocument4 pagesManagement Unit 5 MCQPranav MhatreNo ratings yet
- Reading PracticeDocument1 pageReading Practicejemimahluyando8No ratings yet
- Corrected First Set of Admissions Us Bank ADJUST TO YOUR BANK PLAINTIFFDocument13 pagesCorrected First Set of Admissions Us Bank ADJUST TO YOUR BANK PLAINTIFF1SantaFean100% (1)
- Demonstrating The Social Construction of RaceDocument7 pagesDemonstrating The Social Construction of RaceThomas CockcroftNo ratings yet